Essay answer for "Lothrop procedure" and "Modified Lothrop procedure" under 1000 words. Include flowcharts, diagrams.
Reading File
Finding Sources
Finding Sources
Searching Images
Lothrop procedure frontal sinus surgery endoscopic
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Now I have everything needed for a thorough essay. Here it is:
The Lothrop Procedure and Modified (Endoscopic) Lothrop Procedure
Historical Background
The original Lothrop procedure (1914) was an external, open approach to the frontal sinus. Arthur Lyman Lothrop described a combined external and transnasal operation designed to establish permanent drainage of the diseased frontal sinus. It involved:
- A Lynch-type external incision along the medial orbital wall
- Removal of the floor of the frontal sinus bilaterally
- Resection of the intersinus septum to create a large common cavity
- Resection of the upper nasal septum to enable drainage into the nasal cavity
The goal was to create a single, wide drainage pathway shared by both frontal sinuses directly into the nasal cavity — essentially a bilateral frontal sinus trephination with exteriorisation. Although anatomically sound in concept, the open approach carried significant morbidity: facial scarring, risk of frontal bone osteitis, and high rates of long-term stenosis of the drainage pathway due to mucosal cicatrization.
The Draf Classification — Context for the Modified Lothrop
To understand the Modified Lothrop, one must understand the Draf classification of endoscopic frontal sinus approaches (the "Fulda concept"), as all modern iterations are discussed within this framework:
┌──────────────────────────────────────────────────────────────────────┐
│ DRAF CLASSIFICATION OF FRONTAL APPROACHES │
├───────────┬──────────────────────────────────┬───────────────────────┤
│ Draf I │ Complete ethmoidectomy; removal │ No frontal recess │
│ │ of bulla and suprabullar cells │ instrumentation │
├───────────┼──────────────────────────────────┼───────────────────────┤
│ Draf IIa │ Enlargement of frontal outflow │ "Uncapping the egg" │
│ │ tract; remove occupying cells; │ Frontal sinusotomy │
│ │ preserve mucosa │ │
├───────────┼──────────────────────────────────┼───────────────────────┤
│ Draf IIb │ Drill floor of frontal sinus │ UNILATERAL drillout │
│ │ from lamina papyracea to septum │ Frontal rescue proc. │
├───────────┼──────────────────────────────────┼───────────────────────┤
│ Draf III │ Drill BOTH frontal sinus floors │ = Endoscopic Modified │
│ (= EMLP) │ + intersinus septum + frontal │ Lothrop Procedure │
│ │ beak + superoanterior nasal sept │ Median drainage │
└───────────┴──────────────────────────────────┴───────────────────────┘
The Draf type I is effectively the most conservative, while Draf III represents the maximum endoscopic frontal sinus drainage procedure and is synonymous with the Endoscopic Modified Lothrop Procedure (EMLP).
The Modified Lothrop Procedure (EMLP / Draf III)
The EMLP was first described by Gross et al. in 1995 as a transnasal endoscopic alternative to frontal sinus obliteration. It preserves the Lothrop concept — bilateral drainage into a single common cavity — while eliminating the external incision.
Indications
┌──────────────────────────────────────────────────────────────┐
│ INDICATIONS FOR EMLP (DRAF III) │
├──────────────────────────────────────────────────────────────┤
│ • Failed prior endoscopic frontal sinus surgery (revision) │
│ • Extensive sinonasal polyposis with frontal involvement │
│ • Frontal sinus mucocele or pyocele │
│ • Inverted papilloma of the frontal recess │
│ • Frontal sinus CSF leak repair │
│ • Frontal sinus tumour (benign/selected malignant) │
│ • Osteoma of the frontal sinus │
│ • Cystic fibrosis with severe frontal disease │
│ • Frontal sinus trauma / foreign body retrieval │
└──────────────────────────────────────────────────────────────┘
Severe frontal sinus disease, particularly in revision cases, may require more extensive techniques such as a modified Lothrop (Draf III) procedure. — K.J. Lee's Essential Otolaryngology
Surgical Steps
The procedure is performed under general anaesthesia with intraoperative CT-guided navigation in most centres. The stepwise approach is:
EMLP SURGICAL FLOWCHART
═══════════════════════════════════════════════════
1. Bilateral total ethmoidectomy (anterior + posterior)
↓
2. Bilateral Draf IIa / IIb to identify both frontal recesses
↓
3. Resect the superior nasal septum ("septum window") —
creates transseptal access; preserves olfactory strips
↓
4. Identify both frontal recesses bilaterally
↓
5. Remove mucosa over the nasal beak (lateral wall to lateral wall)
↓
6. Drill frontal beak using 15° 5-mm diamond drill —
rolling, anteromedial direction
[Landmark: skull base = olfactory fibres posteriorly]
↓
7. Remove intersinus septum superiorly (as high as possible)
↓
8. Continue anteriorly almost to skin
(preserve <1 mm bony shell beneath nasal skin)
↓
9. Final neo-ostium boundaries:
LATERAL — lacrimal bones
POSTERIOR — anterior skull base / first olfactory nerve
ANTERIOR — thin bony shell beneath nasal skin
↓
10. Place antibiotic-steroid-impregnated gauze / silastic stent
→ removed at 10–14 days
═══════════════════════════════════════════════════
A key technical pearl: instrumentation that is medial and posterior carries the greatest risk to the lateral lamella and skull base, making a CSF leak the primary surgical complication. Lateral manoeuvres risk orbital entry, so the eye should be balloted intraoperatively to detect inadvertent penetration.
