Here is your complete, exam-ready MUHS 2nd MBBS Pathology answer covering all the topics requested. This is structured for both SAQ and LAQ formats.
LEUKEMIAS - Complete MUHS Exam Notes (2nd MBBS Pathology)
PART A: DEFINITION AND CLASSIFICATION OF LEUKEMIA
Definition
Leukemia is a clonal neoplastic proliferation of hematopoietic stem cells or their precursors that accumulate in the bone marrow, peripheral blood, and other tissues, leading to suppression of normal hematopoiesis.
Classification
LEUKEMIA
├── ACUTE (blasts ≥ 20% in marrow/blood)
│ ├── Acute Myeloid Leukemia (AML) - M0 to M7 by FAB
│ └── Acute Lymphoblastic Leukemia (ALL) - L1, L2, L3 by FAB
│
└── CHRONIC (mature/maturing cells)
├── Chronic Myeloid Leukemia (CML)
├── Chronic Lymphocytic Leukemia (CLL)
├── Hairy Cell Leukemia
└── Others
Key distinguishing rule (MUHS exam tip):
- Acute leukemia = blasts ≥ 20% in bone marrow or blood (WHO criterion)
- Chronic leukemia = predominantly mature or maturing cells
PART B: ACUTE LYMPHOBLASTIC LEUKEMIA (ALL)
Definition
ALL is a neoplasm of immature lymphoid precursors (lymphoblasts) - either pre-B or pre-T cells - that accumulates in the bone marrow and spills into the peripheral blood.
Epidemiology
- Most common cancer in children (peak age: 3-5 years)
- ~85% are B-ALL (pre-B cell origin)
- ~15% are T-ALL (adolescent males, thymic mass)
- Slight male predominance
Pathogenesis
- BCR-ABL fusion (Ph chromosome, t(9;22)) in ~25% adult ALL
- t(12;21) - ETV6::RUNX1 fusion - 25% of B-ALL (good prognosis)
- Mutations in NOTCH1 (T-ALL), PAX5, TCF3 (B-ALL)
- Block in lymphoid differentiation → accumulation of non-functional blasts
PERIPHERAL BLOOD SMEAR FINDINGS - ALL
╔══════════════════════════════════════════════════════╗
║ PERIPHERAL BLOOD SMEAR - ALL ║
╠══════════════════════════════════════════════════════╣
║ • Normocytic normochromic ANEMIA ║
║ • THROMBOCYTOPENIA (low platelets) ║
║ • WBC count - variable (↑, normal or ↓) ║
║ • LYMPHOBLASTS seen in peripheral blood: ║
║ - Small to medium sized cells ║
║ - Scant cytoplasm ║
║ - Round/oval nucleus ║
║ - Fine (stippled) nuclear chromatin ║
║ - Inconspicuous nucleoli (L1) OR ║
║ prominent nucleoli (L2) ║
║ - No Auer rods (KEY FEATURE - differentiates ║
║ from AML) ║
║ • Smudge cells (basket cells) may be seen ║
╚══════════════════════════════════════════════════════╝
BONE MARROW ASPIRATION FINDINGS - ALL
╔══════════════════════════════════════════════════════╗
