Eras protocol
Reading File
Finding Sources
Searching PubMed
"enhanced recovery after surgery" ERAS protocol
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of the Enhanced Recovery After Surgery (ERAS) Protocol:
Enhanced Recovery After Surgery (ERAS)
What Is ERAS?
ERAS is a multimodal, evidence-based perioperative care program designed to reduce surgical stress, accelerate recovery, and improve outcomes. It was pioneered by Henrik Kehlet (Denmark) in the 1990s and formalized as a group protocol in 2001 by Fearon, Ljungqvist, and colleagues. The first consensus guideline—for colonic resection—was published in 2005. The ERAS® Society (erasociety.org) now publishes guidelines across >20 surgical specialties.
The key philosophy: target quality of recovery, not just speed. ERAS bundles address systemic inflammation, the catabolic stress response, fluid balance, anemia, PONV, and pain through a multidisciplinary, multimodal approach.
Core Elements of ERAS
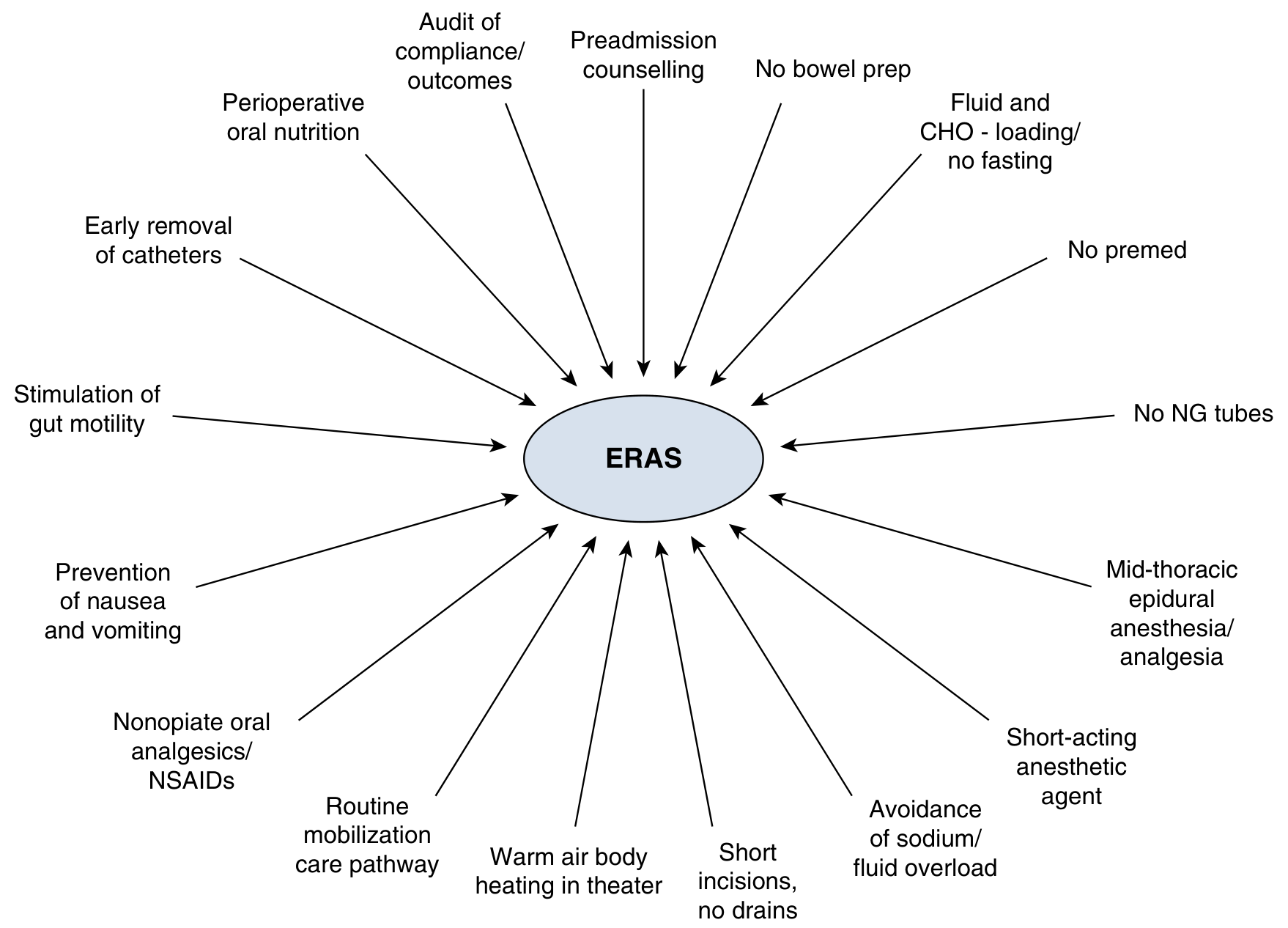
The elements are organized across three phases:
Preoperative
| Element | Rationale |
|---|---|
| Preadmission counseling | Reduces anxiety; sets expectations |
| No routine bowel prep | No outcome benefit; causes dehydration |
| No routine premedication (sedatives) | Prevents delayed awakening and immobility |
| Carbohydrate (CHO) loading / no prolonged fasting | Attenuates insulin resistance; reduces catabolism |
| Prehabilitation (exercise, nutrition optimization) | Optimizes functional reserve before surgery |
| Manage comorbidities (diabetes, anemia, malnutrition) | Reduces surgical risk |
Intraoperative
| Element | Rationale |
|---|---|
| Short-acting anesthetic agents | Faster emergence; earlier mobilization |
| Mid-thoracic epidural anesthesia/analgesia (for open abdominal) | Superior pain control, reduces ileus |
| Opioid-sparing multimodal analgesia | Reduces opioid side effects (ileus, nausea, sedation) |
| Avoidance of sodium and fluid overload | Prevents edema and delayed gut recovery |
| Warm air body heating | Prevents hypothermia-related complications |
| Short incisions, minimal drains | Reduces pain; enables earlier mobility |
| No routine NG tubes | No proven benefit; impairs eating and mobility |
Postoperative
| Element | Rationale |
|---|---|
