Enlarged prostate
Reading File
Finding Sources
Searching PubMed
"benign prostatic hyperplasia"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching PubMed
"benign prostatic hyperplasia" AND "alpha blockers" AND "5-alpha reductase"
I now have comprehensive information from multiple authoritative textbooks. Here is the full answer:
Benign Prostatic Hyperplasia (BPH) - Enlarged Prostate
What Is It?
Benign prostatic hyperplasia (BPH) is the most common benign disease of the prostate in men over 50. It involves nodular proliferation of both stromal and glandular elements in the prostate's transitional zone - the region that directly surrounds the urethra. The prostate normally weighs about 20 g in young men and grows to an average of 24-38 mL between ages 50-80. In BPH, the volume exceeds 30 mL, and the gland can reach 60-100 g (3- to 5-fold normal weight) or more.
- Robbins & Kumar Basic Pathology, p. 659
- Goldman-Cecil Medicine, p. 1316
Epidemiology
| Age Group | Histologic BPH | Symptomatic BPH |
|---|---|---|
| >50 years | ~50% | ~25% |
| 60-69 years | ~70% | Variable |
| 80s | ~90% | ~50% develop notable LUTS |
Age is the single greatest risk factor. Lower urinary tract symptoms (LUTS) increase in a linear fashion between ages 40 and 80. - Goldman-Cecil Medicine, p. 1316
Pathogenesis
The key driver is dihydrotestosterone (DHT):
- Testosterone circulates in the blood and enters the prostate
- The enzyme 5α-reductase type 2 converts testosterone → DHT within prostatic tissue
- DHT is 10× more potent than testosterone; it binds nuclear androgen receptors
- DHT-driven growth factors increase stromal cell proliferation and decrease epithelial cell apoptosis
- With aging, testosterone declines but estrogen levels remain (or rise via peripheral conversion); estrogens may act synergistically with DHT through estrogen receptors on both stromal and epithelial cells
BPH does NOT occur in men castrated before puberty or those with genetic androgen-pathway defects. - Robbins & Kumar, p. 659
Anatomy of Enlargement
BPH originates in the periurethral transition zone, unlike prostate cancer which arises in the peripheral zone. As the nodules grow, they compress the urethra to a slit-like orifice and may push upward into the bladder base.
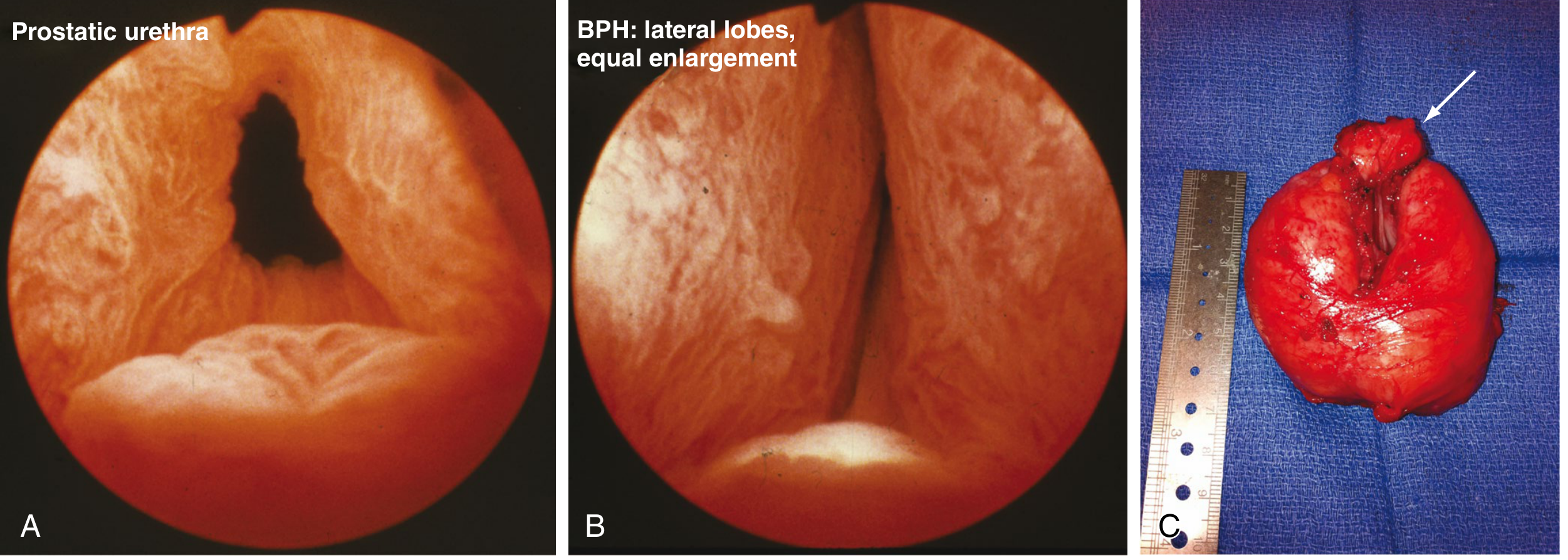
Figure: (A) Normal cystoscopic appearance; (B) Moderate BPH - lateral lobe enlargement compressing the urethral lumen; (C) Surgical specimen (130 g) after open prostatectomy. - Sabiston Textbook of Surgery
Pathology (Microscopy)
- Nodules contain variable proportions of glands and fibromuscular stroma
- Hyperplastic glands are lined by two cell layers: tall inner columnar cells + outer flattened basal cells (this two-layer pattern distinguishes BPH from carcinoma, which loses the basal cell layer)
- Glandular lumina may contain corpora amylacea (laminated proteinaceous secretory material)
- Robbins & Kumar, p. 659
Symptoms (LUTS)
BPH causes lower urinary tract symptoms through two mechanisms:
- Mechanical obstruction - the enlarged gland physically narrows the urethra
- Dynamic obstruction - increased smooth muscle tone in the stroma (α1-adrenergic receptors)
Symptoms are classified as:
| Category | Symptoms |
|---|---|
| Storage | Urinary frequency, urgency, nocturia |
| Voiding | Hesitancy, poor stream, straining, intermittency |
| Post-void | Incomplete emptying, dribbling, overflow incontinence |
Importantly, prostate size does NOT correlate well with symptom severity, and bladder outlet obstruction severity does not necessarily match LUTS severity. - Sabiston Textbook of Surgery, p. 2824
Complications of chronic obstruction:
- Bladder hypertrophy and distention
- Residual urine → recurrent UTIs
- Complete retention → painful distention
- Hydronephrosis (in severe cases)
Diagnosis
- History - LUTS symptom assessment using the International Prostate Symptom Score (IPSS)
- Digital rectal examination (DRE) - assess prostate size and consistency
- Urinalysis - rule out infection, hematuria
- PSA testing - in men with >10 year life expectancy (to screen for prostate cancer); note that BPH itself can elevate PSA
- Post-void residual volume - measured by bladder ultrasound
- Uroflowmetry - non-invasive urinary flow rate testing
- Cystoscopy / urodynamics - reserved for selected cases
Treatment
1. Lifestyle/Behavioral Modifications (first line for all patients)
- Fluid restriction (especially evenings)
- Avoiding caffeine and alcohol
- Bladder training
- Double voiding
2. Medical Therapy
α1-Adrenergic Blockers (first-line drug therapy)
- Relax smooth muscle in the bladder neck, prostate, and urethra → reduce outflow resistance
- Modern agents target α1A subtype specifically (e.g., tamsulosin, alfuzosin, silodosin)
- Side effects: orthostatic dizziness, retrograde ejaculation, rhinitis
- Act quickly (days to weeks)
5α-Reductase Inhibitors (5-ARIs)
- Block conversion of testosterone → DHT → reduce prostate volume by ~20-30% over months
- Examples: finasteride (5-ARI type 2), dutasteride (dual 5-ARI types 1 & 2)
- Reduce serum PSA by ~50% (must be accounted for when interpreting PSA for cancer screening)
- Best for large prostates (>40 mL) or elevated PSA
- Onset of benefit: 6-12 months
Combination therapy (α-blocker + 5-ARI) is more effective than monotherapy for men with large prostates and significant symptoms, as established by the MTOPS and CombAT trials.
Phosphodiesterase-5 inhibitors (e.g., tadalafil daily) are also approved for BPH-LUTS, particularly when erectile dysfunction coexists.
- Sabiston Textbook of Surgery, p. 2824
- Robbins & Kumar, p. 659
3. Surgical / Procedural Options
Reserved for patients who fail medical therapy, have refractory retention, recurrent UTIs, renal insufficiency from obstruction, or prefer definitive treatment:
| Procedure | Notes |
|---|---|
| TURP (Transurethral resection of prostate) | Gold standard; removes hyperplastic tissue endoscopically |
| Laser therapy (HoLEP, GreenLight) | Lower bleeding risk; for large prostates |
| HIFU (High-intensity focused ultrasound) | Non-incisional |
| Transurethral electrovaporization | Coagulative vaporization of tissue |
| Radiofrequency ablation (TUNA) | Minimally invasive |
| Simple open/robot-assisted prostatectomy | For very large glands (>80-100 g) |
| Prostatic urethral lift (Urolift) | Implants hold lateral lobes apart; preserves ejaculation |
- Robbins & Kumar, p. 659
- Sabiston Textbook of Surgery, p. 2824
Key Distinguishing Points vs. Prostate Cancer
| Feature | BPH | Prostate Cancer |
|---|---|---|
| Zone affected | Transition zone | Peripheral zone |
| Behavior | Benign, no metastasis | Malignant |
| Histology | Two cell layers (columnar + basal) | Single layer, loss of basal cells |
| DRE | Smooth, rubbery enlargement | Hard, nodular, asymmetric |
| PSA | Mildly elevated (proportional to size) | Often disproportionately elevated |
| Risk with age | Yes, but not premalignant | Separate condition |
Recent Evidence Note
A 2026 systematic review and meta-analysis (PMID: 42247029) evaluated curcumin vs. placebo in BPH - an emerging area of interest in complementary management, though standard pharmacologic therapy remains the evidence-based cornerstone.
This is a shared conversation. Sign in to Orris to start your own chat.