Pateint with hyperglycemia 520mg/dl weight 74 kg age 50 what should I do
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Now I have comprehensive information. Let me synthesize a structured, actionable clinical response.
Severe Hyperglycemia — 520 mg/dL | 74 kg | 50-year-old
Step 1: Immediate Assessment — Determine the Syndrome
A glucose of 520 mg/dL is a hyperglycemic emergency. Your first priority is distinguishing DKA from HHS (Hyperosmolar Hyperglycemic State), as management differs:
| Feature | DKA | HHS |
|---|---|---|
| Glucose | Usually <500 | Often >600 (can be >1000) |
| Ketones | ✅ Positive | Absent/trace |
| pH | <7.3 (acidosis) | Normal or near-normal |
| HCO₃⁻ | <15 mEq/L | >15 mEq/L |
| Osmolality | <320 mOsm/kg | >320 mOsm/kg |
| Mental status | May be altered | Often markedly altered |
| Anion gap | Elevated | Normal or mildly elevated |
At 520 mg/dL, both DKA and HHS are possible — order labs immediately.
Step 2: Stat Workup
Order simultaneously:
- BMP / Chem-7 (Na⁺, K⁺, Cl⁻, HCO₃⁻, BUN, Cr, glucose)
- Serum ketones / β-hydroxybutyrate
- Arterial blood gas (ABG) — pH, bicarbonate
- Serum osmolality — calculate: 2×Na + glucose/18 + BUN/2.8
- CBC with differential (leukocytosis ≠ infection in DKA — only bandemia suggests infection)
- Urinalysis (ketones, infection)
- Lipase (if abdominal pain present)
- ECG (hypokalemia/hyperkalemia risk)
- Chest X-ray (precipitating pneumonia?)
- HbA1c (establishes baseline, confirms diagnosis if new)
- Blood cultures if febrile
⚠️ Critical: Do NOT start insulin until you know the potassium level. Insulin drives K⁺ into cells — starting insulin with K⁺ <3.3 mEq/L can cause fatal arrhythmia.
Step 3: IV Access and Immediate Resuscitation
Fluids (start immediately, regardless of DKA vs. HHS)
| Time | Fluid | Rate |
|---|---|---|
| First 1–3 hours | 0.9% Normal Saline | 1–2 L IV (bolus over 1–3h) |
| After hemodynamic stability | 0.45% NS or 0.9% NS (based on corrected Na) | 250–500 mL/h |
| When glucose ≤250 mg/dL | Switch to D5W/0.45% NS | Continue until anion gap closed / HCO₃ normalized |
For a 74 kg patient, estimated fluid deficit in DKA is ~5–7% body weight = ~3.7–5.2 L total.
Step 4: Insulin Protocol (after K⁺ confirmed ≥3.3 mEq/L)
DKA Protocol:
- Bolus: 0.1 units/kg regular insulin IV = 7.4 units IV push
- Infusion: 0.1 units/kg/h regular insulin = 7.4 units/hour IV
- (Mix: 100 units regular insulin in 100 mL 0.9% NS → run at 7.4 mL/h)
- Target drop: 50–75 mg/dL per hour
- ⚠️ Do NOT correct >100 mg/dL/h (cerebral edema risk)
- When glucose reaches 250 mg/dL: Reduce insulin to 0.05 units/kg/h and add D5W bag
HHS Protocol:
- Lower insulin doses are often effective; fluids alone may drop glucose substantially
- Start insulin at 0.05–0.1 units/kg/h after fluid resuscitation begun
- Correct glucose slowly — rapid correction risks cerebral edema and worsening neurologic status
Step 5: Potassium Replacement
This is critical — insulin therapy causes hypokalemia:
| Serum K⁺ | Action |
|---|---|
| <3.3 mEq/L | Hold insulin, give 20–40 mEq KCl IV, recheck before starting |
| 3.3–5.5 mEq/L | Add 20–40 mEq KCl to each liter of IV fluid |
| >5.5 mEq/L | Do NOT give K⁺; monitor closely |
Step 6: Monitor Closely
| Parameter | Frequency |
|---|---|
| Blood glucose (fingerstick) | Every hour |
| Serum electrolytes (K⁺, HCO₃⁻, Na⁺) | Every 2–4 hours |
| ABG / venous pH | As needed for acidosis monitoring |
| Urine output | Every hour (target >0.5 mL/kg/h) |
| Mental status | Continuous |
Serum Na⁺ should rise as glucose corrects — if it falls, suspect overhydration with free water.
