Pulmonary embolism
Reading File
Finding Sources
Searching PubMed
"pulmonary embolism"[MeSH Terms] AND "diagnosis" AND "management"
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Now I have comprehensive data from multiple authoritative sources. Let me compile the full answer.
Pulmonary Embolism (PE)
Definition and Epidemiology
PE is obstruction of the pulmonary arterial circulation, most commonly by thrombus arising from deep veins of the lower extremities or pelvis (venous thromboembolism, VTE). It is a leading cause of preventable death in hospitalized patients, responsible for approximately 25% of sudden cardiac deaths, and accounts for 15% of maternal mortality in the United States. The incidence of VTE in pregnancy is about 0.5-1.2 per 1,000 pregnancies.
- Harrison's Principles of Internal Medicine 22E, p. 2199
- ROSEN's Emergency Medicine, p. 1202
Pathophysiology
PE arises from Virchow's triad: venous stasis, hypercoagulability, and endothelial injury, typically with an inflammatory trigger leading to DVT formation. Once a thrombus detaches, it travels through the vena cava and right heart to lodge in the pulmonary arteries.
The cascade of downstream effects includes:
- Increased pulmonary vascular resistance - from physical obstruction and platelet secretion of vasoconstrictors (serotonin), causing ventilation-perfusion (V/Q) mismatch even at sites remote from the embolus
- Impaired gas exchange - increased alveolar dead space, hypoxemia, right-to-left shunting
- Alveolar hyperventilation - via reflex stimulation of irritant receptors
- Decreased pulmonary compliance - from lung edema, hemorrhage, or surfactant loss
The RV failure cascade (the key mechanism of death):
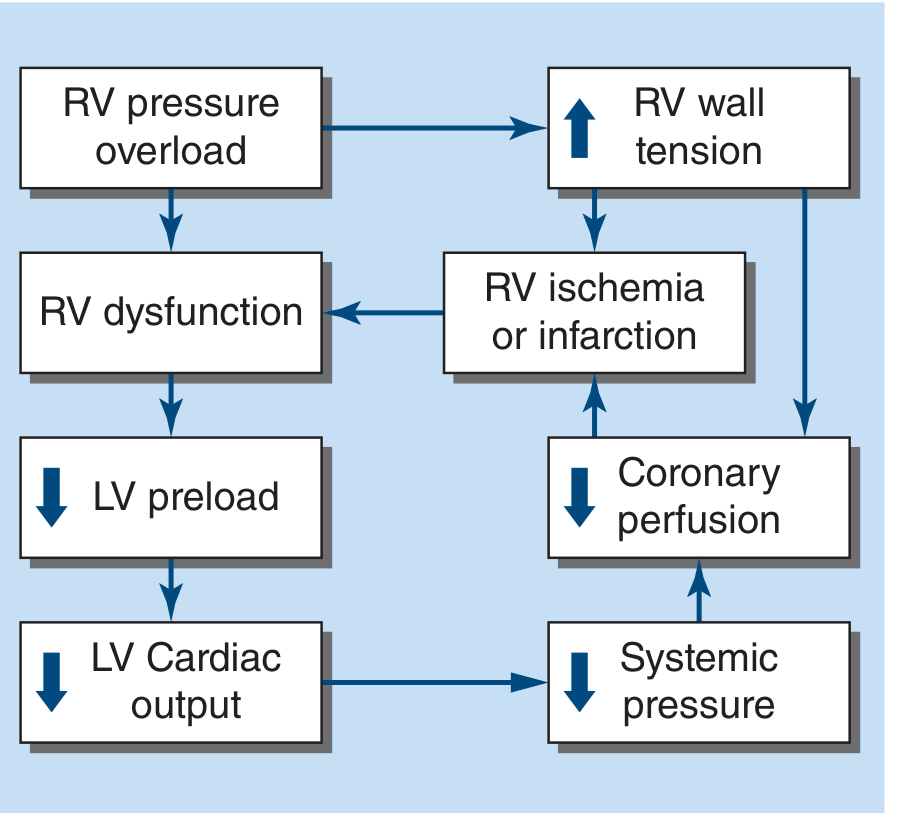
Pulmonary artery obstruction → RV pressure overload → increased RV wall tension → RV dilation/stretch/dysfunction → BNP release, interventricular septal bowing into LV → impaired LV filling → reduced LV cardiac output → systemic hypotension → decreased coronary perfusion pressure → RV ischemia/microinfarction (troponin release) → further RV dysfunction → circulatory collapse and death.
