Explain the whole development of The gut tube and body cavities along with all clinicals
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, authoritative content. Let me compose the full detailed answer.
Development of the Gut Tube and Body Cavities
Sources: Langman's Medical Embryology, The Developing Human (Moore), Fischer's Mastery of Surgery
Part 1: Overview - A Tube on Top of a Tube
During the 3rd and 4th weeks, two fundamental tubular structures form almost simultaneously:
- The dorsal tube - the neural tube (brain + spinal cord), formed by neurulation of the ectoderm
- The ventral tube - the gut tube, formed by folding of the endoderm
The middle layer - mesoderm - holds both tubes together and forms the body cavity between them.
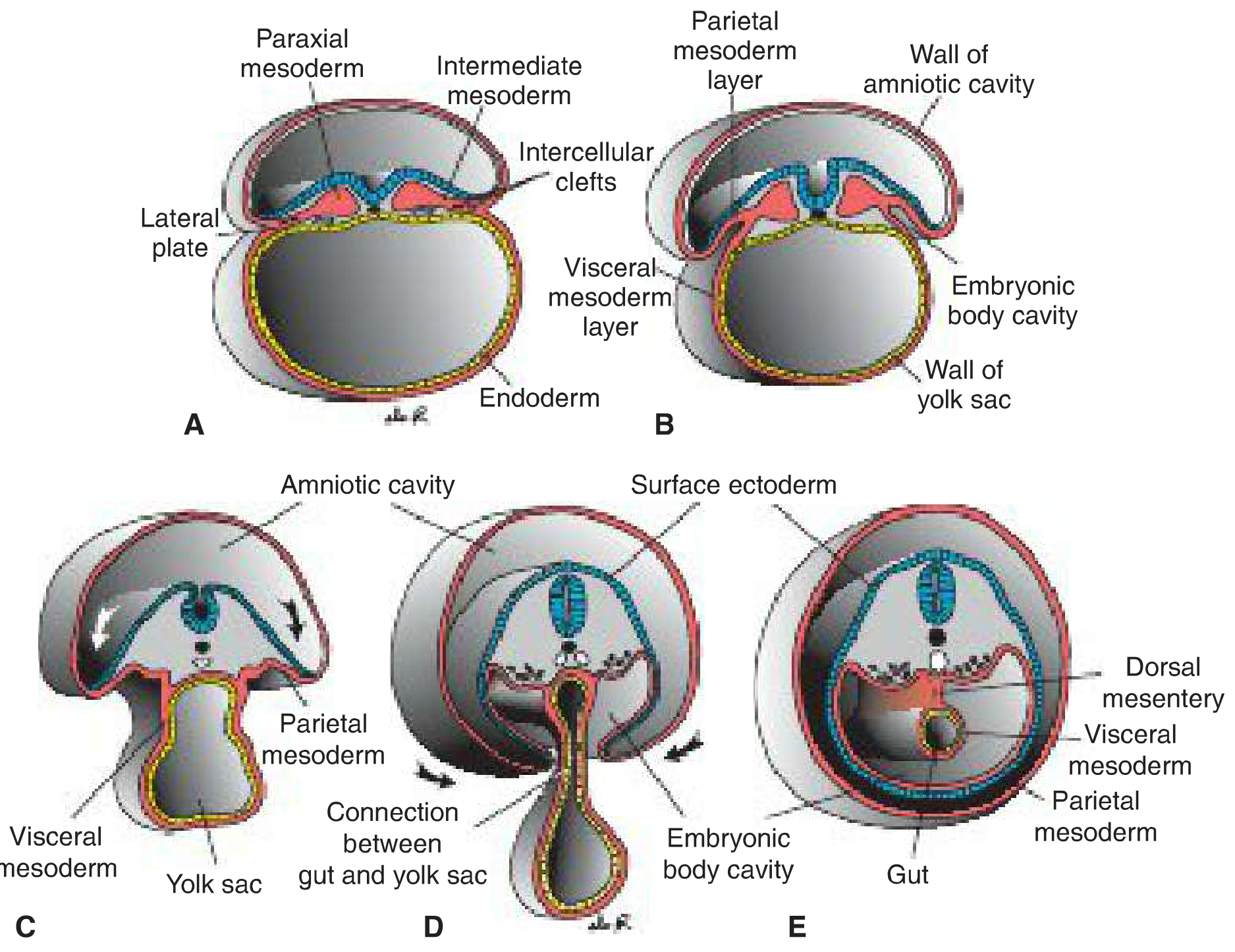
Transverse sections through an embryo at various stages of gut tube and body wall closure (Langman's, p. 116)
Part 2: Formation of the Primitive Body Cavity (Intraembryonic Coelom)
Week 3 - Lateral Plate Mesoderm Splits
By the end of the third week, intraembryonic mesoderm differentiates into three zones:
- Paraxial mesoderm - somitomeres and somites (skull + vertebrae)
- Intermediate mesoderm - urogenital system
- Lateral plate mesoderm - body cavity formation
Intercellular clefts appear in the lateral plate mesoderm and coalesce, splitting it into two layers:
| Layer | Name | Also Called | Covers |
|---|---|---|---|
| Outer (adjacent to surface ectoderm) | Parietal (somatic) layer | Somatopleure | Lines future body wall |
| Inner (adjacent to endoderm) | Visceral (splanchnic) layer | Splanchnopleure | Surrounds gut tube |
The space between these two layers is the primitive body cavity (intraembryonic coelom).
Week 4 - Horseshoe-Shaped Coelom
By the fourth week, the intraembryonic coelom becomes a horseshoe-shaped cavity:
- The cranial bend represents the future pericardial cavity