Step 7: Find and Treat the Precipitant
The most common triggers:
- Infection (sepsis, pneumonia, UTI) — most common; start broad-spectrum antibiotics if suspected
- Medication non-compliance or missed insulin
- MI or stroke (especially in HHS — always get ECG)
- New-onset diabetes
- Surgery, trauma, pancreatitis
Step 8: When to Admit
| Setting | Criteria |
|---|---|
| ICU | pH <7.0, altered mental status, hemodynamic instability, K⁺ <3.0, suspected severe HHS |
| Floor / Telemetry | Stable DKA, mild-moderate HHS |
| Discharge | Only for mild hyperglycemia without ketosis, reliable patient, able to take PO, close follow-up arranged |
For a glucose of 520 mg/dL this patient almost certainly requires hospital admission with telemetry.
Step 9: Resolution Criteria & Transition to SQ Insulin
DKA resolved when ALL three met:
- Glucose <250 mg/dL
- Bicarbonate ≥15 mEq/L
- Anion gap closed
Before stopping insulin drip: Give subcutaneous basal insulin 2 hours prior to stopping the infusion (prevents rebound ketoacidosis).
Summary Algorithm
Glucose 520 mg/dL
↓
STAT labs + ECG + cultures
↓
Start 0.9% NS 1-2L IV immediately
↓
Check K⁺:
<3.3 → Replace K⁺, hold insulin
≥3.3 → Start regular insulin 0.1 u/kg IV bolus + 0.1 u/kg/h
↓
Glucose ≤250 → Add D5W, reduce insulin
↓
Hourly glucose / Q2-4h electrolytes
↓
Treat precipitant | Admit to hospital
Sources: ROSEN's Emergency Medicine; Washington Manual of Medical Therapeutics; Harrison's Principles of Internal Medicine 22e
⚕️ Disclaimer: This is clinical decision support. Always apply individual patient context, local protocols, and senior physician judgment — particularly for critically ill patients.
Can't I give directly actrapid 14 units
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Good — now I have all I need. Here's a direct, clinical answer:
Short Answer: It Depends on the Clinical Situation
Actrapid (regular insulin) SC is not simply interchangeable with IV infusion at this glucose level. Here's the breakdown:
Why a Flat 14 Units SC Is Problematic
1. You haven't checked the potassium yet
This is the most important rule — giving any insulin (SC or IV) before confirming K⁺ ≥3.3 mEq/L can precipitate fatal hypokalemia and cardiac arrhythmia. At 520 mg/dL, the patient is almost certainly total-body K⁺-depleted even if the serum level looks normal.
2. Unreliable absorption
In severe dehydration and poor peripheral perfusion (common at this glucose level), subcutaneous absorption of insulin is unpredictable and delayed. IV insulin has immediate, controllable action. You may give 14 units SC and get almost none absorbed for 30–60 min, then a delayed dump.
3. No control over rate of correction
Correcting glucose faster than ~100 mg/dL/hour risks osmotic cerebral edema. An IV infusion lets you titrate precisely; a SC bolus does not.
4. Dose rationale: Where does 14 units come from?
The correct weight-based dose is 0.1 units/kg IV bolus = 7.4 units for your 74 kg patient, followed by 0.1 units/kg/h infusion. A 14-unit SC bolus (≈0.19 units/kg) is double the recommended bolus dose and uncontrolled in delivery.
When SC Insulin IS Acceptable in Hyperglycemia
| Scenario | SC insulin acceptable? |
|---|---|
| Mild/moderate DKA (pH ≥7.0, HCO₃ >10, alert, tolerating PO) | ✅ Yes — SC lispro or regular q1–2h protocols validated |
| Severe DKA (pH <7.0, altered mental status, hemodynamic instability) | ❌ No — IV infusion required |
| HHS | ❌ IV preferred — fluids are the priority; SC is unreliable in dehydrated patient |
| Asymptomatic hyperglycemia, no ketosis (e.g., known T2DM, glucose 250–400) | ✅ Yes — SC correction dose reasonable |
| Glucose 520 mg/dL, unknown ketosis/acidosis status | ⚠️ Do not give SC insulin until labs return |
Correct Approach for This Patient
- Get K⁺ and ketones first (10–15 min with point-of-care)
- Start 0.9% NS 1 L IV immediately — don't wait for labs for fluids
- Once K⁺ ≥3.3 and if DKA confirmed:
- Actrapid 7.4 units IV bolus + 7.4 units/hour IV infusion (0.1 u/kg each)
- If labs show no ketoacidosis and patient is alert/hemodynamically stable:
- A SC correction dose is acceptable — typically 0.1 u/kg SC = ~7 units, not 14
Bottom line: 14 units SC Actrapid is too much, too fast, and given without critical safety information (K⁺). At 520 mg/dL, always check labs first, start IV fluids, then use IV insulin at proper weight-based dosing. SC is acceptable only in mild/non-acidotic cases.