║ BONE MARROW ASPIRATION - ALL ║
╠══════════════════════════════════════════════════════╣
║ GROSS: Marrow is HYPERCELLULAR (packed marrow) ║
║ ║
║ MICROSCOPY: ║
║ • ≥ 20% lymphoblasts (often 60-100%) ║
║ • Normal erythroid, myeloid, and megakaryocytic ║
║ precursors are REPLACED / markedly reduced ║
║ • Lymphoblasts: scant cytoplasm, round nucleus, ║
║ fine chromatin, inconspicuous/absent nucleoli ║
║ • NO Auer rods ║
║ • TdT (Terminal Deoxynucleotidyl Transferase) ║
║ POSITIVE - nuclear stain (HALLMARK OF ALL) ║
║ • Mitotic figures common ║
║ ║
║ CYTOCHEMISTRY: ║
║ • PAS (Periodic Acid Schiff) - POSITIVE (chunky/ ║
║ block pattern) ║
║ • MPO (Myeloperoxidase) - NEGATIVE ║
║ • Sudan Black B - NEGATIVE ║
║ • TdT - POSITIVE (nuclear marker) ║
╚══════════════════════════════════════════════════════╝
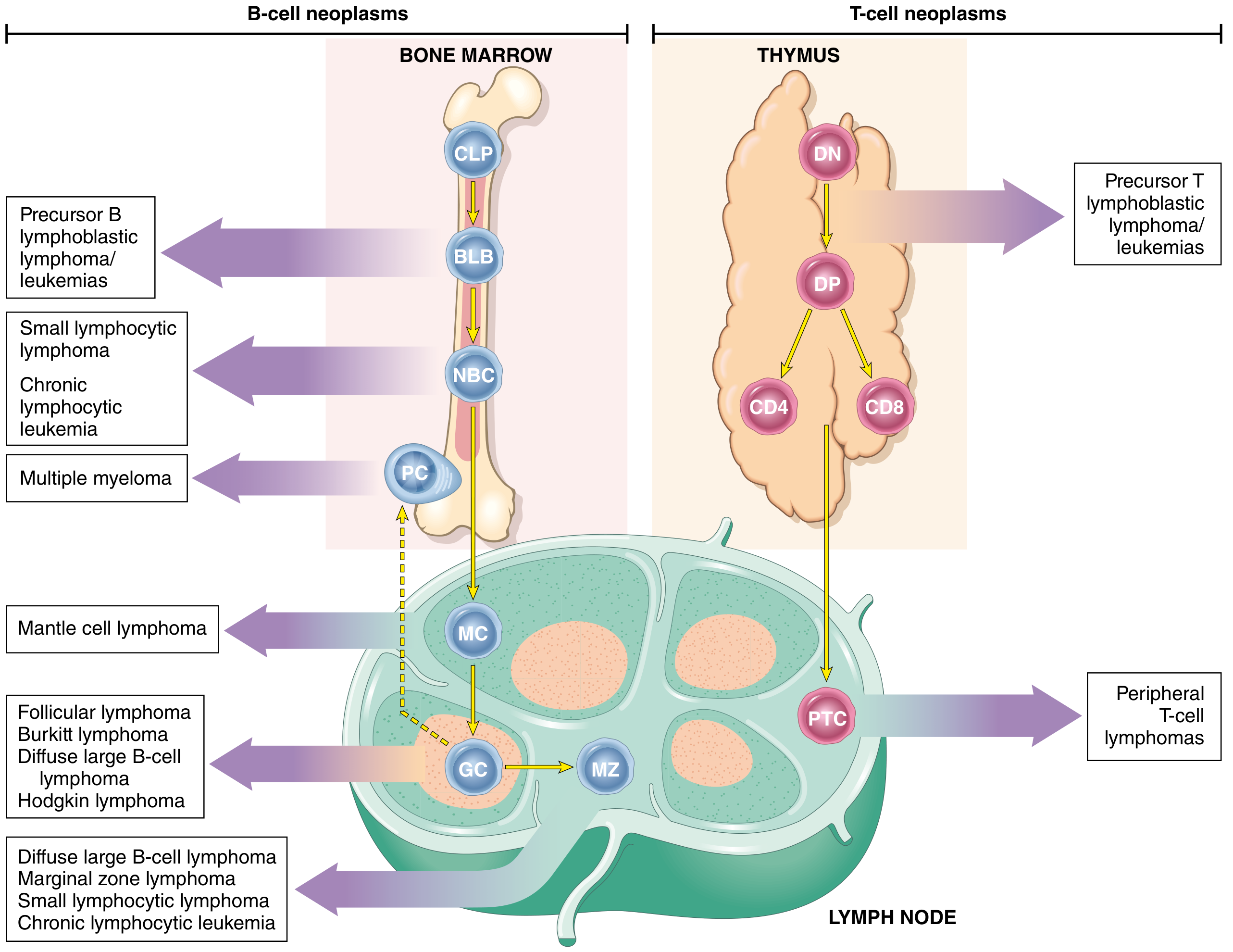
Origin of B-cell and T-cell neoplasms (Robbins/Kumar diagram):
Fig: Origin of lymphoid neoplasms. B-ALL arises from pre-B lymphoblasts (BLB) in bone marrow; T-ALL arises from double-negative/double-positive T cells in thymus.
FAB Classification of ALL (L1, L2, L3)
| Feature | L1 | L2 | L3 (Burkitt type) |
|---|
| Cell size | Small, uniform | Large, heterogeneous | Large, uniform |
| Cytoplasm | Scant | Moderate | Moderate, DEEPLY BASOPHILIC |
| Nucleus | Regular, round | Irregular, clefted | Regular, oval |
| Nucleoli | Inconspicuous | 1 or more PROMINENT | Prominent |
| Chromatin | Fine, homogeneous | Variable | Fine, stippled |
| Vacuoles | Absent | Absent | PROMINENT (starry sky) |
| Age | Children (most common) | Adults | Rare, EBV-assoc. |
MUHS exam tip: L1 is most common in children (75%), L2 in adults, L3 (Burkitt) is associated with t(8;14) and EBV.
Clinical Features of ALL
- Bone marrow failure symptoms (commonest presentation):
- Fatigue, pallor (anemia)
- Fever, infections (neutropenia)
- Bleeding, petechiae (thrombocytopenia)
- Tissue infiltration:
- Lymphadenopathy, splenomegaly, hepatomegaly
- CNS involvement (headache, vomiting - requires CNS prophylaxis)
- Mediastinal mass (T-ALL - superior vena caval syndrome)
- Bone pain (marrow expansion)
- Testicular involvement (males - sanctuary site)
PART C: CHRONIC MYELOID LEUKEMIA (CML)
Definition
CML is a myeloproliferative neoplasm arising from a transformed pluripotent hematopoietic stem cell, characterized by the BCR-ABL fusion gene resulting from the Philadelphia chromosome t(9;22)(q34;q11).