- Its lateral limbs extend to become the future pleural and peritoneal cavities
- The distal parts of each limb communicate with the extraembryonic coelom at the lateral edges of the embryonic disc - this communication allows the normal physiological herniation of the midgut into the umbilical cord later
Part 3: Formation of the Gut Tube
As the lateral body wall folds develop during week 4, the endoderm layer simultaneously folds ventrally to form the gut tube. The process is as follows:
- Lateral body wall folds - parietal mesoderm + overlying ectoderm - grow ventrally on each side
- The endoderm rolls down and its edges close in the ventral midline, forming a sealed tube
- The folds meet and fuse in the midline by the end of week 4, closing the ventral body wall
- Closure is complete everywhere except:
- The region of the connecting stalk (future umbilical cord)
- The midgut-yolk sac connection, the vitelline (yolk sac) duct, which is incorporated into the umbilical cord and degenerates between months 2 and 3
The resulting gut tube is lined entirely by endoderm and is divided into three regions based on blood supply:
| Region | Blood Supply | Derivatives |
|---|---|---|
| Foregut | Celiac artery | Pharynx, esophagus, stomach, duodenum (proximal), liver, gallbladder, pancreas |
| Midgut | Superior mesenteric artery | Duodenum (distal), jejunum, ileum, cecum, appendix, ascending colon, transverse colon (proximal 2/3) |
| Hindgut | Inferior mesenteric artery | Transverse colon (distal 1/3), descending colon, sigmoid, rectum, upper anal canal |
The gut is bounded at either end by ectoderm-lined depressions:
- Cranially: the stomodeum (future mouth), initially separated from the foregut by the oropharyngeal membrane (ruptures ~day 26)
- Caudally: the proctodeum (future anus), separated by the cloacal membrane (ruptures ~week 7)
Part 4: Molecular Regulation of Gut Tube Development