| Prevention of PONV (multimodal antiemetics) | Enables early oral intake |
| Perioperative oral nutrition (early feeding) | Reduces catabolism; supports wound healing |
| Stimulation of gut motility (gum chewing, laxatives, etc.) | Reduces postoperative ileus |
| Early mobilization (routine mobilization care pathway) | Prevents muscle loss, DVT, pulmonary complications |
| Early removal of catheters and drains | Enables mobility; reduces infection risk |
| Audit of compliance and outcomes | Essential feedback loop for continuous improvement |
ERAS Implementation Program (EIP)
A formal EIP requires three components:
- ERAS Protocol — evidence-based care bundle customized to the surgical specialty
- Audit System — tracks protocol compliance AND outcomes (at minimum: LOS and complications). The ERAS® Society offers an interactive audit tool at erasociety.org/interactive-audit
- Multidisciplinary ERAS Team — includes surgeon, anesthesiologist, nursing (preop clinic, OR, ward), pharmacy, dietitian, physiotherapy, occupational therapy, and a manager
Dose-response relationship: Increasing ERAS compliance is directly associated with fewer complications and shorter LOS. Each unit increase in ERAS guideline score correlates with an 8–12% decrease in hospital days (Wijk et al., >2000 patients).
Outcomes and Evidence
- Reduces length of stay significantly (e.g., colorectal surgery from ~2 weeks → 2 days in early series)
- Reduces complication rates and readmissions
- Reduces opioid consumption
- Applicable to ambulatory surgery with modified protocols (opioid minimization framework)
- ERAS Society guidelines cited >11,000 times, downloaded >700,000 times
- Evidence graded using GRADE (strong vs. weak recommendation; high/moderate/low/very low quality)
ERAS by Specialty
The ERAS Society has published guidelines for colorectal, pancreatic, hepatic, esophageal, gastric, gynecologic/oncologic, urologic (radical cystectomy), cardiac, thoracic, orthopedic, bariatric, and other procedures—with ongoing expansion to low- and middle-income countries.
Sources:
- Sabiston Textbook of Surgery, 21st ed. — Chapter 22 (Ljungqvist, de Boer, Nelson)
- Miller's Anesthesia, 10th ed. — Chapters on ambulatory and urologic ERAS
This is a shared conversation. Sign in to Orris to start your own chat.