Pathogenesis
- t(9;22) translocation creates BCR::ABL chimeric gene
- Encodes a 210 kDa constitutively active tyrosine kinase (p210)
- Mimics growth factor receptor signaling (RAS, JAK/STAT pathways)
- Does NOT block differentiation initially - hence cells still mature (unlike acute leukemia)
- Cell of origin: pluripotent HSC
Chromosome 9 + Chromosome 22
ABL gene BCR gene
↓ t(9;22) translocation ↓
Philadelphia Chromosome (Ph)
↓
BCR-ABL fusion
↓
p210 BCR-ABL tyrosine kinase
↓
Constitutive cell proliferation
(granulocytic and megakaryocytic)
PERIPHERAL BLOOD SMEAR FINDINGS - CML ★★ (Most asked)
╔══════════════════════════════════════════════════════╗
║ CML - PERIPHERAL BLOOD SMEAR ║
╠══════════════════════════════════════════════════════╣
║ • LEUKOCYTOSIS (WBC often > 100,000 cells/μL) ║
║ - "Leukaemic hiatus" is ABSENT (unlike AML) ║
║ ║
║ • MYELOID SERIES - ALL STAGES present: ║
║ - Segmented neutrophils (predominant) ║
║ - Band cells ║
║ - Metamyelocytes ║
║ - Myelocytes ← MOST PREDOMINANT IMMATURE FORM ║
║ - Promyelocytes ║
║ - Myeloblasts (< 10% in chronic phase) ║
║ ║
║ • BASOPHILIA - increased basophils (CHARACTERISTIC) ║
║ • EOSINOPHILIA - increased eosinophils ║
║ • THROMBOCYTOSIS (platelets often markedly ↑) ║
║ • Mild normochromic normocytic ANEMIA ║
║ • Nucleated RBCs may be seen ║
║ ║
║ SPECIAL TEST: ║
║ • Leukocyte Alkaline Phosphatase (LAP) score ║
║ → MARKEDLY DECREASED / LOW (key distinguisher) ║
║ → Leukemoid reaction: LAP score HIGH ║
╚══════════════════════════════════════════════════════╝
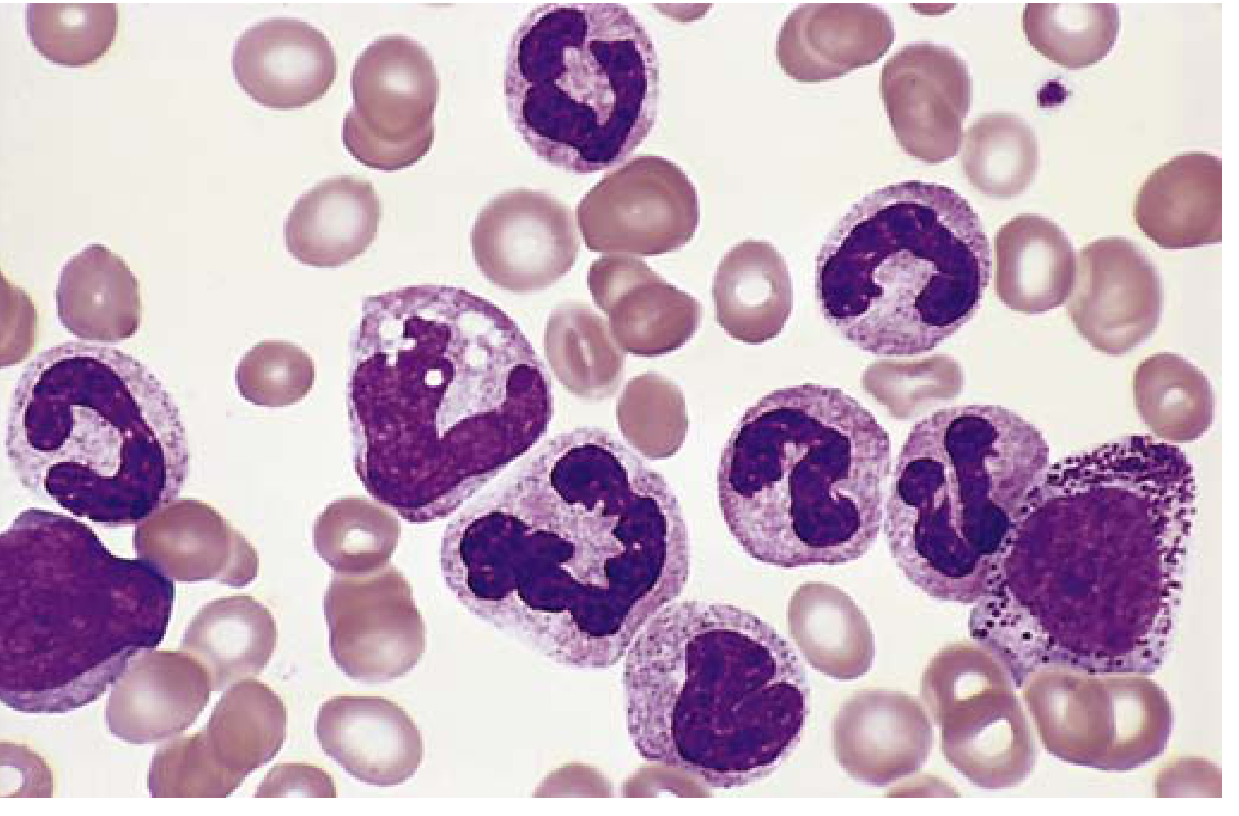
Fig: CML - Peripheral blood smear. Shows neutrophils and immature granulocytic precursors (myelocytes, metamyelocytes, band forms), basophils, and eosinophils at various stages of differentiation. (Robbins Basic Pathology)
BONE MARROW FINDINGS - CML
╔══════════════════════════════════════════════════════╗
║ CML - BONE MARROW FINDINGS ║
╠══════════════════════════════════════════════════════╣
║ GROSS: ║
║ • MARKEDLY HYPERCELLULAR ║
║ • Fatty marrow replaced by cellular marrow ║
║ • Increased myeloid:erythroid ratio (10:1 or more) ║
║ ║
║ MICROSCOPY: ║