Regional identity along the gut tube is established by a retinoic acid (RA) concentration gradient, with low RA at the pharyngeal end and high RA at the colonic end. This drives expression of region-specific transcription factors:
| Region | Transcription Factor |
|---|---|
| Esophagus + stomach | SOX2 |
| Duodenum | PDX1 |
| Small intestine | CDXC |
| Large intestine + rectum | CDXA |
This initial patterning is then stabilized by epithelial-mesenchymal interactions:
- The endoderm secretes Sonic Hedgehog (SHH) throughout the gut tube
- SHH induces a nested expression of HOX genes in the surrounding visceral (splanchnic) mesoderm
- The HOX-coded mesoderm then instructs the endoderm to differentiate into the specific gut segment
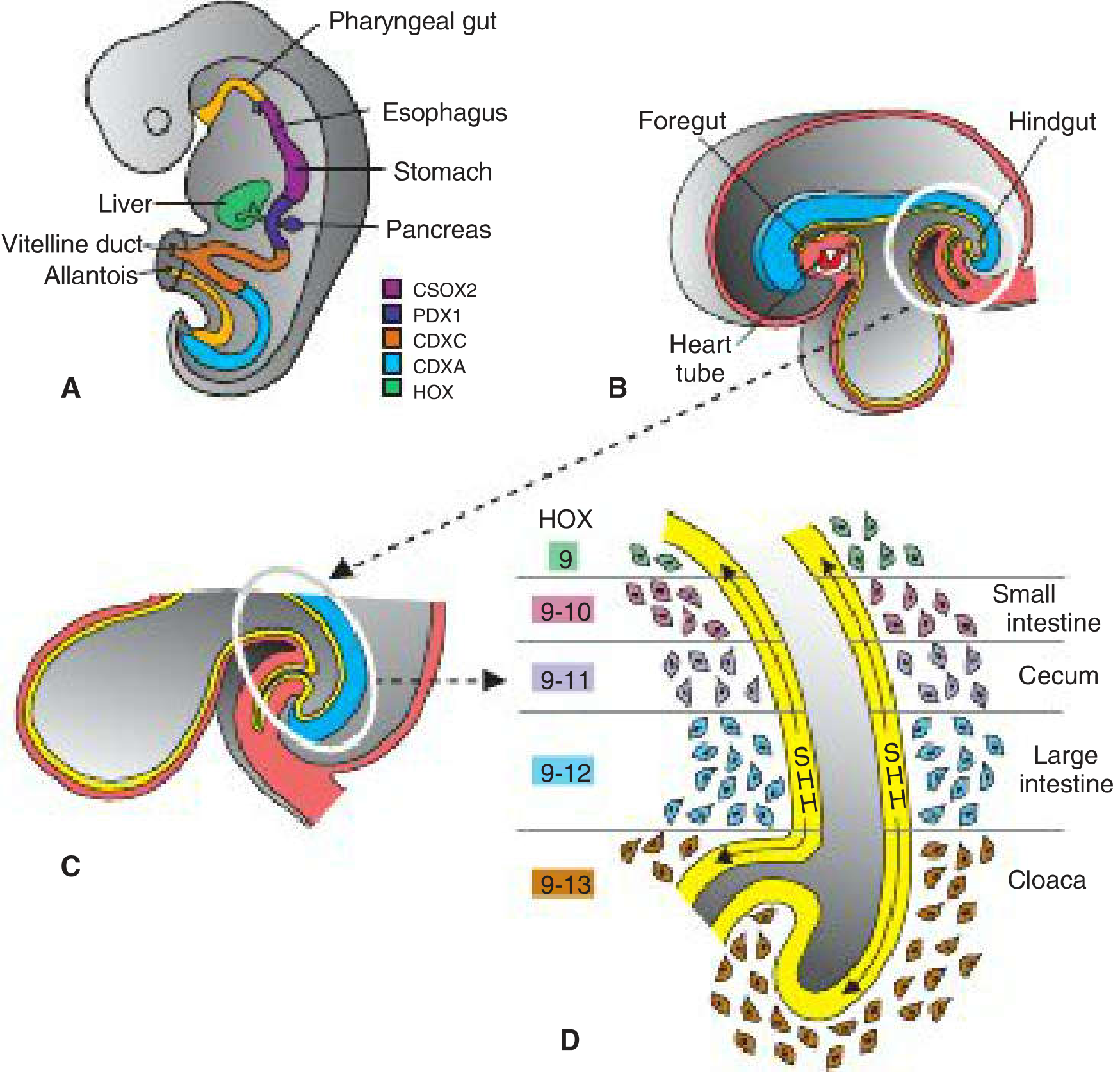
Color-coded diagram showing transcription factor zones (A) and SHH-HOX stabilization cascade (B-D). (Langman's, p. 251)
Part 5: Serous Membranes and Mesenteries
Serous Membranes
Once the primitive body cavity forms, cells of the lateral plate mesoderm become mesothelial and generate serous membranes:
- Parietal layer - lines the body wall (parietal peritoneum, parietal pleura, serous pericardium)
- Visceral layer - covers organs (visceral peritoneum, visceral pleura, epicardium)
Dorsal Mesentery
The visceral and parietal layers are continuous at the point where the gut tube meets the posterior body wall - this double-layered peritoneal fold is the dorsal mesentery. It:
- Extends continuously from the lower esophagus to the rectum
- Provides a pathway for blood vessels, lymphatics, and nerves to reach the gut
- Is regionally named according to the part of gut it suspends:
| Region | Mesentery Name |
|---|---|
| Stomach | Dorsal mesogastrium (becomes greater omentum) |
| Duodenum | Mesoduodenum |
| Small intestine | Mesentery proper |
| Transverse colon | Transverse mesocolon |
| Sigmoid colon | Mesosigmoid |
| Rectum | Mesorectum |