- Harrison's Principles of Internal Medicine 22E, p. 2200
Risk Factors
| Category | Examples |
|---|---|
| Acquired | Cancer, surgery, trauma, obesity, smoking, immobilization, estrogen/OCP use, pregnancy, postpartum, long-haul travel |
| Inherited thrombophilia | Factor V Leiden, prothrombin G20210A, antithrombin III deficiency, protein C/S deficiency |
| Acquired thrombophilia | Antiphospholipid syndrome |
| Comorbidities | Hypertension, COPD, CKD, CHF, prior VTE, HIT |
| Other | Advanced age, COVID-19 (via endothelial activation), sedentary lifestyle |
- Harrison's Principles of Internal Medicine 22E, pp. 2200-2201
Clinical Presentation
PE is the great masquerader - it can present with virtually any cardiorespiratory symptom. Key facts:
- Dyspnea is the most common symptom (75-80%), but is absent in ~25% of patients
- Chest pain (second most common) - pleuritic in only 20%, typically from peripheral PE causing pulmonary infarction
- Hemoptysis - suggests pulmonary infarction (peripheral PE)
- Unilateral leg swelling - present in <30%, but relatively specific when combined with dyspnea or chest pain
- Syncope - uncommon (<5% of syncope presentations), but when unexplained, raises suspicion
- PEA cardiac arrest - most common ECG finding in PE-induced cardiac arrest
When PE causes pulmonary infarction, the presentation mimics lobar pneumonia (pleuritic pain, cough, hemoptysis, low-grade fever). A temperature >38.6°C or productive sputum cough favors pneumonia over PE.
- ROSEN's Emergency Medicine, pp. 1202-1203
Diagnosis
Step 1: Pre-test Probability (PTP) Assessment
Wells Score for PE
| Variable | Points |
|---|---|
| Clinical signs of DVT | 3 |
| PE is the most likely diagnosis | 3 |
| Heart rate >100 bpm | 1.5 |
| Immobilization or surgery in prior 4 weeks | 1.5 |
| Prior DVT or PE | 1.5 |
| Hemoptysis | 1 |
| Malignancy (treatment ongoing or within 6 months) | 1 |
Score <2 = low, 2-6 = moderate, >6 = high. A two-level version: >4 = "PE likely."
Revised Geneva Score (fully objective, no "clinical gestalt" item)
| Feature | Points |
|---|---|
| Age >65 | 1 |
| Prior PE or DVT | 3 |
| Recent surgery/immobilization (within 4 weeks) | 2 |
| Active cancer | 2 |
| Unilateral leg pain | 3 |
| Hemoptysis | 2 |
| HR 75-94 bpm | 3; HR >95 bpm = 5 |
| Unilateral edema + leg pain on palpation | 4 |
Score 0-3 = low, 4-10 = intermediate, >10 = high.
- ROSEN's Emergency Medicine, p. 1205
Step 2: PERC Rule (rule-out without testing)
When clinical gestalt estimates low PTP and all 8 criteria are met, the probability falls below the 2% testing threshold - no further workup needed:
- Age <50
- Pulse <100
- SaO2 >94%
- No unilateral leg swelling
- No hemoptysis
- No recent trauma or surgery
- No prior PE/DVT
- No hormone use
- ROSEN's Emergency Medicine, p. 1205
Step 3: D-Dimer
- Sensitivity 95-98%, specificity 40-55%
- A normal D-dimer excludes PE in patients with non-high PTP (negative predictive value 99-100%)
- Age-adjusted D-dimer (for patients >50 years): upper limit of normal = age × 10 ng/mL (e.g., 700 ng/mL for a 70-year-old)
- D-dimer has limited utility in hospitalized patients (frequently elevated due to systemic illness) and in pregnancy (elevated by trimester)
- Harrison's Principles of Internal Medicine 22E, p. 2203; ROSEN's Emergency Medicine, p. 1205
Step 4: Imaging
CT Pulmonary Angiography (CTPA) - first-line imaging
- Has largely replaced V/Q scanning; widely available, rapid, allows direct visualization of thrombus
- Highly sensitive and specific at the segmental level and above
- Also identifies alternative diagnoses
- Detects isolated subsegmental thrombi in ~1-5% (clinical significance uncertain)
- Goldman-Cecil Medicine, p. 803
Ventilation-Perfusion (V/Q) Scanning
- Preferred when CTPA is contraindicated (CKD, contrast allergy, pregnancy - lower fetal radiation dose)
- A normal perfusion scan excludes PE; a high-probability scan (segmental or larger V/Q mismatch) confirms it
- Only 10% of scans are high-probability; ~65% are non-diagnostic ("intermediate/non-high probability")
- Goldman-Cecil Medicine, p. 803
Echocardiography
- Not a primary diagnostic tool, but useful in hemodynamically unstable patients
- Findings of RV dysfunction: RV dilation or hypokinesis, RV:LV ratio >1, increased tricuspid regurgitation velocity, septal bowing
- Recommended in severe hypoxemia or hemodynamic compromise
- Goldman-Cecil Medicine, p. 805
ECG - limited sensitivity, mainly in large PE
- T-wave inversions V1-V4
- S1Q3T3 pattern (classic but uncommon)
- New right bundle branch block (complete or incomplete)
- PEA in cardiac arrest
Risk Stratification and Treatment
Treatment strategy depends on hemodynamic status and evidence of RV dysfunction:
| Category | Criteria | Treatment |
|---|---|---|
| Low-Risk ("non-massive") | Hemodynamically stable, no RV dysfunction | Anticoagulation (DOAC preferred); outpatient management feasible |
| Intermediate-Risk ("submassive") | Stable hemodynamics + RV dysfunction (echo/CT) and/or elevated troponin | Anticoagulation; consider observation/monitoring; thrombolysis reserved for deterioration |
| High-Risk ("massive") | SBP <90 mmHg sustained ≥15 min, vasopressor requirement, or profound bradycardia | Thrombolysis + anticoagulation; surgical/catheter thrombectomy if contraindications to thrombolysis |
Mortality: <1-3% (low risk) → 3-15% (intermediate) → 15-50% (high risk)
- ROSEN's Emergency Medicine, p. 1208
Anticoagulation
Anticoagulation is the cornerstone of VTE treatment, initiated immediately even before confirmatory testing in high suspicion cases.
