Pain pathway dental student oral surgery
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have rich, comprehensive material. Let me compile the full answer.
Pain Pathway - Dental Student / Oral Surgery Guide
This is a complete overview of the pain pathway as it applies to oral surgery, from the receptor level to the cortex, with emphasis on the trigeminal system.
1. The Peripheral Nociceptor - Where Pain Begins
Fiber Types
| Fiber | Myelination | Diameter | Conduction | Pain Quality |
|---|---|---|---|---|
| Aβ | Heavily myelinated | Large | Fast | Touch/proprioception - NOT pain in normal tissue |
| Aδ | Thinly myelinated | Small | 5-30 m/s | Sharp, well-localized, "first pain" - e.g., the initial prick of a needle |
| C | Unmyelinated | Smallest | 0.5-2 m/s | Dull, burning, aching, "second pain" - e.g., the throbbing after extraction |
The cell bodies of all primary sensory afferents lie in the trigeminal ganglion (= the cranial equivalent of the dorsal root ganglion). From there, one branch projects centrally into the brainstem and one branch projects peripherally to innervate teeth, periodontium, mucosa, bone, and muscles of mastication.
The ability to detect painful stimuli is completely abolished when conduction in Aδ and C fibers is blocked - this is exactly what local anesthetics achieve. - Harrison's Principles of Internal Medicine 22E
What Activates Nociceptors?
Individual nociceptors can respond to multiple stimulus types:
- Mechanical - pressure, drilling, extraction forces
- Thermal - heat/cold (tooth sensitivity)
- Chemical - low pH, bradykinin (BK), ATP, serotonin, histamine, prostaglandins
- TRPV1 receptor - activated by heat, acidic pH, and capsaicin
2. Sensitization - Clinically Critical in Oral Surgery
Peripheral Sensitization
When tissues are damaged or inflamed (e.g., periapical abscess, post-extraction socket, periodontal disease):