Ventral Mesentery
Derived from mesenchyme of the septum transversum. As the liver grows into the septum, it divides the ventral mesentery into:
- Lesser omentum (ventral mesogastrium) - from stomach/proximal duodenum to liver
- Falciform ligament - from liver to ventral body wall (carries the ligamentum teres = remnant of left umbilical vein)
Clinical importance: The dorsal mesentery is a continuous structure. This is critical during cancer surgery - resection of tumors in the abdomen must respect the mesenteric planes. The Toldt fascia is a fascial plane between visceral and parietal peritoneum that forms when organs (like the ascending/descending colon) become secondarily retroperitoneal; surgeons exploit this avascular plane during colectomy.
Part 6: Division of the Body Cavity - Separation into Three Compartments
The primitive single body cavity is divided into pericardial, pleural, and peritoneal cavities by a sequence of partitions.
Step 1: Head Fold Repositions the Pericardial Cavity
During the head fold in week 4, the pericardial region swings ventrally to lie anterior to the foregut. The septum transversum, originally at the level of the cervical segments, is carried down by this movement to the position of the future diaphragm.
Step 2: Septum Transversum
- Grows dorsally from the ventrolateral body wall
- Forms a thick incomplete connective tissue partition between the pericardial and peritoneal cavities
- Does not completely separate them - leaves two openings: the pericardioperitoneal canals on each side of the foregut
- Later becomes the central tendon of the diaphragm
Step 3: Separation of Pleural Cavities - Pleuropericardial Membranes
When the lung buds begin growing (week 5), they expand caudolaterally within the pericardioperitoneal canals. As the lungs expand, they grow into the body wall mesenchyme - posteriorly, then laterally and ventrally.
