give me the note of corneal ulcer from basic to advanced level from the standard textbooks and add images to it, any clinical trials and recent advances. write it in chat
"corneal ulcer" AND treatment
🔬 Corneal Ulcer - Comprehensive Clinical Notes
1. DEFINITION & OVERVIEW
- A simple epithelial defect is an erosion - once stromal involvement occurs, it is a true ulcer
- The cornea resists infection via an intact epithelium, tear film (lysozyme, lactoferrin, IgA), limbal vascularity, and blinking
Tintinalli's: "A corneal ulcer is a serious infection involving multiple layers of the cornea and develops secondary to breaks in the epithelial barrier, so that infectious agents invade the underlying corneal stroma."
2. ANATOMY RELEVANT TO CORNEAL ULCERS
- Epithelium (5-6 cell layers, non-keratinized) - first barrier; regenerates rapidly
- Bowman's layer - acellular condensed stroma; does NOT regenerate (scarring is permanent here)
- Stroma - 90% of corneal thickness; collagen lamellae; keratocytes
- Descemet's membrane - basement membrane of endothelium; very elastic (bulges as descemetocele when only it remains)
- Endothelium - single cell layer; fluid pump; cannot regenerate
3. ETIOLOGY & PATHOGENS
3.1 Bacterial (Most Common Overall)
| Organism | Notes |
|---|---|
| Pseudomonas aeruginosa | #1 in contact lens wearers; >60% of CL-related keratitis; aggressive, rapid progression |
| Staphylococcus aureus | Gram-positive commensal; focal, well-defined yellow-white infiltrate |
| Streptococcus pneumoniae | Upper respiratory commensal; often aggressive |
| S. pyogenes | Aggressive |
| Moraxella spp. | Alcoholics, immunocompromised |
| Neisseria gonorrhoeae | Can penetrate INTACT epithelium; hyperpurulent conjunctivitis preceding |
| N. meningitidis, C. diphtheriae, H. influenzae | Can also penetrate intact epithelium |
3.2 Viral
| Organism | Features |
|---|---|
| Herpes Simplex Virus (HSV) | Most common cause of central corneal ulcer; dendritic pattern |
| Herpes Zoster (VZV) | V1 distribution; pseudo-dendrite, neurotrophic ulcer |
| Adenovirus | Subepithelial infiltrates, no true ulcer usually |
3.3 Fungal
| Organism | Features |
|---|---|
| Fusarium, Aspergillus, other filamentous | Trauma with vegetable matter; satellite lesions; feathery margins |
| Candida | Immunocompromised, debilitated patients; dense yellow-white suppurative infiltrate |
3.4 Parasitic
| Organism | Features |
|---|---|
| Acanthamoeba spp. | Contact lens + tap water; severe pain disproportionate to signs; radial perineuritis pathognomonic |
| Onchocerca (river blindness) | Tropics; interstitial keratitis |
| Microsporida | Immunocompromised |
3.5 Non-Infectious (Sterile) Ulcers