║ • Massively increased granulocytic precursors ║
║ (myelocytes predominate) ║
║ • Megakaryocytes INCREASED - often small, ║
║ dysplastic (dwarf megakaryocytes) ║
║ • Erythroid precursors - normal or mildly ↓ ║
║ • SEA-BLUE HISTIOCYTES - characteristic finding ║
║ (macrophages with abundant wrinkled, green-blue ║
║ cytoplasm - pseudo-Gaucher cells) ║
║ • Increased reticulin deposition (mild) ║
║ • Blasts < 10% (chronic phase) ║
║ • Eosinophils and basophils increased ║
╚══════════════════════════════════════════════════════╝
Clinical Features of CML
Onset: Insidious
Symptoms:
- Fatigue, weakness, weight loss, anorexia (hypermetabolism)
- Dragging sensation/heaviness in left hypochondrium - due to massive splenomegaly (most characteristic)
- Left upper quadrant pain (splenic infarction)
- Night sweats
Signs:
- Massive splenomegaly (most prominent finding - due to extramedullary hematopoiesis)
- Hepatomegaly (mild-moderate)
- Sternal tenderness (marrow expansion)
- Lymphadenopathy (mild)
Lab findings:
- WBC: >100,000/μL with full myeloid spectrum
- LAP score: Low/absent (important exam fact)
- Ph chromosome (BCR-ABL): POSITIVE
- Uric acid: elevated (hyperuricemia from cell turnover)
- Vitamin B12 levels: elevated (from WBC)
Natural History / Phases of CML
CHRONIC PHASE (3-4 years average)
↓ (additional mutations)
ACCELERATED PHASE (6-12 months)
- Increasing anemia & thrombocytopenia
- Basophilia ↑↑
- Blasts 10-19%
- New cytogenetic abnormalities
↓
BLAST CRISIS (resembles acute leukemia)
- Blasts ≥ 20% (WHO criterion)
- 70% = Myeloid blast crisis (AML-like)
- 30% = Lymphoid blast crisis (B-ALL-like)
→ This proves CML arises from pluripotent HSC
Treatment: Imatinib (Gleevec) - tyrosine kinase inhibitor targeting BCR-ABL - revolutionized CML treatment; induces sustained remission.
PART D: ACUTE LEUKEMIAS - FAB CLASSIFICATION
Background
The French-American-British (FAB) Cooperative Group published the classification in 1976 based on morphology of Romanowsky-stained blood/marrow films and cytochemical stains. Though now superseded by WHO classification, FAB remains standard for MUHS examination.