- Small ridges called pleuropericardial folds form, projecting into the undivided thoracic cavity
- These folds expand and contain the common cardinal veins and phrenic nerves
- Descent of the heart pulls these folds medially in a mesentery-like fashion
- They fuse with each other and with the root of the lungs to form the pleuropericardial membranes
- This divides the thoracic cavity into the pericardial cavity + two pleural cavities
- The pleuropericardial membranes form the fibrous pericardium in the adult
Step 4: Separation of Pleural and Peritoneal Cavities - Formation of the Diaphragm
The diaphragm is formed from four components:
| Component | Contribution |
|---|---|
| Septum transversum | Central tendon (anterior/central portion) |
| Dorsal mesentery of esophagus | Median portion; myoblasts form the crura |
| Pleuroperitoneal membranes | Posterolateral portions (large in fetus, small in newborn) |
| Body wall mesenchyme (weeks 9-12) | Peripheral dome (costal part) - from somatic mesoderm |
Sequence of Closure:
- Pleuroperitoneal folds project into the caudal pericardioperitoneal canals (week 5)
- They grow medially, becoming the pleuroperitoneal membranes by week 7
- These fuse with the mesentery of the esophagus (forming the crura)
- Then fuse with the septum transversum - completing the partition
- Weeks 9-12: Lungs burrow into lateral body walls, splitting them into: (a) outer layer = definitive abdominal wall; (b) inner layer = peripheral diaphragm
- This process creates the costodiaphragmatic recesses and the characteristic dome shape
Innervation of the Diaphragm:
- Phrenic nerve (C3, C4, C5) - motor to the entire diaphragm + sensory to central portion
- The early diaphragm (septum transversum) forms at the cervical level and descends to L1 by week 8, carrying its cervical nerves with it - hence the long thoracic course of the phrenic nerve
- Thoracic nerves T7-T12 - sensory to the peripheral diaphragm (from body wall origin)
Part 7: Clinical Correlations
1. Congenital Diaphragmatic Hernia (CDH) - Bochdalek Hernia
Mechanism: Failure of the pleuroperitoneal membranes to fuse with the other diaphragm components, leaving a large posterolateral opening (lumbocostal triangle = foramen of Bochdalek).
Key facts:
- Incidence: ~1 in 2200-5000 births
- Left-sided in 85-90% of cases (right pleuroperitoneal opening closes earlier)
- Abdominal viscera (stomach, intestines, liver) herniate into the thoracic cavity
- Ipsilateral lung is compressed and hypoplastic (the most common cause of pulmonary hypoplasia)