Preferred agents:
- DOACs (rivaroxaban, apixaban) - preferred first-line for most patients; fixed dosing, no routine monitoring required
- LMWH (enoxaparin) - subcutaneous, predictable kinetics; preferred in cancer-associated VTE and pregnancy (does not cross placenta)
- UFH (unfractionated heparin) - IV; preferred when thrombolysis/surgery is being considered (short half-life); provides unreliable anticoagulation in first 24-48h
- Fondaparinux - for patients with HIT (heparin-induced thrombocytopenia); no protamine reversal
Duration of therapy (3 phases):
- Initial phase (1-3 weeks): Prevent extension and fatal PE
- Long-term (3 months): Treat VTE, reduce post-thrombotic syndrome and chronic thromboembolic pulmonary hypertension (CTEPH)
- Extended (>3 months): When recurrence risk without anticoagulation exceeds bleeding risk on it
Reversal agents:
- UFH: protamine sulfate (near-complete reversal)
- LMWH: protamine (only ~50% reversal)
- Rivaroxaban/apixaban: andexanet alfa (anti-Xa reversal); 4-factor PCC has limited evidence
- Goldman-Cecil Medicine, p. 804; ROSEN's Emergency Medicine, p. 989
Thrombolytic (Fibrinolytic) Therapy
Indicated for high-risk PE (hemodynamic instability) without contraindications.
Regimens:
- Alteplase (rtPA): 100 mg IV over 2 hours (or two 50-mg boluses 15 minutes apart for unstable patients)
- Reteplase: 10 units IV over 2 minutes, repeated at 30 minutes
- Tenecteplase: Single weight-based bolus over 5-10 seconds
For intermediate-risk PE, thrombolysis is generally reserved for patients who deteriorate despite anticoagulation.
- ROSEN's Emergency Medicine, p. 992
Supportive Care (High-Risk PE)
- Supplemental oxygen; intubation if needed (use low tidal volumes; PEEP with caution - reduces venous return)
- Modest IV fluid resuscitation for RV failure
- Vasopressors: norepinephrine, dopamine, or dobutamine for refractory hypotension
- Emerging: endothelin antagonists, phosphodiesterase-5 inhibitors for pulmonary hypertension
IVC Filter
- For patients with absolute contraindications to anticoagulation
- Retrievable filters preferred; not superior to anticoagulation for recurrence prevention in patients who can be anticoagulated
Special Populations
Pregnancy:
- DVT/PE is the leading cause of maternal mortality (15% of maternal deaths)
- LMWH is the anticoagulant of choice (does not cross the placenta; DOACs contraindicated)
- D-dimer has limited utility (elevated in normal pregnancy); a pregnancy-adapted YEARS algorithm may help
- CTPA and V/Q scanning can both be used; halving the perfusion dose reduces fetal radiation
- Murray & Nadel's Respiratory Medicine, p. 3029
Cancer-associated VTE:
- LMWH or DOACs (apixaban, rivaroxaban) preferred over warfarin; indefinite anticoagulation often required
Subsegmental PE:
- If no DVT on bilateral lower limb ultrasound, no RV dysfunction, and no ongoing major thrombotic risk - watchful waiting without anticoagulation is reasonable
Complications
- CTEPH (Chronic Thromboembolic Pulmonary Hypertension) - mechanical obstruction from incompletely resolved thrombus
- Post-thrombotic syndrome - valvular incompetence and venous hypertension in the affected limb
- Recurrent VTE - highest risk in first weeks; residual DVT and malignancy are major risk factors
- PE-related sudden death - accounts for ~25% of sudden cardiac deaths
Prophylaxis
- Early ambulation post-operatively
- Graduated compression stockings in bedridden patients
- Pharmacologic anticoagulation (LMWH/UFH) in high-risk surgical/medical patients
- Robbins & Cotran Pathologic Basis of Disease, p. 3250-3254
Recent evidence note: A 2026 meta-analysis (PMID 41161416) found that standard diagnostic strategies (D-dimer + Wells) have limited safety for ruling out PE in patients with chronic lung disease - these patients may warrant direct imaging more readily. A 2025 meta-analysis (PMID 39256101) identified specific predictors of PE in COPD exacerbations that may guide clinical decision-making in that population.
This is a shared conversation. Sign in to Orris to start your own chat.