- Neurotrophic keratopathy (loss of CN V sensation)
- Exposure keratopathy (Bell's palsy, proptosis)
- Autoimmune: Mooren's ulcer, peripheral ulcerative keratitis (PUK) in RA/Wegener's
- Chemical/thermal burns
- Vitamin A deficiency (keratomalacia)
- Rosacea keratitis
- Contact lens toxicity
4. RISK FACTORS
- Contact lens wear (most important - esp. extended wear, overnight use, soft lenses; poor hygiene)
- Ocular surface disease (dry eye, entropion, trichiasis, blepharitis)
- Corneal anaesthesia (CN V lesion, post-herpetic)
- Previous ocular surgery (LASIK, PRK, keratoplasty)
- Trauma (vegetable matter = suspect fungi)
- Topical steroid use
- Systemic immunosuppression (HIV, diabetes, malnutrition)
- Vitamin A deficiency (developing world)
- Exposure keratopathy
Kanski's: "Contact lens wear, particularly if extended, is the most important risk factor... Wearers of soft lenses are at higher risk than those wearing rigid gas permeable... Infection is more likely if there is poor lens hygiene, but it can also occur even with apparently meticulous lens care and with daily disposable lenses."
5. CLINICAL FEATURES
5.1 Symptoms
- Ocular pain (may be severe - especially in Acanthamoeba)
- Photophobia
- Lacrimation / watering
- Mucopurulent or watery discharge
- Blurred vision / reduced visual acuity (especially if central)
- Foreign body sensation
- Red eye (ciliary flush / circumcorneal injection)
5.2 Signs on Slit-Lamp Examination
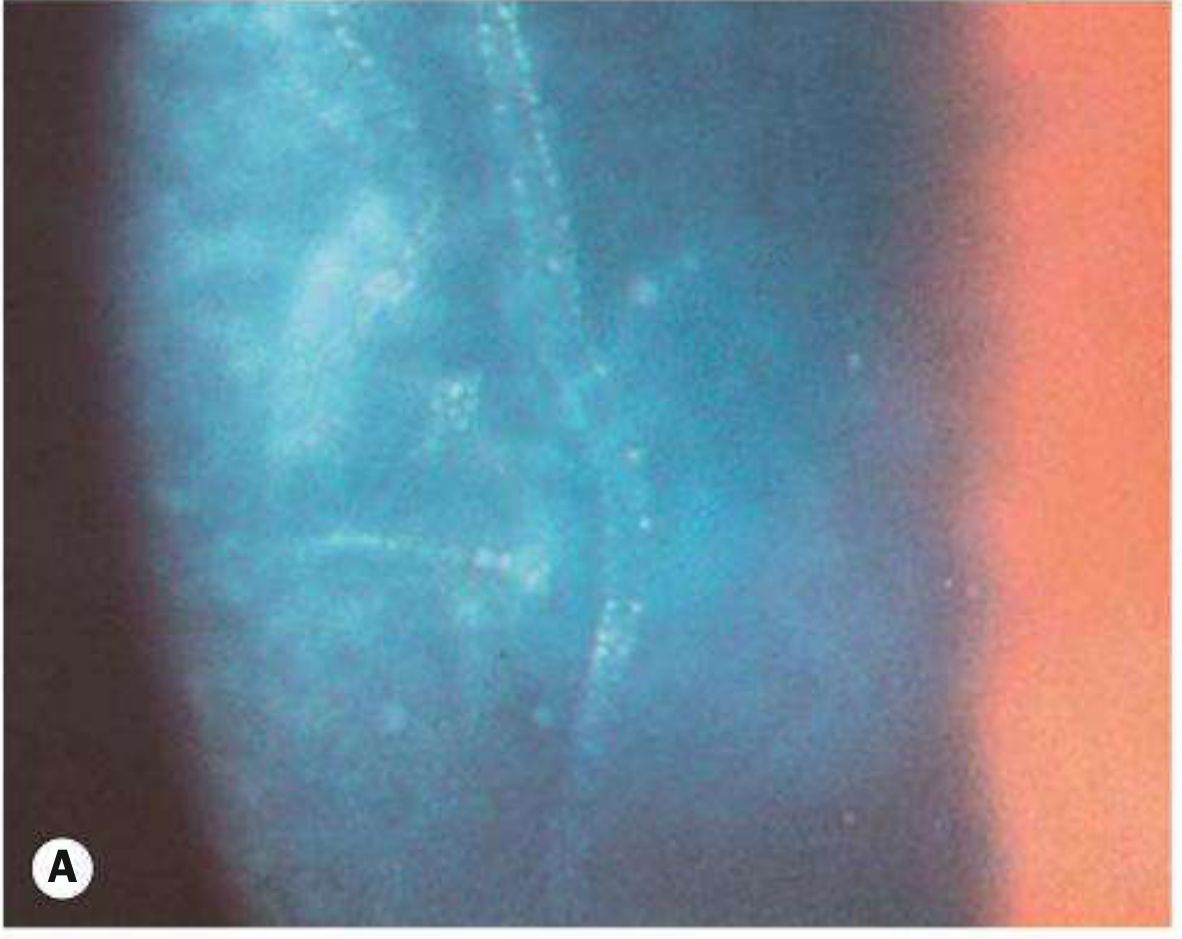
- Epithelial defect - stains with fluorescein (green); confirms breach
- Stromal infiltrate - white/grey hazy area; indicates WBC infiltration
- Corneal oedema - surrounding haze
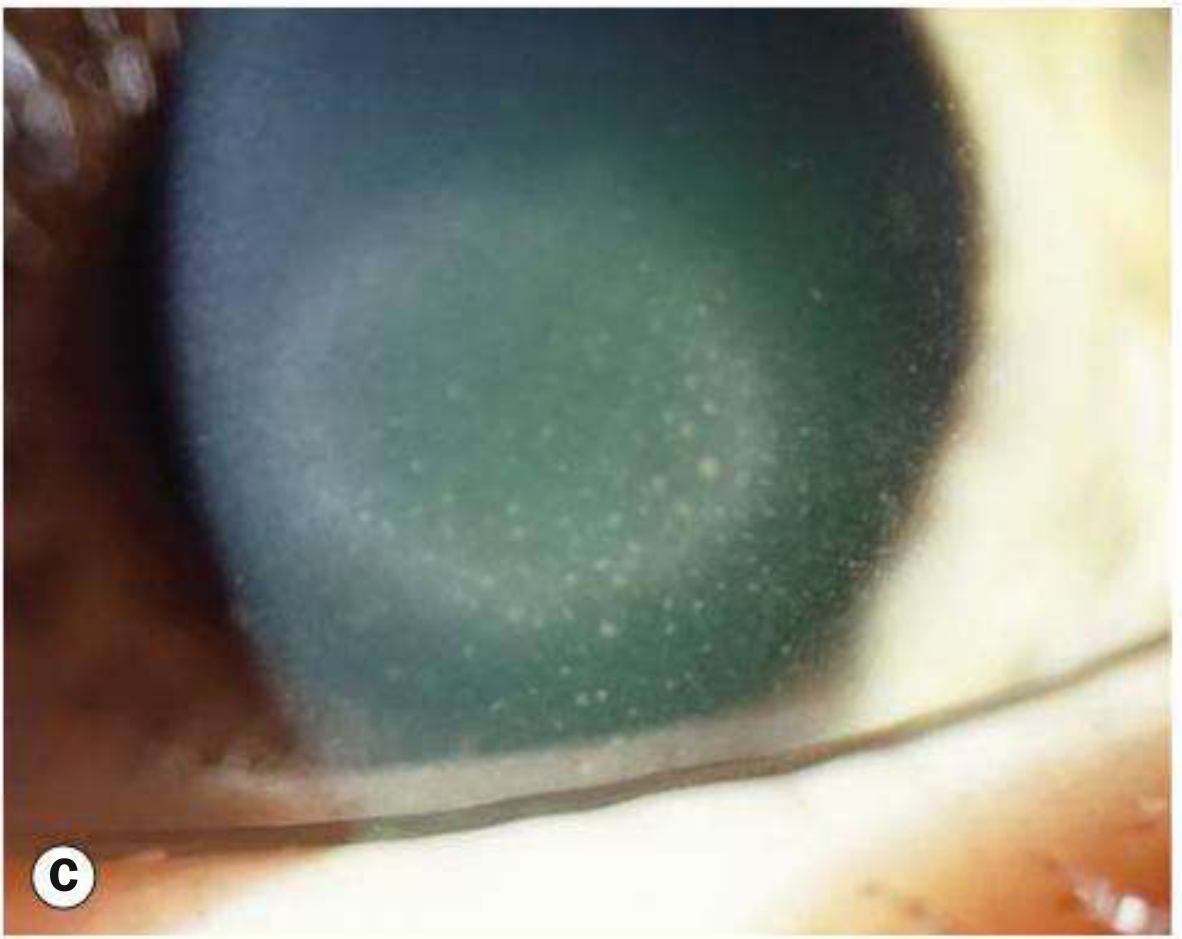
- Satellite lesions - secondary infiltrates (classic in fungi, but not exclusive)
- Hypopyon - layered sterile pus in anterior chamber (reactive); alarming sign
- Anterior uveitis - flare and cells (ciliary spasm causes consensual photophobia)
- Descemetocele - transparent bowing of Descemet's - imminent perforation
- Corneal vascularisation - in chronic disease
| Feature | Likely Cause |
|---|---|
| Dendritic ulcer with terminal buds; rose Bengal + margins | HSV |
| Pseudo-dendrite (no true terminal buds) | Acanthamoeba, VZV |
| Satellite lesions, feathery margins, raised epithelium | Fungal (filamentous) |
| Dense yellow-white suppurative infiltrate | Candida or bacterial |
| Radial perineuritis (pathognomonic) | Acanthamoeba |
| Ring abscess | Acanthamoeba (late), Pseudomonas |
| Rapid progression, contact lens user | Pseudomonas |
6. IMAGES
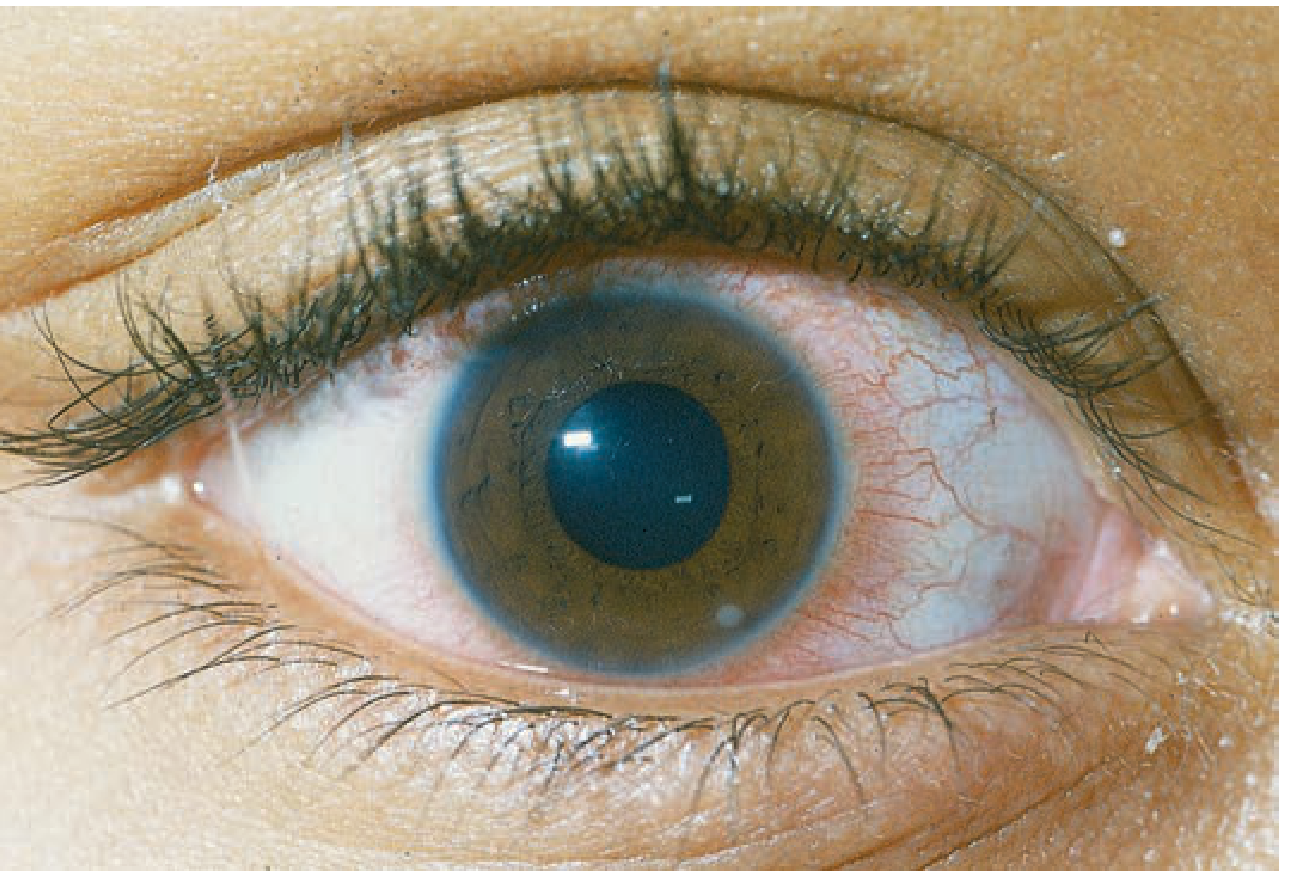
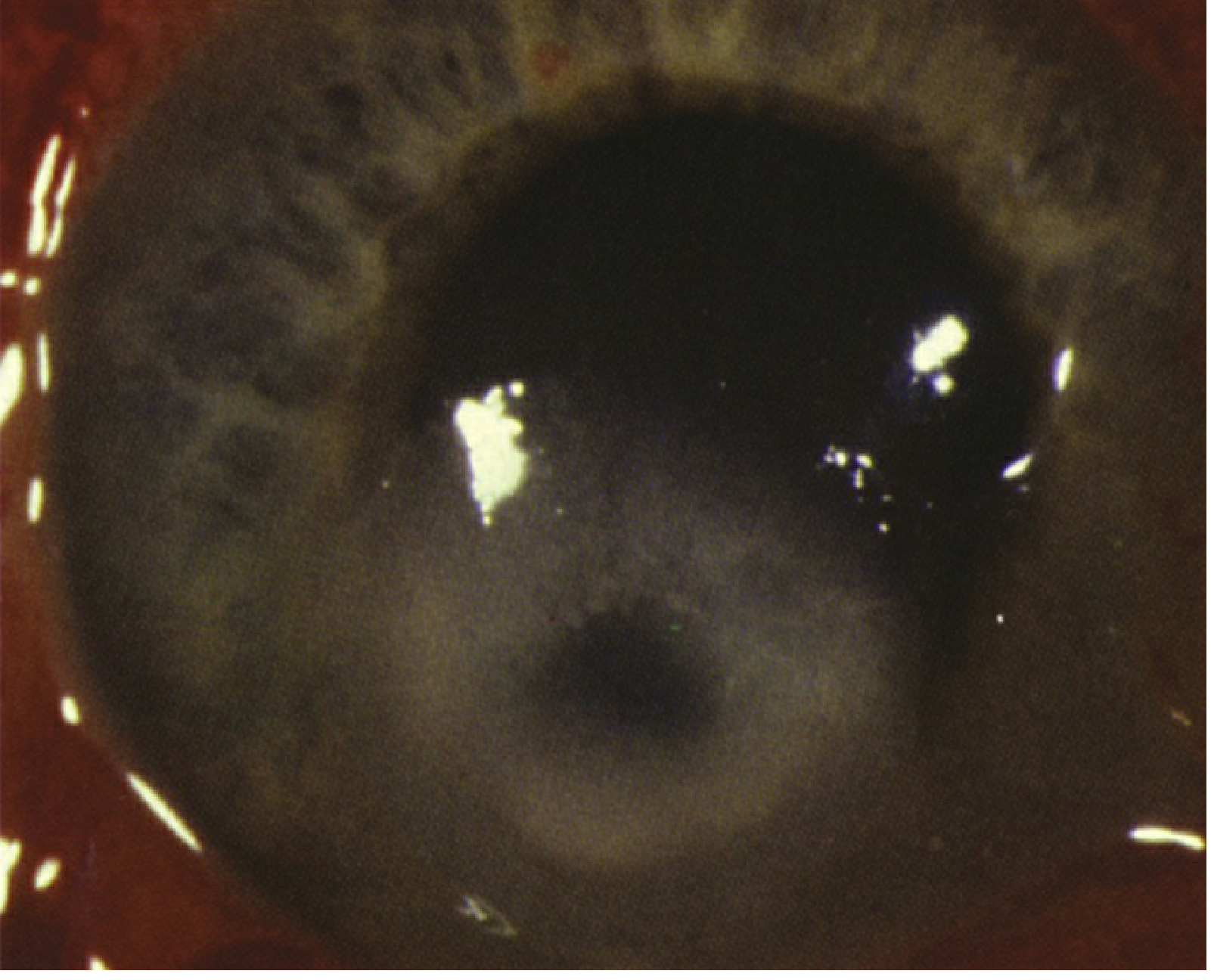
Clinical photo of corneal ulcer (5 o'clock position):