Sources: Washington Manual of Medical Therapeutics; ROSEN's Emergency Medicine
Ecg understanding give me common ecg changes with proper explanation in easy language
Reading File
Finding Sources
Finding Sources
Searching Images
normal ECG waves P QRS T labeled diagram
Finding Sources
Finding Sources
Searching Images
ECG ST elevation myocardial infarction STEMI changes
Reading File
Finding Sources
Searching Images
atrial fibrillation ECG irregular rhythm no P waves
Searching Images
hyperkalemia peaked T waves ECG changes
Searching Images
heart block complete AV block ECG P wave dissociation
Searching Images
ventricular tachycardia wide QRS ECG rhythm strip
I now have all the textbook content and images needed. Let me build a comprehensive, easy-language ECG guide with real ECG images.
📋 ECG Understanding — Common Changes Explained Simply
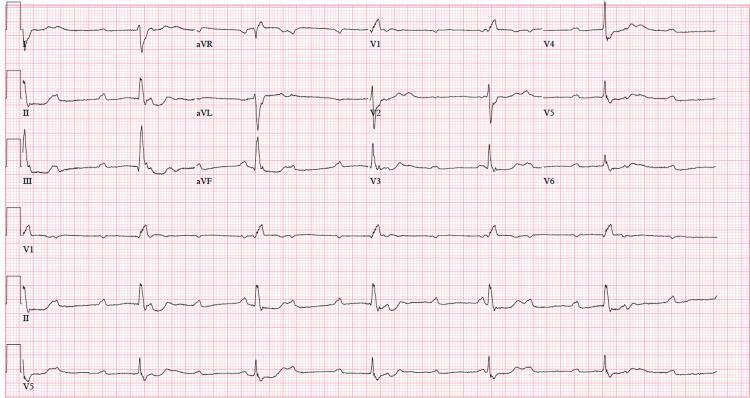
First: What is an ECG?
An ECG records the electrical activity of the heart on paper. Each heartbeat produces a wave that looks like this:
R
|
P | T
/ \ | / \
--/ \--+-------/ \-----
\ /
Q S
| Wave | What it means in plain language |
|---|---|
| P wave | Atria (upper chambers) contracting — "atria fire" |
| PR interval | Electrical signal traveling to ventricles through AV node — "the delay" |
| QRS complex | Ventricles (lower chambers) contracting — "main pump fires" |
| ST segment | Ventricles between contraction and relaxation — "resting phase" |
| T wave | Ventricles recharging — "resetting for next beat" |
| QT interval | Total ventricular electrical activity time |
Normal values to memorize:
- Heart rate: 60–100 bpm
- PR interval: 0.12–0.20 sec (3–5 small boxes)
- QRS duration: <0.12 sec (<3 small boxes)
- QT interval: <0.44 sec (corrected)
🔴 Change 1 — STEMI (Heart Attack with ST Elevation)
What it means: A coronary artery is completely blocked. The heart muscle is dying right now. This is a medical emergency.
What you see on ECG:
- ST segment rises above the baseline like a "tombstone" or "coved" shape
- Seen in specific leads depending on which artery is blocked
- Reciprocal changes — ST depression in opposite leads (mirror image)
- Later: Q waves develop (= dead tissue), T wave inverts
| ST elevation in these leads | Artery blocked | Wall affected |
|---|---|---|
| V1–V4 | LAD (Left Anterior Descending) | Anterior wall |
| II, III, aVF | RCA (Right Coronary) | Inferior wall |
| I, aVL, V5–V6 | LCx (Left Circumflex) | Lateral wall |
Remember: >1 mm elevation in limb leads, >2 mm in chest leads = significant


🟠 Change 2 — NSTEMI / Ischemia (ST Depression + T-wave Inversion)
What it means: The artery is partially blocked or there is demand ischemia. Muscle is stressed but not fully dead yet.
What you see on ECG:
- ST segment dips below the baseline (ST depression ≥0.5–1 mm)
- T wave inverts (flips upside down) — called T-wave inversion
- No ST elevation
- Deep symmetric T-wave inversions in V2–V3 = Wellens' syndrome (LAD critically stenosed — danger!)