- Inflammatory mediators (BK, nerve growth factor, prostaglandins, leukotrienes) lower the activation threshold of nociceptors
- This is why a tooth with irreversible pulpitis may require more local anesthetic - the nociceptors are already in a hyper-excited state
- This is also why NSAIDs (which block prostaglandin synthesis) are effective pre-emptive analgesics
Central Sensitization
- Sustained nociceptor activity enhances the excitability of neurons in the spinal trigeminal nucleus (the brainstem equivalent of the dorsal horn)
- Leads to allodynia (normally innocuous stimuli cause pain - e.g., air puff on an exposed dentinal tubule)
- Leads to hyperalgesia (exaggerated response to a painful stimulus)
Neurogenic Inflammation
Primary afferent nociceptors are not passive messengers. When activated they release neuropeptides from their peripheral terminals:
- Substance P - potent vasodilator, causes mast cell degranulation, contributes to the inflammatory flare response
- CGRP (calcitonin gene-related peptide) - vasodilation, edema This is the basis of neurogenic inflammation seen around inflamed dental pulp and extraction sockets.
3. The Central Pain Pathway - From Periphery to Cortex
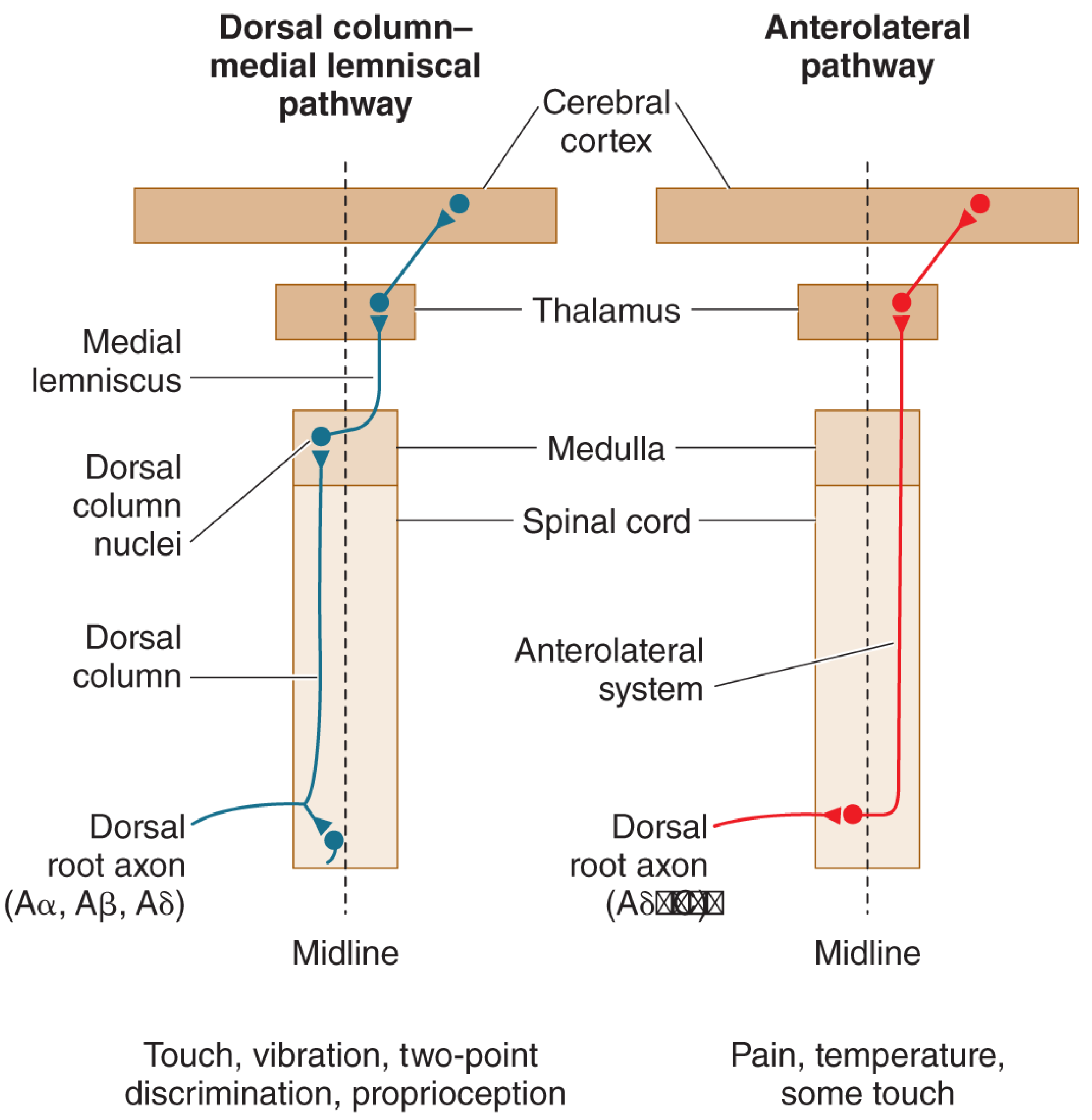
For the Body (spinal pathway):
- 1st-order neuron: Aδ/C fibers enter dorsal horn → synapse in Rexed laminae I and II (substantia gelatinosa)
- 2nd-order neuron: crosses the midline → ascends in the anterolateral/spinothalamic tract
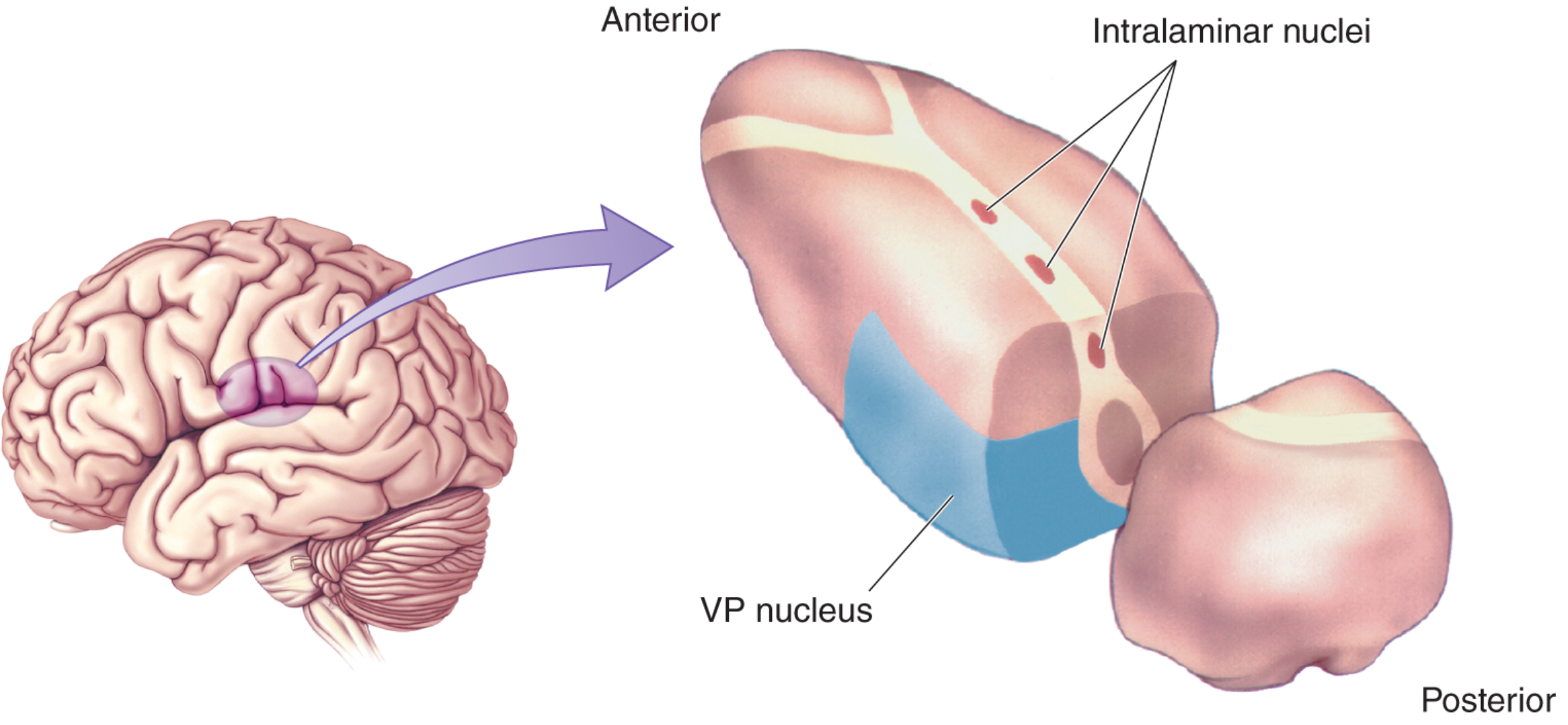
- 3rd-order neuron: thalamus (VP nucleus + intralaminar nuclei) → somatosensory cortex
The Trigeminal Pain Pathway (face and teeth):
This is the anatomically unique path relevant to oral surgery:
-
1st-order neuron: Aδ/C fibers travel in branches of the trigeminal nerve (CN V):
- V1 (ophthalmic) - orbit, forehead, nose