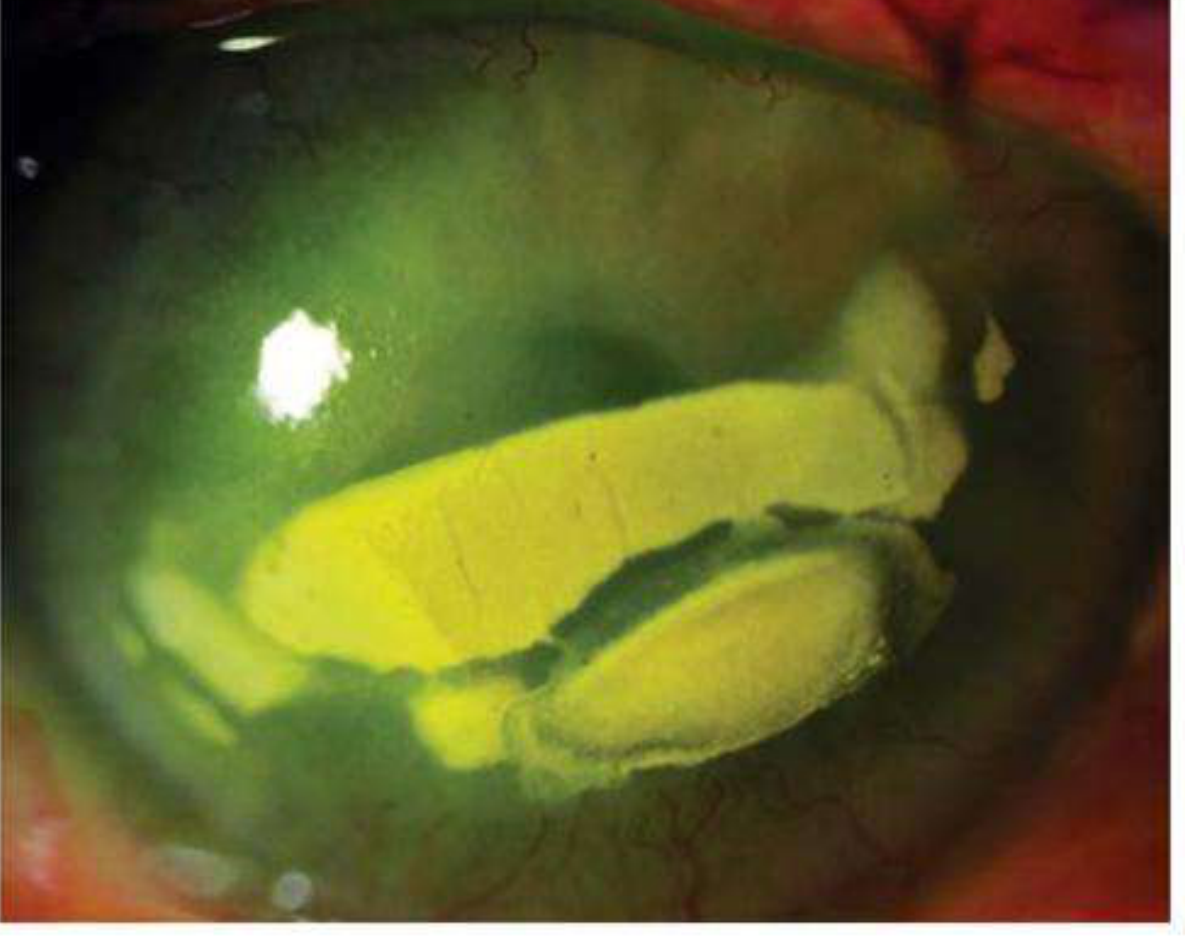
Fluorescein staining - large bacterial corneal ulcer:
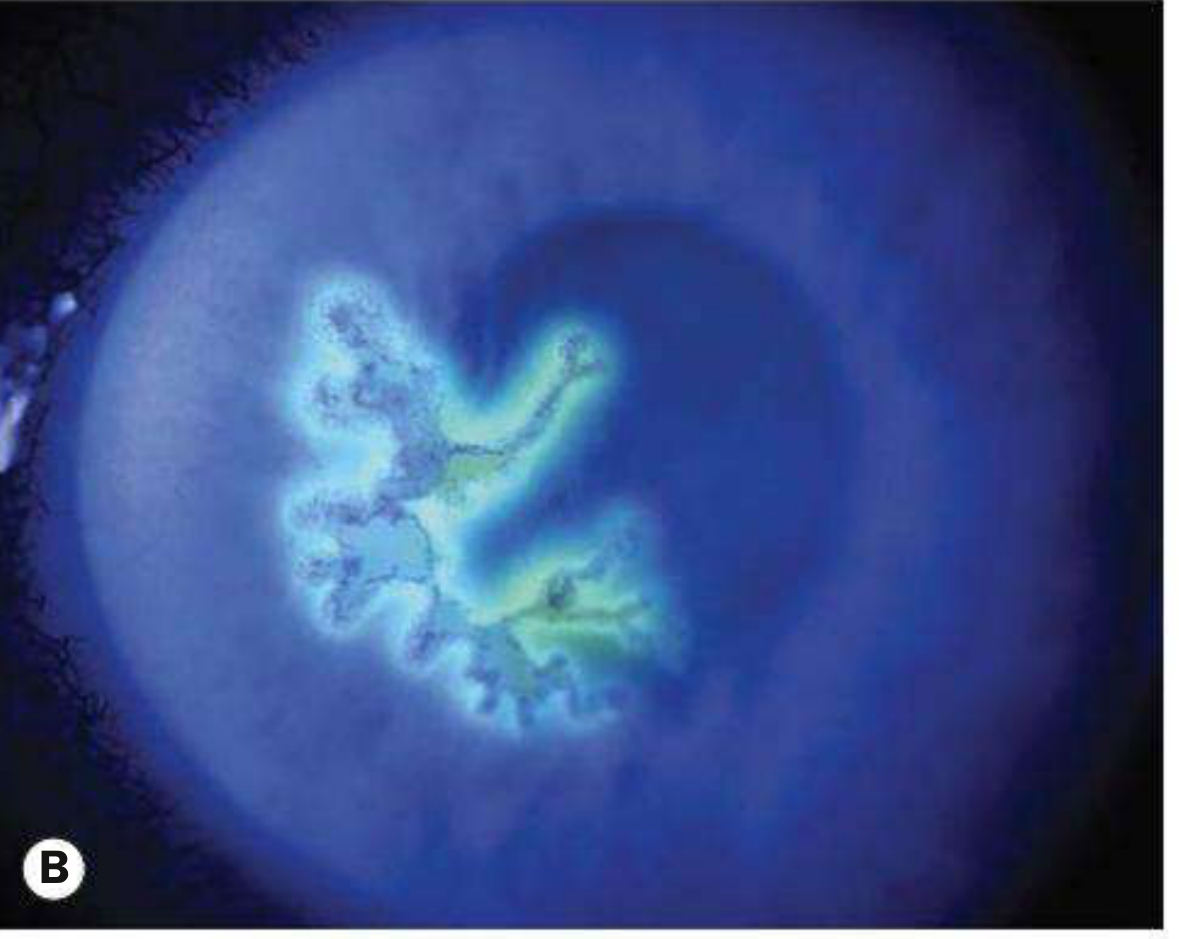
HSV dendritic ulcer - fluorescein:
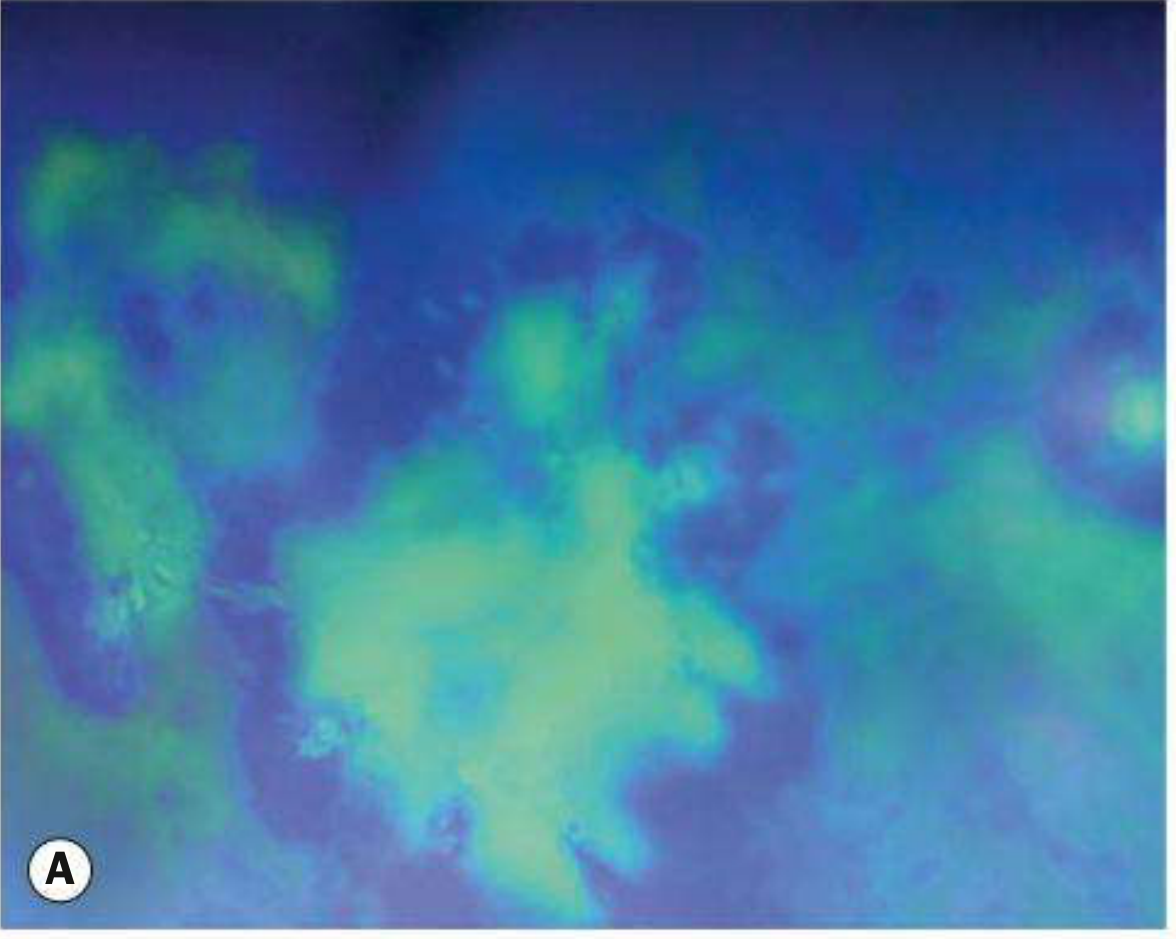
HSV geographic ulcer (post-steroid enlargement):
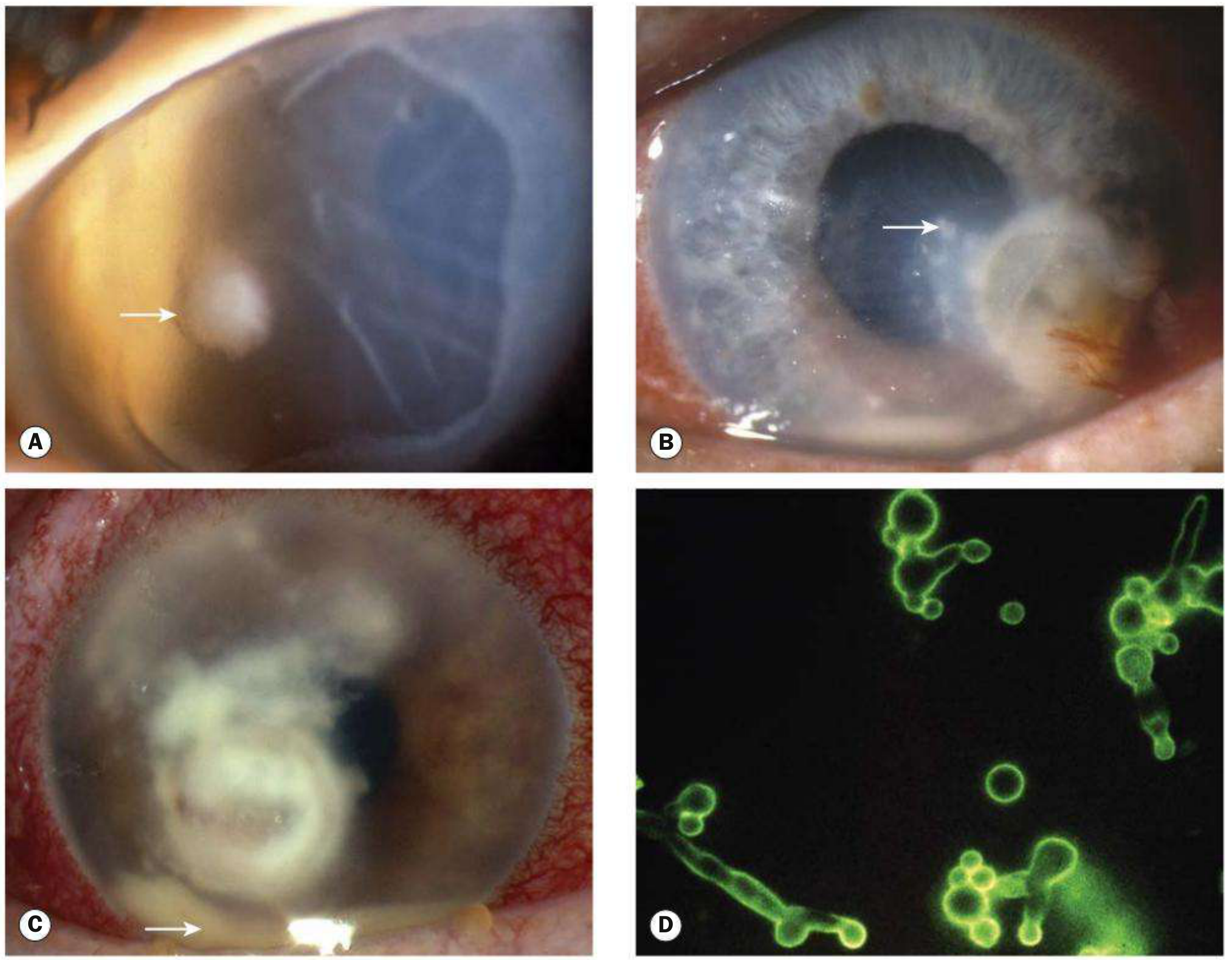
Fungal keratitis - key features:
7. DIAGNOSIS
7.1 History
- Duration, onset speed (rapid = bacterial/Pseudomonas; gradual = fungal/Acanthamoeba)
- Contact lens use + type + hygiene + solution type
- Prior herpes simplex/zoster
- Trauma (vegetable matter → fungal)
- Steroid use (topical or systemic)
- Immunosuppression
7.2 Examination
- Visual acuity (both eyes)
- Slit-lamp biomicroscopy with white light and cobalt blue filter after fluorescein
- Examine: infiltrate size, depth, margins, satellite lesions, AC reaction, hypopyon, IOP, iris, lens
- Rose Bengal - stains devitalized cells and virus-laden margins of HSV dendrites
- Corneal sensation - CN V testing with cotton wisp
7.3 Investigations (Corneal Scraping)
| Medium | Organism |
|---|---|
| Blood agar | Most bacteria and fungi |
| Chocolate agar | Fastidious bacteria (H. influenzae, Neisseria, Moraxella) |
| Sabouraud dextrose agar | Fungi |
| Non-nutrient agar + E. coli | Acanthamoeba |
| Brain-heart infusion | Difficult-to-culture organisms; streptococci; yeasts |
| Löwenstein-Jensen | Mycobacteria, Nocardia |
| Stain | Use |
|---|---|
| Gram stain | Bacteria (Gram+/-); ~60% sensitive |
| Giemsa | Bacteria, fungi, multinucleated giant cells (HSV) |
| KOH prep | Rapid fungal diagnosis; highly sensitive |
| Calcofluor white | Fungi and Acanthamoeba (fluorescent) |
| Periodic acid-Schiff (PAS) | Fungi, Acanthamoeba cysts |
| Methenamine silver | Fungi |
| Ziehl-Neelsen | Mycobacteria |
- In vivo confocal microscopy (IVCM) - non-invasive; can visualise Acanthamoeba cysts and fungal hyphae in real time
- PCR - highly sensitive for HSV, VZV, Acanthamoeba; nanopore sequencing identifies exact species + antibiotic resistance
- Corneal biopsy - for deep or unresponsive ulcers where scraping is negative
- Contact lens + case + solution for culture
8. TREATMENT
8.1 General Principles
- All ulcers should be treated aggressively
- Obtain cultures FIRST, then start empirical therapy
- Cycloplegic (cyclopentolate 1%, homatropine 2%, or atropine 1%) - prevents posterior synechiae formation and reduces ciliary spasm pain
- Never patch a contact lens-wearing patient (accelerates infection)
- Discontinue contact lenses immediately
8.2 Bacterial Keratitis
- Fluoroquinolone eye drops: ciprofloxacin 0.3%, ofloxacin 0.3%, levofloxacin 1.5%, moxifloxacin 0.5%, besifloxacin 0.6%