- Contralateral lung also shows morphologic changes
- Heart and mediastinum displaced to the right
- Associated pulmonary hypertension (decreased vascular cross-section) and potential right-to-left shunting
- Treatment of pulmonary hypertension: inhaled nitric oxide (potent pulmonary vasodilator)
- Genetics: Chromosome 15q26 (GATA6), GATA4, ZFPM2, NR2F2, WT1; deletions at 8p23.1 and 4p16.3
- Prenatal detection: ultrasound + MRI showing abdominal organs in thorax
- Mortality primarily from pulmonary hypoplasia and hypertension, not the hernia itself
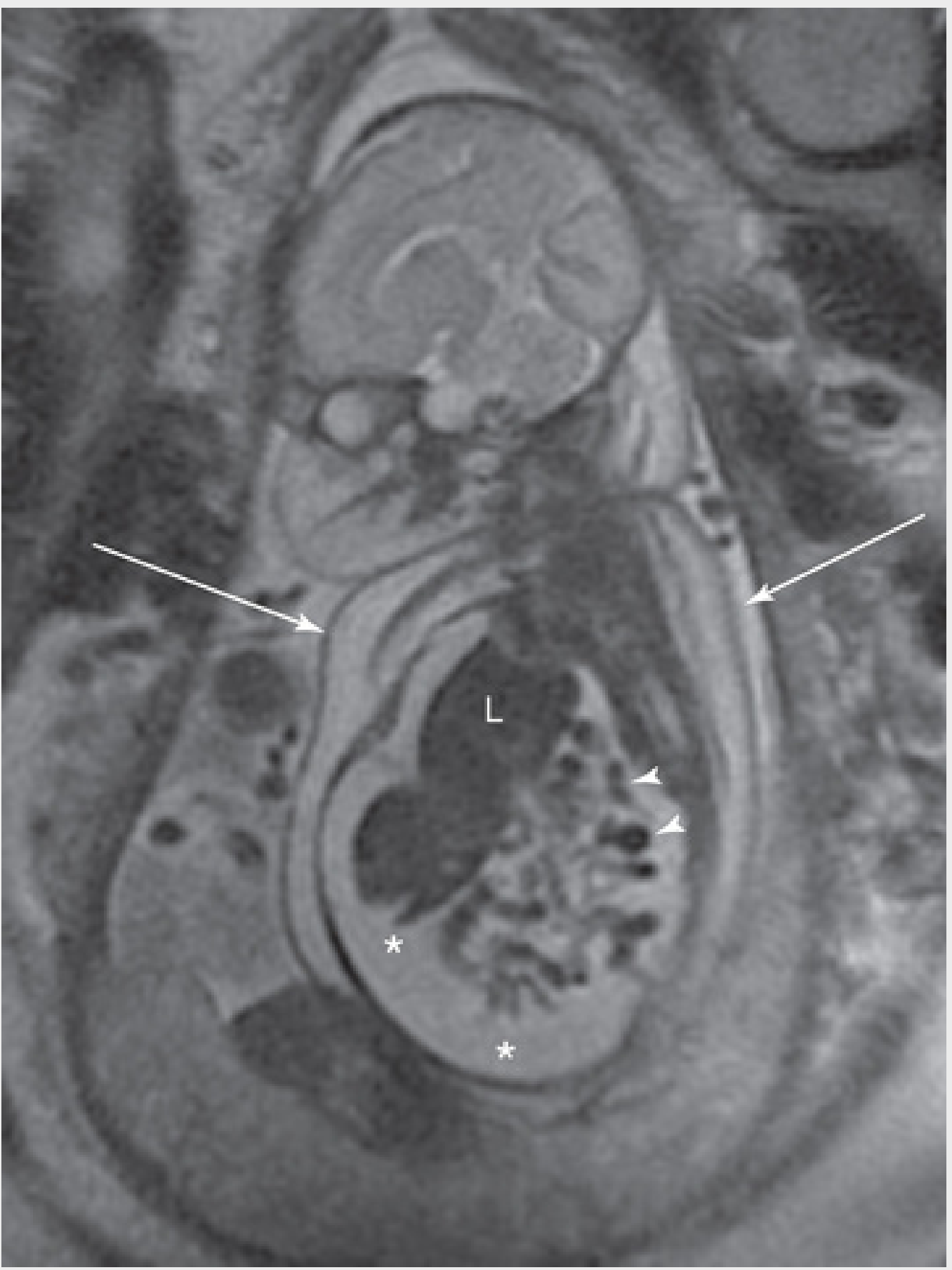
MRI of a fetus with right-sided CDH: liver (L) and bowel loops (arrowheads) in the thorax. (The Developing Human, p. 444)
2. Morgagni Hernia (Retrosternal/Parasternal Hernia)
Mechanism: Herniation through the sternocostal hiatus (foramen of Morgagni) - the gap between the sternal and costal parts of the diaphragm, normally occupied by the superior epigastric vessels.
Features:
- Less common than Bochdalek hernia
- Located anteriorly (vs Bochdalek which is posterior)
- May contain intestine entering the pericardial sac, or occasionally part of the heart descending into the peritoneal cavity
- Large defects are associated with umbilical body-wall defects
- Small fatty herniations through this hiatus are common incidental findings with no clinical significance
Mnemonic: "Bochdalek is Back and Big; Morgagni is Midline/Minor"
3. Eventration of the Diaphragm
Mechanism: Failure of muscular tissue from the body wall to extend into the pleuroperitoneal membrane on one side - resulting in an aponeurotic (membranous) sheet that balloons superiorly into the thorax.
Features:
- Half the diaphragm has defective musculature
- Abdominal viscera displaced upward into a pouch-like outpouching
- NOT a true herniation (viscera remain within a sac of diaphragmatic tissue)
- Clinical manifestations may simulate CDH
- Some cases are acquired (phrenic nerve injury)
4. Hiatal Hernia (Congenital Predisposition)
Mechanism: Herniation of part of the stomach through an excessively large esophageal hiatus in the diaphragm.
Features:
- Usually acquired in adult life, but a congenitally enlarged esophageal hiatus may be the predisposing structural factor
- Types: Sliding (type I - most common), paraesophageal (type II), mixed (type III/IV)
- Symptoms: GERD, dysphagia, chest pain
5. Gastroschisis
Mechanism: Failure of the lateral body wall folds to completely fuse in the ventral midline during week 4. Results in a full-thickness defect in the anterior abdominal wall.