FAB CLASSIFICATION OF ALL (L1-L3)
(Already detailed above in Part B)
FAB CLASSIFICATION OF AML (M0-M7)
╔══════════════════════════════════════════════════════════════════════╗
║ FAB CLASSIFICATION OF AML (M0 - M7) ║
╠═══════╦═══════════════════════════════╦═══════════════════════════╗ ║
║ FAB ║ NAME ║ KEY FEATURES ║ ║
╠═══════╬═══════════════════════════════╬═══════════════════════════╣ ║
║ M0 ║ AML, Minimally Differentiated ║ No differentiation; ║ ║
║ ║ ║ MPO negative by cytochem; ║ ║
║ ║ ║ Myeloid markers by flow ║ ║
╠═══════╬═══════════════════════════════╬═══════════════════════════╣ ║
║ M1 ║ AML without maturation ║ >3% MPO+ blasts; ║ ║
║ ║ ║ <10% maturing cells ║ ║
╠═══════╬═══════════════════════════════╬═══════════════════════════╣ ║
║ M2 ║ AML with maturation ║ ≥10% maturing granulocytes║ ║
║ ║ ║ t(8;21); Auer rods ║ ║
╠═══════╬═══════════════════════════════╬═══════════════════════════╣ ║
║ M3 ║ Acute Promyelocytic Leukemia ║ HYPERGRANULAR ║ ║
║ ║ (APL) ║ PROMYELOCYTES; MULTIPLE ║ ║
║ ║ ║ AUER RODS (faggot cells); ║ ║
║ ║ ║ t(15;17) PML-RARA; ║ ║
║ ║ ║ DIC common; ATRA therapy ║ ║
╠═══════╬═══════════════════════════════╬═══════════════════════════╣ ║
║ M4 ║ Acute Myelomonocytic Leukemia ║ Both myeloid + monocytic ║ ║
║ ║ (AMMoL) ║ differentiation; ║ ║
║ ║ ║ ≥20% monocytic component; ║ ║
║ ║ ║ inv(16) in M4Eo ║ ║
╠═══════╬═══════════════════════════════╬═══════════════════════════╣ ║
║ M5 ║ Acute Monocytic Leukemia ║ ≥80% monocytic cells; ║ ║
║ ║ ║ gum infiltration & skin ║ ║
║ ║ ║ rash (leukemia cutis) ║ ║
╠═══════╬═══════════════════════════════╬═══════════════════════════╣ ║
║ M6 ║ Acute Erythroid Leukemia ║ >50% dysplastic erythroid ║ ║
║ ║ (Di Guglielmo disease) ║ precursors; PAS positive ║ ║
║ ║ ║ erythroblasts ║ ║
╠═══════╬═══════════════════════════════╬═══════════════════════════╣ ║
║ M7 ║ Acute Megakaryoblastic ║ Blasts with megakaryocytic║ ║
║ ║ Leukemia ║ markers (CD41, CD61); ║ ║
║ ║ ║ Marrow fibrosis; Down ║ ║
║ ║ ║ syndrome association ║ ║
╚═══════╩═══════════════════════════════╩═══════════════════════════╝ ║