- Loading dose: 1 drop every 5-15 minutes for the first hour, then hourly day and night initially, tapering as response occurs
- Note: Ciprofloxacin can form white corneal precipitates (see image above) - this does not indicate treatment failure
- Fortified cephalosporin (cefazolin/cefuroxime 50 mg/mL) + fortified aminoglycoside (gentamicin 15 mg/mL or tobramycin 14 mg/mL)
- Alternated every 30 minutes (not simultaneously to avoid drug interaction)
- Cefazolin 50 mg/mL: 500 mg parenteral diluted in 2.5 mL sterile water + 7.5 mL preservative-free artificial tears
- Gentamicin 15 mg/mL: 2 mL parenteral (40 mg/mL) added to 5 mL commercial 0.3% gentamicin
- Controversial; the SCUT (Steroids for Corneal Ulcers Trial) showed no significant benefit overall, but patients with severe ulcers (CF vision or ulcers involving central 4 mm) tended to do better
- CONTRAINDICATED if fungal or mycobacterial infection suspected
- Use with caution: promotes HSV replication, retards epithelial healing
- For N. gonorrhoeae: ceftriaxone IV + azithromycin oral
- For HSV/VZV keratitis with systemic involvement
8.3 Fungal Keratitis
- Natamycin 5% drops - first-line; poorly penetrating but effective for filamentous; q1h initially
- Voriconazole 1% drops - better stromal penetration; effective for both filamentous and yeast
- Systemic voriconazole (200 mg BD orally) for deep/resistant cases
- Duration: Minimum 6-12 weeks; often longer
- Fluconazole (topical + systemic) or voriconazole
- Amphotericin B 0.15% drops for resistant cases
- Topical steroids are strictly contraindicated in fungal keratitis
- Natamycin showed superiority over voriconazole for Fusarium in the MUTT-I trial
- Penetrating keratoplasty (PKP) may be necessary for non-responding cases
8.4 Herpetic (HSV) Keratitis
- Topical antivirals: aciclovir 3% ointment 5x/day OR ganciclovir 0.15% gel 5x/day - continue for 14 days or 3 days after healing
- Oral aciclovir 400 mg 5x/day (especially for geographic ulcers or if topical poorly tolerated)
- Debridement of involved epithelium (historical; less preferred now)
- AVOID topical steroids in epithelial disease - causes expansion to geographic/amoeboid ulcer
- Topical steroids ARE used (prednisolone 0.5-1%)
- Antiviral cover mandatory when using steroids (prophylactic topical aciclovir)
- HEDS trials established role of oral aciclovir (400 mg BD) for recurrence prophylaxis (reduces recurrence by ~50%)
8.5 Acanthamoeba Keratitis
- Early diagnosis is critical - outcome much better with early treatment
- Epithelial debridement to aid drug penetration
- Topical amoebicides (cysticidal agents):
- Polyhexamethylene biguanide (PHMB) 0.02% - kills trophozoites AND cysts
- Chlorhexidine 0.02% - kills trophozoites AND cysts