Simple rule: ST elevation = total blockage (STEMI). ST depression = partial blockage or ischemia (NSTEMI/UA).
🟡 Change 3 — Atrial Fibrillation (AF)
What it means: The atria are firing chaotically — like a "bag of worms" instead of one coordinated squeeze. The heart beats irregularly.
What you see on ECG:
- No P waves — replaced by irregular fibrillatory (f) waves (wavy baseline)
- Irregularly irregular rhythm — R-R intervals are ALL different lengths
- QRS complexes are narrow (unless bundle branch block present)
- Fast ventricular rate (100–160 bpm if uncontrolled)
Trick to remember: If you can't find any pattern to the rhythm → think AF first.
🟡 Change 4 — Ventricular Tachycardia (VT)
What it means: The ventricles are firing very fast from an abnormal focus — bypassing the normal conduction system. Life-threatening.
What you see on ECG:
- Rate >100 bpm (usually 150–250 bpm)
- Wide, broad, bizarre QRS complexes (>0.12 sec = >3 small boxes)
- No visible P waves (or P waves dissociated from QRS)
- Regular rhythm
- Looks like a "fast, wide, ugly" tracing
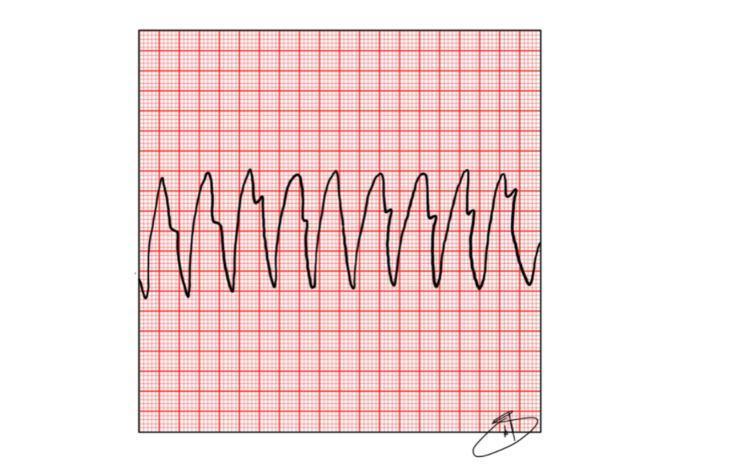
Wide + fast = VT until proven otherwise. Do not assume SVT with aberrancy — treat as VT.
🟢 Change 5 — Heart Block (AV Block)
This means the signal from atria to ventricles is delayed or blocked.
1st Degree AV Block
- PR interval >0.20 sec (>5 small boxes)
- Every P wave still conducts to a QRS
- Usually benign
2nd Degree — Mobitz I (Wenckebach)
- PR interval gets longer and longer with each beat until a QRS is dropped
- Then cycle resets
- "Longer, longer, longer… drop. Then you have a Wenckebach."
2nd Degree — Mobitz II
- PR interval is constant, then suddenly a P wave occurs with no QRS (dropped beat)
- More dangerous — can progress to complete block
- Requires pacemaker
3rd Degree (Complete Heart Block)
- No relationship between P waves and QRS complexes
- P waves march at their own rate, QRS complexes march at their own (slower) rate
- Ventricular escape rate: 20–40 bpm → very slow, dangerous
- Patient needs an emergency pacemaker
🔵 Change 6 — Hyperkalemia (High Potassium)
Why it matters: High K⁺ is directly toxic to the heart. You will see this in renal failure, DKA, crush injuries.
Progressive ECG changes as K⁺ rises:
| Serum K⁺ | ECG Change |
|---|---|
| 5.5–6.5 mEq/L | Peaked (tented) T waves — tall, narrow, symmetric |
| 6.5–7.5 mEq/L | PR prolongation, P wave flattening/disappearing, QRS widening |
| >7.5 mEq/L | Sine wave pattern (QRS and T merge together) → imminent arrest |
| >8–9 mEq/L | Ventricular fibrillation / asystole |
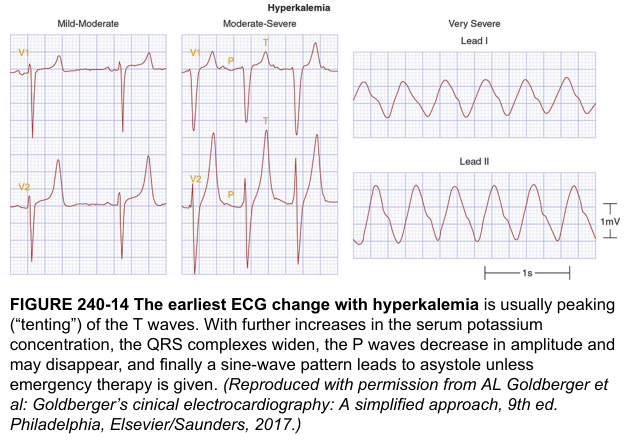
Easy memory: K⁺ goes up → T waves tent up → P waves disappear → QRS widens → sine wave → death.