╚══════════════════════════════════════════════════════════════════════╝
MUHS EXAM MNEMONIC: "My Mother Makes Perfectly Moist Fried Muffins"
M0-Minimal, M1-Myeloblastic no maturation, M2-Myeloblastic with maturation, M3-Promyelocytic, M4-Myelomonocytic, M5-Monocytic, M6-Erythroid, M7-Megakaryoblastic
PART E: ACUTE MYELOID LEUKEMIA (AML) - DETAILED
Definition
AML is a clonal neoplasm of myeloid progenitors caused by acquired mutations that block differentiation, leading to accumulation of immature myeloid blasts in the marrow and blood.
Epidemiology
- Most common acute leukemia in adults (peak age: >60 years)
- Incidence rises with age (10/100,000 per year after age 60)
- Risk factors: benzene exposure, radiation, prior cytotoxic therapy, smoking
Diagnostic criterion: ≥ 20% myeloid blasts in blood or bone marrow
PERIPHERAL BLOOD SMEAR - AML
╔══════════════════════════════════════════════════════╗
║ AML - PERIPHERAL BLOOD SMEAR ║
╠══════════════════════════════════════════════════════╣
║ • Normocytic normochromic ANEMIA ║
║ • THROMBOCYTOPENIA ║
║ • WBC: variable (↑, normal, or ↓) ║
║ ║
║ MYELOBLASTS (key cells to identify): ║
║ • Large cells (larger than lymphoblasts) ║
║ • Abundant cytoplasm (more than ALL) ║
║ • AUER RODS: eosinophilic rod-shaped cytoplasmic ║
║ inclusions (fused primary granules) ║
║ → PATHOGNOMONIC of AML (NEVER in ALL) ║
║ → Most prominent in M3 (APL) - "faggot cells" ║
║ → Stain +ve: MPO, Sudan Black B, CAE, acid phosph ║
║ • Prominent nucleoli (3-5 usually) ║
║ • Fine (uncondensed) nuclear chromatin ║
║ • Cytoplasmic azurophilic granules ║
║ ║
║ "LEUKAEMIC HIATUS" (seen in AML): ║
║ • Gap between blasts and mature forms ║
║ • Intermediate forms (promyelocytes, myelocytes) ║
║ markedly reduced ║
╚══════════════════════════════════════════════════════╝
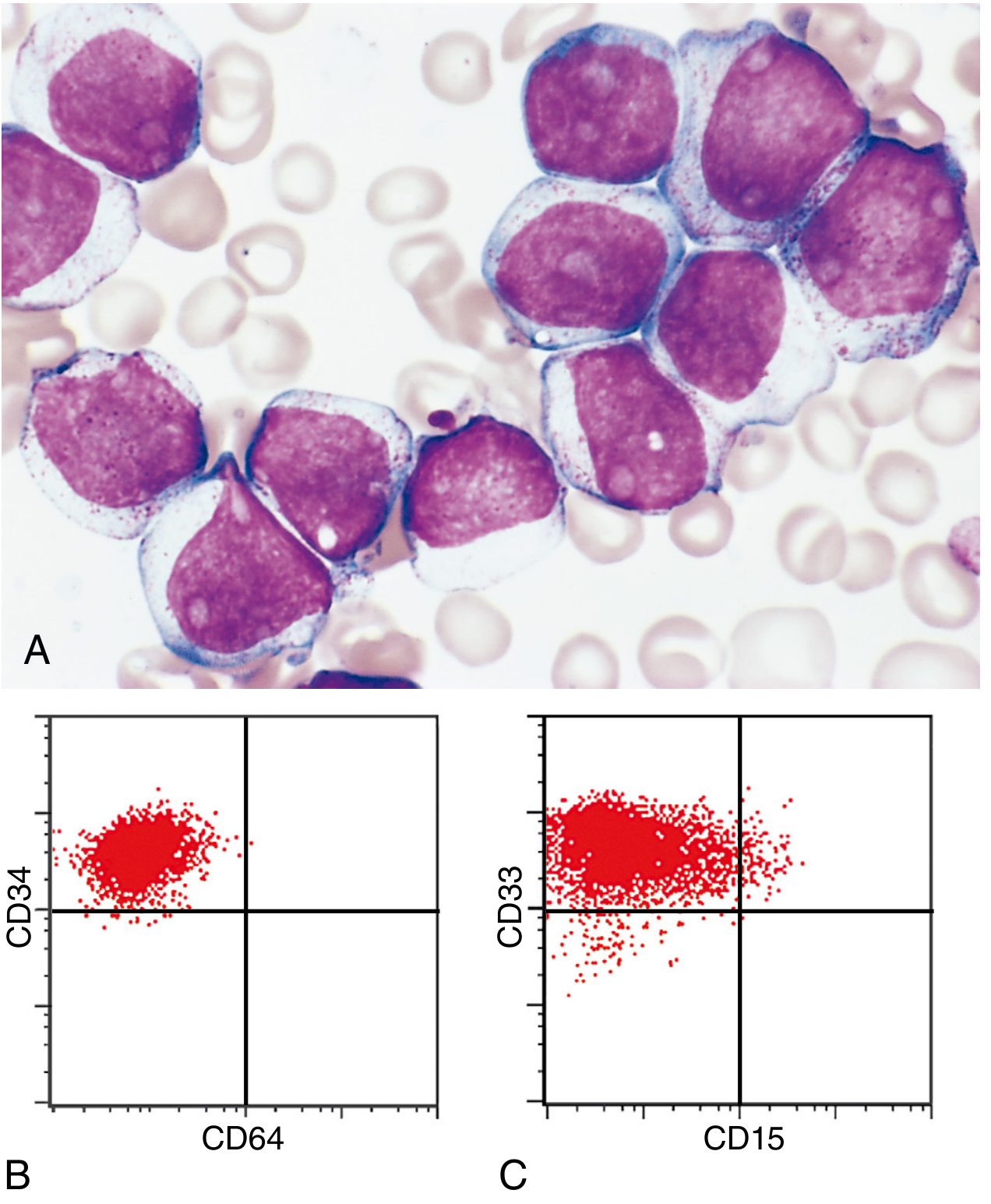
Fig: AML myeloblasts (A) with prominent nucleoli and azurophilic granules; (B-C) Flow cytometry showing CD34+ and CD33+ myeloid blasts confirming myeloid lineage. (Robbins, Cotran & Kumar)
BONE MARROW FINDINGS - AML
╔══════════════════════════════════════════════════════╗