- Hexamidine or propamidine (Brolene) - mainly anti-trophozoite
- Initial dosing: hourly day and night, then tapering over weeks-months
- Treatment duration: minimum 3-6 months
- Avoid topical steroids early; may help later for inflammatory scleritis/keratitis
- Confocal microscopy to monitor cyst clearance
- PKP as last resort after infection eradicated
8.6 Promotion of Epithelial Healing
- Preservative-free artificial tears and lubricating ointment
- Bandage contact lens (BCL) - mechanical protection of regenerating epithelium; must be supervised closely for superinfection
- Antibiotic ointment prophylaxis under BCL
- Tarsorrhaphy (temporary or permanent lateral): for exposure/neurotrophic ulcers
- Botulinum toxin ptosis: induces temporary (2-3 months) lid closure
- Conjunctival (Gundersen) flap: for chronic, poor visual prognosis eye
- Amniotic membrane graft (AMG): for persistent epithelial defects; multilayered transplant or patch grafting
- Cyanoacrylate tissue glue: seals small perforations; applied under BCL
- Limbal stem cell transplantation: if LSCD from chemical burns/cicatrizing conjunctivitis
8.7 Surgical Management
- Failed medical therapy
- Corneal perforation (actual or impending)
- Deep stromal involvement
- Descemetocele
- Cyanoacrylate glue + BCL - for small perforations (<2 mm)
- Patch graft (lamellar) - seals perforation, preserves anatomy
- Penetrating keratoplasty (PKP) - for larger perforations or failed medical treatment; "hot keratoplasty" for active infection carries high risk of graft failure
- Deep anterior lamellar keratoplasty (DALK) - if Descemet's is spared; avoids endothelial rejection risk
9. SPECIFIC CLINICAL SCENARIOS
9.1 Contact Lens-Related Ulcer
- Empirical broad-spectrum fluoroquinolone (moxifloxacin or ciprofloxacin)
- Never patch - risk of rapid Pseudomonas proliferation
- Culture before starting treatment
- Discard lenses and lens case
- Urgent ophthalmology referral
9.2 Post-Vegetation Trauma
- Suspect fungal keratitis; use KOH prep, culture on Sabouraud's
- Start natamycin 5% empirically
- Avoid steroids
9.3 Post-Refractive Surgery (LASIK)
- Flap interface keratitis (Sands of the Sahara) vs. infectious
- Mycobacteria, Nocardia, fungi are more common in LASIK-related infections
- Flap lift + irrigation of interface + targeted topical therapy
9.4 Neurotrophic/Exposure Ulcer
- Typically sterile with rolled edges, no infiltrate
- Treat underlying cause (tarsorrhaphy, lubricants)
- Cenegermin (recombinant NGF, Oxervate) - approved for neurotrophic keratopathy stages 2-3
- AMG or conjunctival flap for non-healing cases
10. COMPLICATIONS
- Corneal scarring - permanent if Bowman's layer breached; causes irregular astigmatism, leukoma