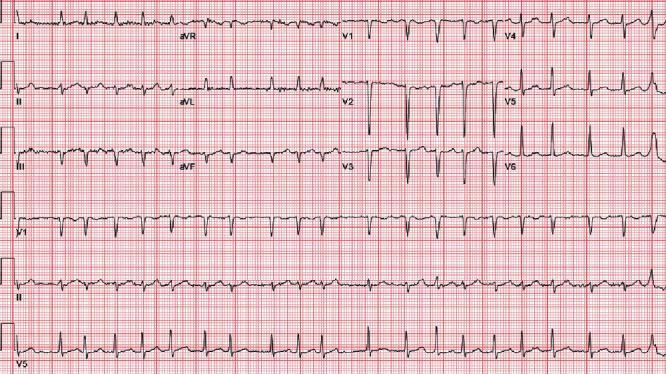
🔵 Change 7 — Left Ventricular Hypertrophy (LVH)
What it means: The left ventricle muscle wall is thickened (from chronic hypertension, aortic stenosis).
What you see:
- Tall R waves in left-sided leads (V5, V6, aVL) + deep S waves in right leads (V1, V2)
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 >35 mm
- "Strain pattern" — ST depression + T-wave inversion in V5–V6 (lateral leads)
🔵 Change 8 — Bundle Branch Block
What it means: One of the electrical highways to the ventricles is blocked, so activation takes a detour.
| LBBB (Left BBB) | RBBB (Right BBB) | |
|---|---|---|
| QRS | Wide >0.12s | Wide >0.12s |
| V1 appearance | Broad negative QS | rSR' ("rabbit ears" M-shape) |
| V6 appearance | Broad tall R (no Q or S) | Wide S wave |
| Key memory | "WiLLiaM" — W in V1, M in V6 | "MaRRoW" — M in V1, W in V6 |
| Clinical significance | Often indicates significant cardiac disease | Can be normal or right heart strain |
New LBBB + chest pain = treat like STEMI (Sgarbossa criteria apply).
🔵 Change 9 — Pulmonary Embolism (PE)
What you see:
- Sinus tachycardia (most common finding — ~40% of PE)
- Classic but rare: S1Q3T3 — deep S in lead I, Q wave in III, inverted T in III
- Right heart strain: RBBB, right axis deviation
- T-wave inversions in V1–V4 (right ventricular strain pattern)
🔵 Change 10 — Pericarditis
What it means: Inflammation of the sac around the heart.
What you see:
- Diffuse ST elevation in almost all leads (not just one territory) — saddle-shaped, concave up
- PR depression (very specific for pericarditis)
- No reciprocal ST depression (unlike MI)
- No Q waves
Simple rule: ST elevation everywhere + PR depression = pericarditis. ST elevation in one territory = MI.
Quick Reference Summary
| ECG Change | What to Think | Key Action |
|---|---|---|
| ST elevation (one territory) | STEMI — artery blocked | 🚨 Activate cath lab immediately |
| ST depression + T inversion | NSTEMI/ischemia | Heparin, troponins, cardiology |
| No P waves + irregular | Atrial fibrillation | Rate control, anticoagulation |
| Wide + fast + no P waves | Ventricular tachycardia | 🚨 Cardiovert / defibrillate |
| P waves + slow + dissociated | Complete heart block | 🚨 Pacemaker urgently |
| Peaked T waves | Hyperkalemia | Calcium gluconate, treat K⁺ |
| Wide QRS + rSR' in V1 | RBBB | Evaluate for PE/RV strain |
| Wide QRS + W in V1 | LBBB + chest pain | Treat as STEMI |
| Diffuse ST elevation + PR depression | Pericarditis | NSAIDs, colchicine |
Sources: Medical Physiology (Boron & Boulpaep); ROSEN's Emergency Medicine; Harrison's Principles of Internal Medicine 22e
This is a shared conversation. Sign in to Orris to start your own chat.