- V2 (maxillary) - upper teeth, maxillary sinus, palate, cheek
- V3 (mandibular) - lower teeth, mandible, tongue, muscles of mastication
- Cell bodies in the trigeminal (semilunar/Gasserian) ganglion
-
1st synapse: Small-diameter fibers synapse on 2nd-order neurons in the spinal trigeminal nucleus of the brainstem. This nucleus is essentially a caudal extension of the substantia gelatinosa of the spinal cord, stretching from the pons down to C2-C3. This explains why dental pain can sometimes be referred to the neck.
-
2nd-order neuron: Axons cross the midline and ascend to the thalamus in the trigeminal lemniscus (the cranial equivalent of the spinothalamic tract)
-
Thalamus: Pain signals terminate in the ventral posterior (VP) nucleus and the intralaminar nuclei
-
Cortex: Projects to somatosensory cortex (conscious perception), prefrontal and cingulate cortex (emotional/suffering component)
4. Pain Modulation - The Gate Control Theory
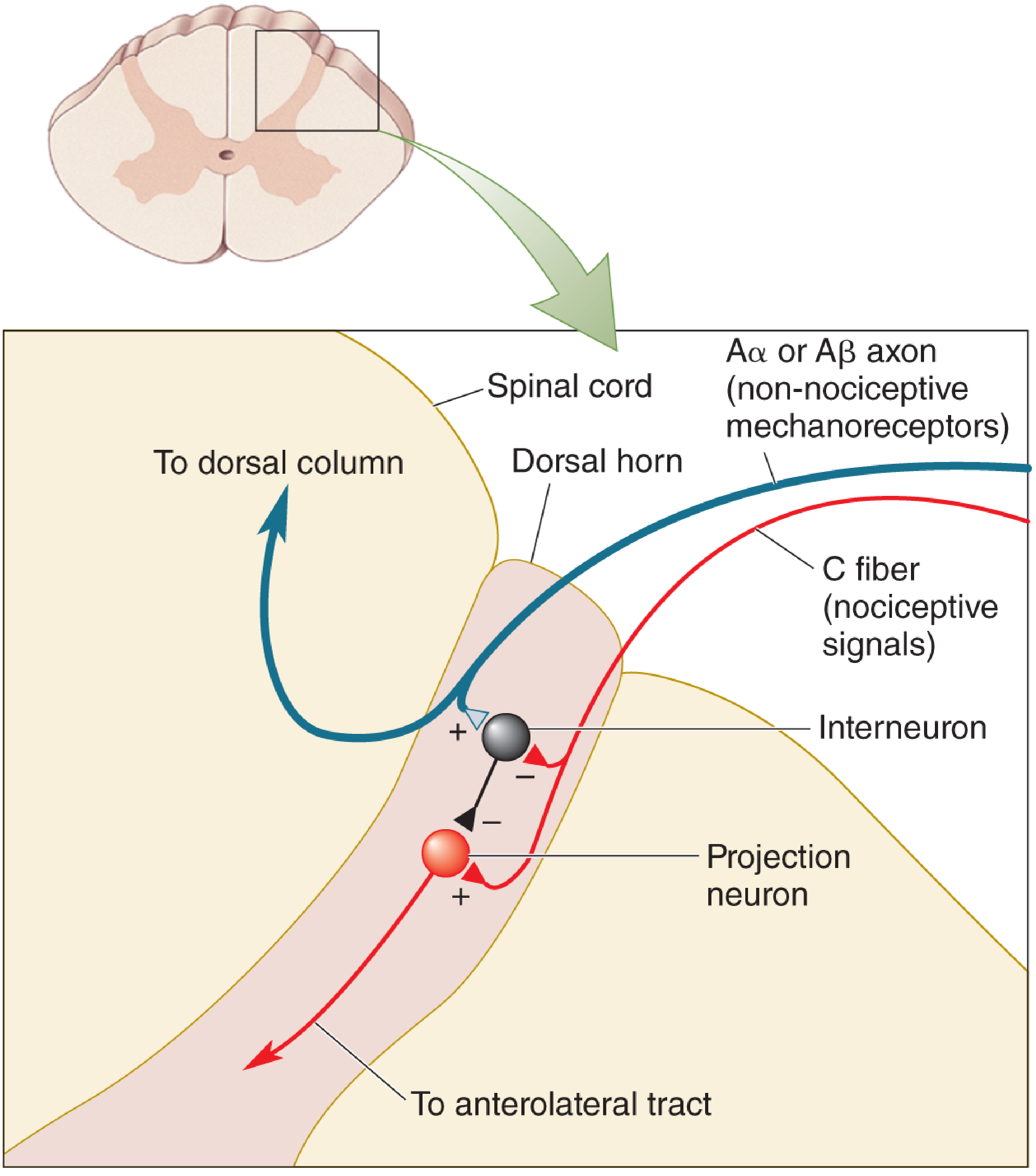
Proposed by Melzack and Wall (1965):
- Dorsal horn projection neurons receive input from both large Aβ fibers and small Aδ/C nociceptive fibers
- When Aβ fibers fire (rubbing, TENS stimulation), inhibitory interneurons are activated → reduce the ability of C fibers to excite the projection neuron
- Clinical application: TENS (transcutaneous electrical nerve stimulation) uses this mechanism for chronic pain relief
Descending Modulation
- The brain also sends signals downward to modulate incoming pain
- The periaqueductal gray (PAG) and raphe nuclei release endogenous opioids (endorphins, enkephalins) and serotonin at the dorsal horn/spinal trigeminal nucleus
- This is the basis of opioid analgesia and why emotional state affects pain perception
5. Clinical Relevance for Oral Surgery
| Mechanism | Clinical Implication |
|---|---|