- Corneal vascularisation - complicates future corneal transplant (pre-sensitization)
- Descemetocele - thinning until only Descemet's remains; imminent perforation
- Corneal perforation - iris plugging, expulsive hemorrhage, endophthalmitis risk
- Hypopyon - anterior chamber pus (usually sterile, but may indicate intraocular involvement)
- Endophthalmitis - particularly with fungal keratitis (may penetrate Descemet's without perforation)
- Glaucoma - inflammatory angle closure, synechiae
- Cataract - from inflammation or surgical intervention
- Phthisis bulbi - end-stage, shrunken blind eye
11. PREVENTION
- Proper contact lens hygiene education
- No tap water use for lens cleaning or storage
- Daily disposable lenses preferred
- No sleeping in lenses
- Protective eyewear for agricultural/outdoor work
- Prophylactic antiviral (oral aciclovir 400 mg BD) for recurrent HSV keratitis
- Vitamin A supplementation in deficient populations
- Prompt treatment of ocular surface disease
12. RECENT CLINICAL TRIALS & ADVANCES
12.1 SCUT Trial (Steroids for Corneal Ulcers Trial)
- Large RCT; evaluated topical corticosteroids (prednisolone phosphate 1%) after 48h of antibiotics vs. placebo in bacterial keratitis
- Result: No significant overall benefit in visual acuity at 3 months; trend toward benefit in severe central ulcers
- The SCUT II Trial (NCT, Prajna et al., Cornea 2024, PMID 39208371) is ongoing - evaluates adjunctive corneal cross-linking AND/OR topical difluprednate in smear-positive bacterial ulcers (280 enrolled)
12.2 MUTT Trials (Mycotic Ulcer Treatment Trials)
- MUTT-I: Natamycin 5% superior to voriconazole 1% for filamentous fungal keratitis (especially Fusarium); voriconazole superior for Aspergillus
- MUTT-II: Oral voriconazole showed no significant benefit over placebo when added to topical antifungal treatment
12.3 PACK-CXL (Photoactivated Chromophore for infectious Keratitis - Corneal Collagen Cross-Linking)
- Riboflavin + UV-A cross-linking as adjunctive or primary treatment for resistant infections
- Evidence of microbicidal effect in early bacterial keratitis
- Referenced in Kanski's 10th edition as a treatment option for resistant infections/corneal melting
- SCUT II is now testing this in a rigorous RCT
12.4 Rose Bengal Photodynamic Therapy (PDT) - 2026 RCT
- International, double-masked RCT of 330 patients; rose bengal PDT + topical antimicrobials vs. sham
- Result: No overall benefit on BSCVA at 6 months. Significant interaction by organism: RB PDT improved BSCVA in Fusarium infections but worsened it in Aspergillus infections. Scar size was smaller at 3 weeks in the PDT group but not at 3 or 6 months.