Endoscopic View — Draf III (EMLP)
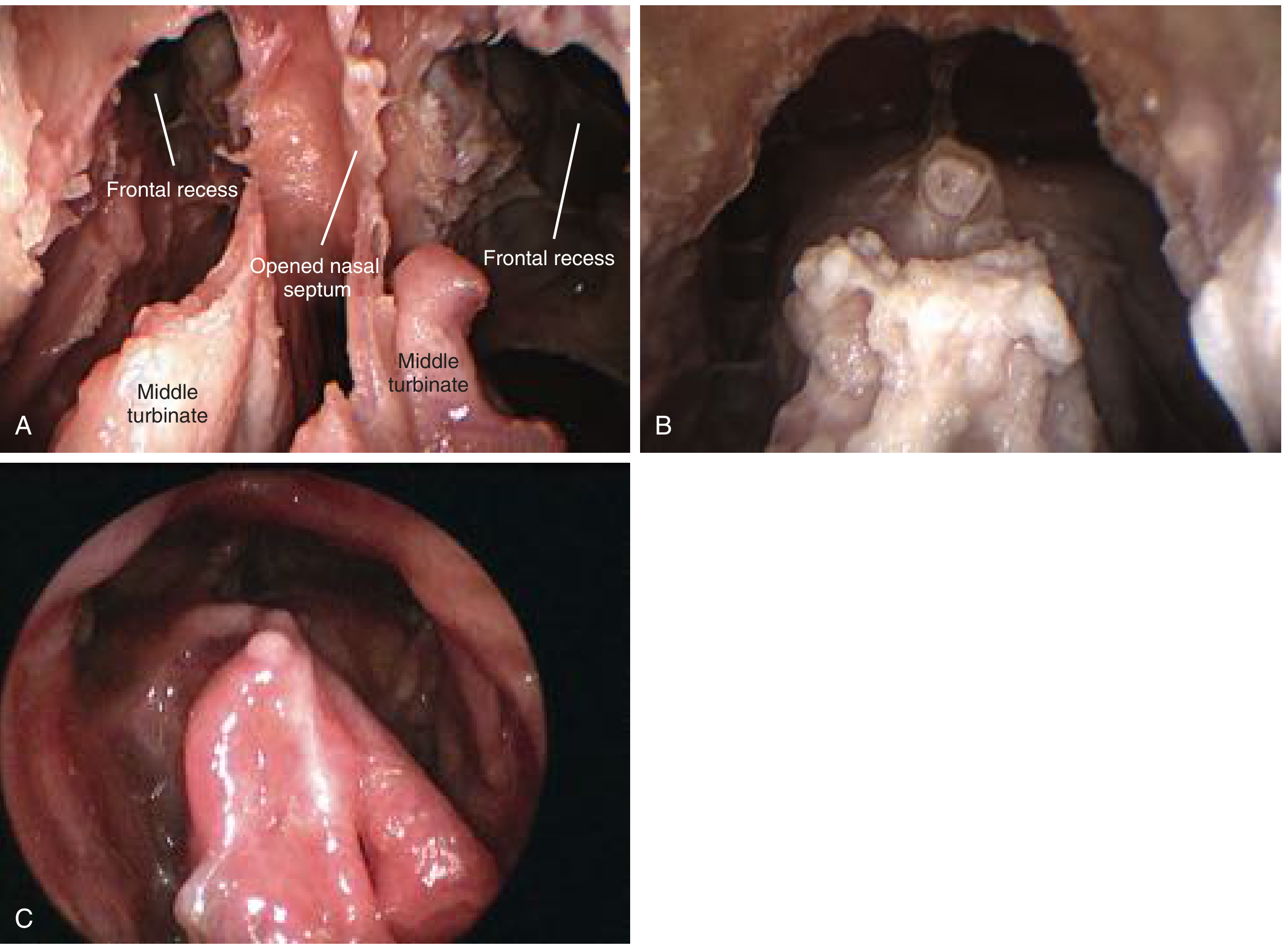
Draf III / EMLP — (A) Opening the bilateral frontal recess and making the septum window; (B) neo-ostium drilled as widely as possible; (C) patent neo-ostium 8 years post-operatively. — Cummings Otolaryngology
Intraoperative View Post-EMLP
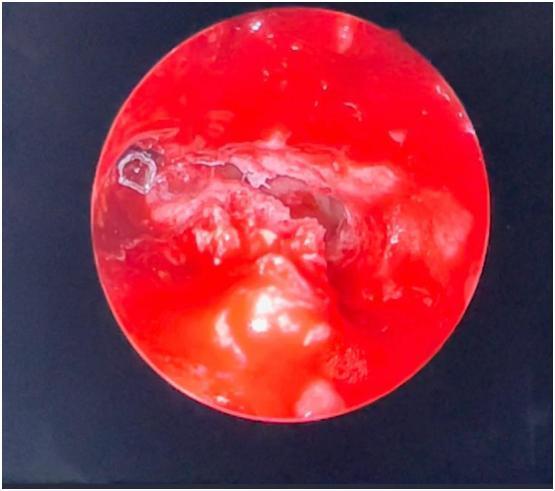
Intraoperative endoscopic view after EMLP (Draf III) — note the wide neo-ostium created across the midline with irregular bony margins at the drilled frontal floor.
Comparison: Original Lothrop vs. Modified (Endoscopic) Lothrop
┌─────────────────────┬────────────────────────┬──────────────────────────┐
│ Feature │ Original Lothrop (1914)│ Modified EMLP (Draf III) │
├─────────────────────┼────────────────────────┼──────────────────────────┤
│ Approach │ External (Lynch) │ Fully endoscopic │
│ Incision │ Medial orbital / brow │ None (transnasal) │
│ Frontal floor │ Bilateral removal │ Bilateral drillout │
│ Intersinus septum │ Resected │ Drilled out │
│ Nasal septum │ Superior portion removed│ Septum window (partial) │
│ Drainage │ Common nasal cavity │ Large neo-ostium → nose │
│ Morbidity │ High (facial, scarring)│ Lower; endoscope-related │
│ Stenosis risk │ Very high │ 10–30% │
│ Navigation │ None │ CT-image guidance │
│ Indication today │ Largely abandoned │ Preferred maximum approach│
└─────────────────────┴────────────────────────┴──────────────────────────┘
Outcomes and Complications
Stenosis of the neo-ostium is the principal long-term complication of EMLP, reported in 10–30% of cases, and is associated with:
- Asthma
- Allergy
- Cystic fibrosis
- Previous frontal sinus surgery