| Aδ fibers carry "first pain" | Sharp, well-localized pain helps patient identify the tooth |
| C fibers carry "second pain" | Dull, throbbing ache after procedure - managed by NSAIDs and analgesics |
| Peripheral sensitization | Inflamed pulps require higher LA doses; pre-emptive analgesia with NSAIDs reduces sensitization before surgery |
| Trigeminal ganglion location | V2 (infraorbital) and V3 (inferior alveolar / mental) nerve blocks work at this level |
| Spinal trigeminal nucleus extends to C2-C3 | Explains referred dental pain to the ear, neck, or temple |
| Neurogenic inflammation | Substance P and CGRP from activated nociceptors worsen post-op edema; corticosteroids can reduce this |
| Central sensitization | Explains why untreated acute pulpitis can become chronic pain - early and adequate analgesia prevents central sensitization |
| Gate control | Rubbing the injection site before giving LA may reduce needle pain; TENS for chronic orofacial pain |
6. Local Anesthetics - How They Interrupt the Pathway
Local anesthetics (e.g., lidocaine, articaine, bupivacaine) work by blocking voltage-gated sodium channels on the axon membrane, preventing action potential propagation:
- Affect smaller fibers preferentially (C > Aδ > Aβ) at lower concentrations - this is why pain is blocked before touch
- Block is use-dependent - more effective on rapidly firing (sensitized) fibers
- Inflamed tissue is more acidic, which shifts the LA equilibrium toward the ionized (active) form - but the ionized form cannot cross the nerve membrane as easily, explaining why LA is less effective in infected/inflamed tissue
Sources: Harrison's Principles of Internal Medicine 22E, p. 137-140 | Neuroscience: Exploring the Brain, 5th Ed., p. 1211-1215 | Barash Clinical Anesthesia 9e, pp. 1153-1257
This is a shared conversation. Sign in to Orris to start your own chat.