- Conclusion: RB PDT not recommended as standard adjuvant; further work with alternative photosensitizers needed
12.5 AI for Infectious Keratitis Diagnosis
- AI models show good accuracy for classifying infectious keratitis types on slit-lamp photography
- Potential for low-resource settings to guide empirical therapy before lab results
12.6 Confocal Microscopy for Acanthamoeba & Fungal Keratitis
- In vivo confocal microscopy (IVCM) shows high specificity for both Acanthamoeba and fungal keratitis
- Sensitivity for Acanthamoeba ~90%, specificity ~95% in experienced hands
- Increasingly recommended as first-line non-invasive diagnostic tool
12.7 Amniotic Membrane Graft (AMG) for Persistent Ulcers
- AMG associated with improved uncorrected VA and reduced neovascularisation in persistent post-infective epithelial defects
- No improvement in epithelial healing time or corneal opacity vs. controls
- More large RCTs needed
12.8 Hypochlorous Acid (HOCI) for Fungal Ulcers
- 0.01% hypochlorous acid eye drops + conventional treatment vs. conventional treatment alone for fungal corneal ulcers
- Statistically significant improvements in epithelial healing time, infiltrate size reduction, and symptom scores in the HOCI group
- Emerging adjunct for fungal keratitis
12.9 Cenegermin (Recombinant Human NGF)
- Oxervate 0.002% (cenegermin) approved for neurotrophic keratopathy
- Addresses the neurotrophic component that prevents healing in post-herpetic and CN V palsy-related ulcers
- Promotes epithelial regeneration by restoring nerve growth factor signalling
13. DIFFERENTIAL DIAGNOSIS
| Condition | Key distinguishing feature |
|---|---|
| Corneal abrasion | No infiltrate; history of trauma; heals within 24-48h |
| Marginal keratitis (staphylococcal hypersensitivity) | Peripheral; clear zone between infiltrate and limbus; no epithelial defect initially |
| Episcleritis/scleritis | No corneal ulcer; sectoral/diffuse scleral inflammation |
| Contact lens-related CLARE | No infiltrate; resolves with lens removal |
| Mooren's ulcer | Peripheral; sterile; progressive; overhanging edge; idiopathic autoimmune |
| Recurrent erosion syndrome | History of trauma; morning onset; no infiltrate |
| Interstitial keratitis | Stromal vascularisation; associated with syphilis/Cogan's; no true ulcer |
| Pterygium | Grows from limbus; no ulceration |
14. KEY CLINICAL PEARLS
- Never use topical steroids in fungal keratitis - promotes fungal growth and masks clinical progression
- Never patch a contact lens-related red eye - risk of explosive Pseudomonas proliferation
- HSV + inadvertent steroids = geographic amoeboid ulcer enlargement
- Severe pain disproportionate to signs = think Acanthamoeba
- Satellite lesions + feathery margins = think fungi (but not pathognomonic)
- Radial perineuritis = Acanthamoeba (pathognomonic)
- Post-vegetation injury = empirical antifungal, not antibacterial
- Descemetocele = surgical emergency; consider glue, patch graft, or PKP
- Ciprofloxacin precipitates (white deposit at ulcer base) = do NOT mistake for treatment failure
- Culture media for Acanthamoeba = non-nutrient agar seeded with E. coli (the amoeba consumes the bacteria)
Search for recent clinical practice guidelines on corneal ulcer management from ophthalmology societies
"corneal ulcer" OR "infectious keratitis" AND "guidelines"
corneal ulcer infectious keratitis clinical practice guidelines 2024 2025 ophthalmology society AAO NICE
corneal ulcer management guidelines diagnosis treatment recommendations
AAO preferred practice pattern infectious keratitis 2024 OR 2025 corneal ulcer guidelines update
corneal ulcer bacterial keratitis diagnosis treatment recommendations culture indications antibiotics
"bacterial keratitis" AND "preferred practice pattern"
"bacterial keratitis" AND "practice pattern" AND keratitis
Royal College Ophthalmologists RCOphth microbial keratitis guidelines 2024 2025 site:rcophth.ac.uk OR British Ophthalmological Society
📋 Recent Clinical Practice Guidelines on Corneal Ulcer Management
1. OVERVIEW OF CURRENT GUIDELINE LANDSCAPE
| Organisation | Document | Year |
|---|---|---|
| American Academy of Ophthalmology (AAO) | Bacterial Keratitis Preferred Practice Pattern® (Rhee MK et al.) | Feb 2024 |
| AAO | Cornea/External Disease Summary Benchmarks | December 2024 |
| Bascom Palmer Eye Institute (BPEI) | Infectious Keratitis Management: 10-Year Update (Pasricha et al., J Clin Med) | August 2025 |
| Indian Journal of Ophthalmology | Preferred Practice Guidelines on Infectious Keratitis in Ocular Surface Diseases (Bari A et al.) | April 2025 (PMID 40146138) |
| Royal College of Ophthalmologists (RCOphth) | Emergency Eye Care Commissioning Guidance (Microbial Keratitis section) | 2021, in force |
| Review of Ophthalmology | Infectious Keratitis: Guidelines for Diagnosis and Treatment (Aguwa et al.) | September 2025 |
2. AAO PREFERRED PRACTICE PATTERN® - BACTERIAL KERATITIS (2024)
2.1 When to Culture (AAO PPP 2024 Recommendations)
- Infiltrate >2 mm, central, or with stromal depth
- Significant stromal involvement or melting
- ≥1+ cells in the anterior chamber
- History of corneal surgery (LASIK, keratoplasty)
- Atypical clinical features suggestive of fungal, amoebic, or mycobacterial keratitis
- Multiple corneal infiltrates
- Unresponsive to initial broad-spectrum antibiotic therapy
Note: In mild, peripheral infiltrates without AC reaction (e.g., classic contact lens-related marginal infiltrate), empirical treatment without culture is acceptable.