Features:
- Incidence: ~1 in 3000 live births
- Defect is to the right of the umbilical cord (not truly midline)
- Bowel is uncovered (no peritoneal sac) and floats freely in amniotic fluid
- Chemical peritonitis from amniotic fluid exposure causes a characteristic "peel" on the bowel surface
- Detected prenatally on routine ultrasound
6. Congenital Epigastric Hernia
Mechanism: Same as gastroschisis - incomplete fusion of lateral body wall folds - but less severe.
Features:
- Located in the midline between xiphoid and umbilicus
- Bowel remains covered by skin and subcutaneous tissue (vs gastroschisis)
- No amniotic fluid exposure
7. Omphalocele (Exomphalos)
Mechanism: Failure of the physiological herniation of the midgut to return to the abdominal cavity by week 11, OR failure of the lateral body folds to close around the umbilicus properly.
Features:
- Bowel is in the umbilical cord, covered by a peritoneal sac (amnion + peritoneum)
- Defect is at the umbilicus (unlike gastroschisis which is paraumbilical)
- Associated with chromosomal anomalies (trisomy 13, 18) and other malformations
- Sac may contain liver, bowel, and other viscera
Key distinction:
- Omphalocele: midline, covered by sac, associated with other anomalies
- Gastroschisis: right of umbilicus, no sac, bowel in amniotic fluid, usually isolated
8. Persistent Vitelline (Meckel's) Diverticulum
Mechanism: The vitelline (yolk sac) duct fails to degenerate after week 7 and persists as a fingerlike projection of the ileum.
Features (Rule of 2s):
- Occurs in 2% of population
- Located 2 feet (60 cm) proximal to the ileocecal valve
- Approximately 2 inches long
- Usually symptomatic before age 2
- Contains 2 types of ectopic mucosa (gastric and pancreatic most common)
- Ectopic gastric mucosa causes ulceration and painless rectal bleeding
- Can also cause intussusception, volvulus, or Meckel's diverticulitis (mimics appendicitis)
- Diagnosed with Tc-99m pertechnetate scan (Meckel's scan)
9. Congenital Peritoneopericardial Communication
Mechanism: Failure of complete fusion of the pleuropericardial membranes with foregut mesoderm - leaves abnormal communication between peritoneal and pericardial cavities.
Features: Extremely rare; may present with cardiac tamponade from herniated bowel
10. Referred Pain from the Diaphragm
A key clinical pearl related to diaphragm development: the central diaphragm descends from cervical (C3-C5) segments, so irritation of the diaphragm (e.g., by sub-phrenic abscess, ectopic pregnancy, or bile leak) causes referred pain to the shoulder tip (C4 dermatome = tip of shoulder).
Summary Table
| Event | Timing | Key Structure |
|---|---|---|
| Lateral plate mesoderm splits into 2 layers | End of week 3 | Intraembryonic coelom forms |
| Horseshoe-shaped coelom | Week 4 | Pericardial cavity + limbs |
| Lateral body wall folds close gut tube | Week 4 | Gut tube sealed; vitelline duct persists temporarily |
| Head fold rotates pericardial cavity ventrally | Week 4 | Septum transversum descends |
| Pleuropericardial membranes fuse | Week 5-6 | Pericardial + pleural cavities separated |
| Pleuroperitoneal membranes fuse | Week 7 | Diaphragm primordium complete |
| Midgut herniates into umbilical cord | Week 6 | Physiological umbilical hernia |
| Body wall muscle grows into peripheral diaphragm | Weeks 9-12 | Costal diaphragm + costodiaphragmatic recesses |
| Midgut returns to abdominal cavity | Week 11 | Gut tube fully intra-abdominal |
| Vitelline duct degenerates | Months 2-3 | Meckel's diverticulum if it persists |
- Langman's Medical Embryology, pp. 116-117, 121, 251-253
- The Developing Human: Clinically Oriented Embryology, pp. 424-451
- Fischer's Mastery of Surgery - 8th Ed., pp. 8259-8262
This is a shared conversation. Sign in to Orris to start your own chat.