Management of early stenosis: local corticosteroid injection when a thick web forms at the nasofrontal beak within the first 3 months. Late bridging adhesions may require endoscopic excision of scar tissue, usually sufficient for a durable outcome. — Cummings Otolaryngology
POST-EMLP STENOSIS MANAGEMENT ALGORITHM
════════════════════════════════════════
Neo-ostium stenosis detected
│
├─── Early (<3 months): Thick web forming?
│ → Local corticosteroid injection
│
└─── Late: Bridging adhesions / progressive scar?
→ Endoscopic scar excision of neo-ostium
│
└─── Adequate result?
YES → Surveillance
NO → Reassess / consider obliteration
════════════════════════════════════════
The strategy of "all or none" is well-established: either avoid drilling the frontal recess altogether (Draf I) or commit to the maximum Draf III, because intermediate drilling (Draf IIb) carries high rates of scarring and stenosis without the compensating drainage advantage of the full bilateral procedure.
Summary
The Lothrop procedure established the foundational concept of bilateral frontal sinus drainage via a common neo-ostium and nasal septal resection. Its external approach made it morbid and prone to long-term failure. The Endoscopic Modified Lothrop Procedure (EMLP, Draf III) re-operationalised this concept entirely endonasally, using powered drills and endoscopic navigation to achieve the same anatomical goal with far less morbidity. It now represents the maximum endoscopic approach to the frontal sinus and occupies the apex of the Draf classification system, reserved for revision or complex disease where lesser procedures have failed or are inadequate.
Sources: Cummings Otolaryngology Head and Neck Surgery, 7th ed.; K.J. Lee's Essential Otolaryngology, 11th ed.
This is a shared conversation. Sign in to Orris to start your own chat.