║ AML - BONE MARROW FINDINGS ║
╠══════════════════════════════════════════════════════╣
║ GROSS: ║
║ • HYPERCELLULAR (packed marrow) ║
║ • Normal architecture replaced by blasts ║
║ • Grey-white appearance (loss of fat cells) ║
║ ║
║ MICROSCOPY: ║
║ • ≥ 20% myeloblasts (often 60-100%) ║
║ • Large blasts with: ║
║ - Delicate nuclear chromatin ║
║ - 3-5 prominent nucleoli ║
║ - Fine azurophilic cytoplasmic granules ║
║ - AUER RODS (pathognomonic) ║
║ • Normal precursors (RBC, WBC, platelet) REPLACED ║
║ • In M3: Hypergranular promyelocytes, faggot cells ║
║ • In M5: Monoblasts with folded/irregular nuclei ║
║ • In M7: Megakaryoblasts + marrow fibrosis ║
║ ║
║ CYTOCHEMICAL STAINS (KEY FOR MUHS EXAM): ║
║ • MPO (Myeloperoxidase) - POSITIVE (>3% blasts) ║
║ • Sudan Black B (SBB) - POSITIVE ║
║ • Chloroacetate Esterase (CAE) - POSITIVE ║
║ • Non-specific esterase (NSE/ANAE) - POSITIVE ║
║ (especially in M4 & M5 monocytic types) ║
║ • NSE inhibited by NaF = monocytic lineage ║
║ • PAS - variable (block positive in M6 erythroid) ║
║ • TdT - NEGATIVE (positive only in ALL) ║
╚══════════════════════════════════════════════════════╝
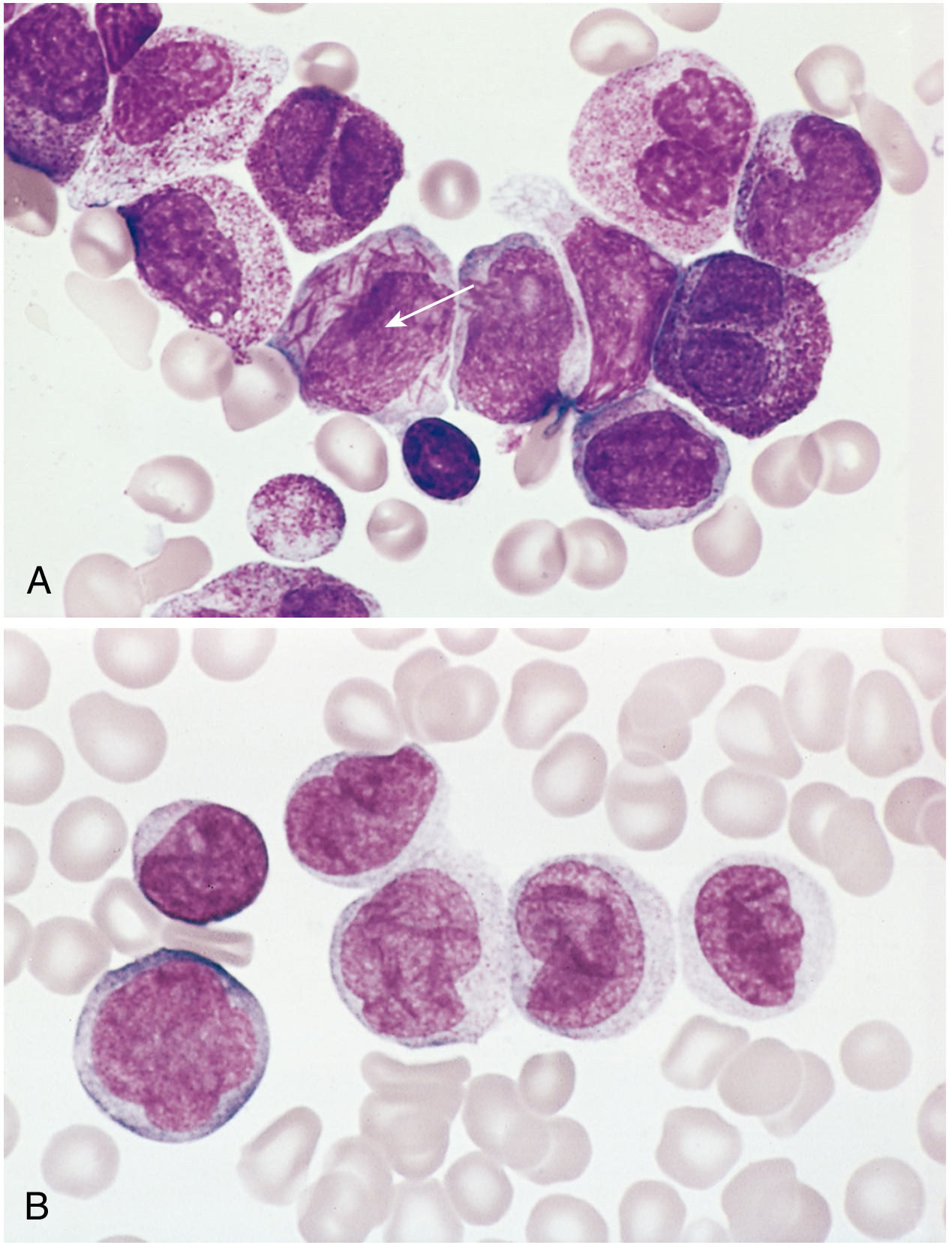
Fig: AML subtypes. (A) APL (M3/t(15;17)): hypergranular promyelocytes, bilobed nuclei, and faggot cells (multiple Auer rods, arrow). (B) AML M5 monocytic: monoblasts and promonocytes with folded/indented nuclei. (Robbins, Cotran & Kumar)
PART F: CYTOCHEMICAL STAINS - SUMMARY TABLE (★★★ High Yield)
| Stain | AML | ALL | CML | Notes |
|---|
| MPO (Myeloperoxidase) | + | - | + (mature) | Most important for AML |
| Sudan Black B | + | - | + | Parallels MPO |
| CAE (Chloroacetate Esterase) | + | - | + | Granulocytic lineage |
| NSE (Non-specific Esterase) | + (M4, M5) | - | - | Monocytic; inhibited by NaF |
| PAS | Variable (+ M6) | + (block pattern) | - | Block pattern = B-ALL |
| TdT | - | + | - | Nuclear; HALLMARK of ALL |
| Acid phosphatase | - | + (T-ALL) | - | T-ALL specific |
MUHS exam tip: TdT positive = ALL (lymphoblastic). MPO/SBB positive = AML (myeloblastic). This is the single most tested cytochemistry point.
PART G: COMPARISON TABLE - AML vs ALL (MUHS Favourite)
| Feature | AML | ALL |
|---|
| Age | Adults (>60 yr) | Children (peak 3-5 yr) |
| Cell of origin | Myeloid progenitor | Lymphoid precursor |
| Blasts | Myeloblasts | Lymphoblasts |
| Auer rods | PRESENT | ABSENT |
| TdT | Negative | POSITIVE |
| MPO/SBB | Positive | Negative |
| PAS | Variable | Block positive |
| NSE | + (monocytic) | Negative |
| CD markers | CD13, CD33, CD117, MPO | CD10 (CALLA), CD19, TdT |
| CNS involvement | Less common | More common |
| Gum infiltration | Yes (M4, M5) | No |
| Prognosis | Worse overall | Better (especially in children) |
| Philadelphia chr | Rare (<5%) | 25% adults (poor prognosis) |
PART H: LABORATORY FINDINGS - ACUTE LEUKEMIA (LAQ TOPIC)
General Lab Findings in ALL/AML:
- CBC: Anemia (normocytic normochromic), thrombocytopenia, variable WBC
- Peripheral smear: Blasts present, reduced normal cells
- Bone marrow: ≥20% blasts, hypercellular
- Cytochemistry: As above table
- Immunophenotyping (flow cytometry): Definitive lineage assignment
- Cytogenetics/FISH: Prognostic significance (t(15;17) = good, t(9;22) = poor)
- Serum: Elevated LDH, uric acid, potassium (tumor lysis)
- Coagulation: DIC in APL (M3) - prolonged PT, PTT, low fibrinogen, raised FDP
PART I: DIAGRAM SUMMARY FOR EXAM DRAWING
Easy-to-Draw CML Blood Smear Diagram:
NORMAL BLOOD: CML BLOOD SMEAR:
O O O O O O O O O ← RBCs (normal/↓)
O O O O O O O O O
[N] [N][N][N] ← Neutrophils (↑↑)
[Band][Meta] ← Band + metamyelocytes
[Myelo] ← Myelocytes (↑↑↑)
[B][Eo] ← Basophils + Eosinophils (↑)
[Blast] ← Myeloblasts (<10%)
◆ ◆ ◆ ← Platelets (↑↑)
Note: "Full Myeloid Spectrum" - hallmark of CML
Note: LAP score LOW (leukemoid reaction = HIGH)
Easy-to-Draw AML Myeloblast:
AML MYELOBLAST (for exam):
╭──────────────╮
╱ Large round ╲
│ nucleus with │
│ 3-5 PROMINENT │
│ NUCLEOLI │
│ │
╲ AUER ROD ╱
│ ══════► │ ← Auer rod (eosinophilic, rod-shaped)
╰──────────╯
Abundant cytoplasm
with azurophilic granules
KEY: Auer rods = pathognomonic of AML
Lymphoblast in ALL (for exam):
ALL LYMPHOBLAST:
╭──────╮
╱ LARGE ╲
│ nucleus │ ← fine/stippled chromatin
│ (fills │
│ most of │ ← nucleolus: absent(L1) or
│ cell) │ prominent(L2/L3)
╲ ╱
╰────╮──╯
SCANT cytoplasm
(very little compared to AML)
KEY: NO Auer rods; TdT POSITIVE
QUICK REVISION - HIGH-YIELD MUHS EXAM POINTS
| Point | Answer |
|---|
| Most common cancer in children | ALL |
| Philadelphia chromosome | t(9;22) - BCR-ABL - seen in CML (100%) and B-ALL (25% adults) |
| Pathognomonic of AML | Auer rods |
| Hallmark marker of ALL | TdT (Terminal deoxynucleotidyl transferase) |
| LAP score in CML | LOW (vs HIGH in leukemoid reaction) |
| CML blast crisis | ≥20% blasts; 70% myeloid, 30% lymphoid |
| Sea-blue histiocytes | CML bone marrow |
| DIC in leukemia | AML-M3 (APL) with t(15;17) |
| Best prognosis AML | M3 (APL) - treated with ATRA + arsenic trioxide, >90% curable |
| Treatment of CML | Imatinib (Gleevec) - BCR-ABL tyrosine kinase inhibitor |
| FAB blast cutoff | ≥20% (WHO) / classically ≥30% in old FAB - exam usually asks WHO |
| Gum infiltration | AML M4/M5 (monocytic differentiation) |
| CNS sanctuary site | ALL (requires intrathecal chemotherapy prophylaxis) |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (10th Ed.); Robbins & Kumar Basic Pathology; Henry's Clinical Diagnosis and Management by Laboratory Methods; structured for MUHS 2nd MBBS Pathology examination.