- Corneal scrapings should be inoculated directly onto culture media at the slit lamp to maximise yield
- If direct inoculation is not feasible, use transport media and promptly incubate
- Contact lens, case, and solution should also be sent for culture in contact lens-related cases
2.2 Antibiotic Therapy - AAO PPP 2024 Recommendations
| Organism (or Unknown) | Topical Antibiotic | Concentration | Subconjunctival Dose |
|---|---|---|---|
| None/multiple types (empirical) | Fortified cefazolin | 50 mg/mL | 100 mg in 0.5 mL |
| Fortified tobramycin | 9-14 mg/mL | 20 mg in 0.5 mL | |
| OR fluoroquinolones | 3-6 mg/mL | Not available | |
| Gram-positive cocci | Cefazolin | 50 mg/mL | 100 mg in 0.5 mL |
| Vancomycin | 25-50 mg/mL | 25 mg in 0.5 mL | |
| Moxifloxacin/gatifloxacin/levofloxacin/besifloxacin | 5-6 mg/mL | Not available | |
| Gram-negative rods | Tobramycin | 9-14 mg/mL | 20 mg in 0.5 mL |
| Ceftazidime | 50 mg/mL | 100 mg in 0.5 mL | |
| Ciprofloxacin/ofloxacin/moxifloxacin/gatifloxacin | standard concentrations | Not available |
- For severe ulcers: loading dose every 5-15 minutes for first hour, then hourly for first 24-48 hours, tapering as response occurs
- Modify regimen if no improvement or stabilisation within 48 hours
- Hospitalization warranted for severe or vision-threatening cases, poor compliance, or inability to self-administer drops
2.3 Corticosteroid Use - AAO PPP 2024
- Reduce or eliminate topical steroids in any patient already using them at presentation until infection is controlled
- When the infiltrate compromises the visual axis, consider adding topical steroid after at least 2-3 days of progressive improvement on antibiotics, typically after pathogen identification
- Re-examine within 1-2 days after initiating topical steroid; monitor IOP
- Based on the SCUT trial evidence: no consistent overall visual benefit; benefit possible in severe central ulcers (the PPP acknowledges this ongoing uncertainty)
2.4 Patient Education (AAO PPP 2024)
- Warn patients with risk factors (contact lens wearers especially) of signs/symptoms requiring urgent review
- Discuss potential for permanent visual loss and need for visual rehabilitation
- Educate contact lens wearers about overnight wear risk and lens hygiene
- Refer patients with significant visual impairment for low vision rehabilitation
3. BPEI 10-YEAR UPDATE (PASRICHA ET AL., J CLIN MED 2025) - INSTITUTIONAL ALGORITHM
3.1 Key Culture Data Findings (BPEI, 2011-2021)
- Only 38.7% of cultures yielded a positive organism - highlights the difficulty of microbiological confirmation
- Bacteria accounted for 83.4% of positives
- Top Gram-negative: Pseudomonas aeruginosa; top Gram-positive: Staphylococcus aureus
3.2 BPEI Algorithm - New IK Patient
- Corneal cultures recommended for ALL cases of infectious keratitis, regardless of disease stage (more aggressive than AAO's selective culture criteria)
- High-risk features warranting additional measures:
- Contact lens wear → send lens, case, and solution for culture (mince lens on chocolate agar)
- Scleral involvement → systemic uveitis workup (TB, syphilis, Lyme)
- Neurotrophic keratopathy and corneal thinning → specialist involvement
- Empirical first-line: Fortified vancomycin + tobramycin (based on local sensitivity data supporting broad Gram+/- coverage)
- Note: BPEI favours fortified vancomycin over cephalosporins given increasing resistance
3.3 BPEI Algorithm - Referred/Clinically Worsening Patient
- Drug holiday (washout) 24-72 hours with no antimicrobials (if no severe melting or impending perforation) to maximise culture yield
- Confocal microscopy recommended to identify atypical organisms (fungus, Acanthamoeba)
- If organism identified but no clinical improvement → check sensitivities for resistance + assess compliance
- If worsening without significant thinning → corneal biopsy + PCR/metagenomic deep sequencing (MDS)
- Technique: 3 mm dermatological trephine + crescent blade; sample sent for both microbiology (chocolate agar) and pathology
- If corneal thinning/impending perforation → surgical intervention
3.4 Advanced Diagnostics Endorsed by BPEI
- Metagenomic Deep Sequencing (MDS) - emerging gold standard for pathogen identification when culture-negative; identifies exact species + resistance genes without prior organism hypothesis
- In vivo confocal microscopy - high sensitivity/specificity but limited by cost, availability, and user expertise
- PCR - useful for HSV, VZV, Acanthamoeba in culture-negative cases
4. PROCEDURAL TREATMENT - GUIDELINE POSITIONS ON PACK-CXL AND RB-PDAT (2025)
PACK-CXL (Photoactivated Chromophore CXL)
- May benefit patients with corneal melting secondary to infectious keratitis
- The SCUT II trial (RCT, ongoing, Prajna VN et al., PMID 39208371) is evaluating riboflavin CXL + difluprednate in bacterial ulcers - results awaited
- Current status: adjunctive, not first-line; used selectively for resistant/melting cases
- Kanski 10th edition endorses its use in resistant infections
Rose Bengal Photodynamic Antimicrobial Therapy (RB-PDAT)
- Not currently recommended as standard adjuvant based on the 2026 RCT (Prajna NV et al., PMID 40907580)
- The trial showed no overall benefit; organism-specific differences (benefit in Fusarium, harm in Aspergillus)
- BPEI states RB-PDAT "may benefit fungal IK patients" pending further clarification
5. INFECTIOUS KERATITIS IN OCULAR SURFACE DISEASE - PREFERRED PRACTICE GUIDELINES (INDIA, 2025)
- Lower threshold for inpatient admission in OSD-complicated keratitis
- Fluorescein staining with cobalt blue filter to document all epithelial defects
- Preservative-free monotherapy drops in mild-to-moderate ulcers to reduce epitheliotoxicity
- Anterior segment OCT for quantifying corneal thinning and infiltrate depth (not routine slit-lamp alone)
- Early tapering of epitheliotoxic drugs + judicious lubricant and steroid addition
- Lower threshold for procedures to enhance healing: AMG, electrolysis of trichiasis, punctal occlusion for severe dry eye
- Higher threshold for therapeutic keratoplasty in OSD - postoperative healing is markedly compromised
- Closer follow-up mandatory - healing is slower, reinfection risk is higher
- For corneal opacity in OSD: ocular surface stabilisation first before any keratoplasty
6. RCOphth EMERGENCY EYE CARE GUIDANCE (UK)
- Patients with suspected CL-related microbial keratitis should be examined on a slit lamp as soon as possible and within 24 hours of symptom onset
- Once clinical diagnosis made, corneal scrape for culture should be performed before commencing antimicrobials
- Referral pathway: same-day urgent ophthalmic assessment, not next-day routine clinic
- The RCOphth and AAO PPP are aligned on corneal scraping technique: sterile Kimura spatula or blade, samples from both ulcer edge and base
7. ACANTHAMOEBA KERATITIS - ADVANCES IN GUIDELINES (CMR 2026)
- No standardized treatment guidelines currently exist for AK - management remains largely empirical and institution-dependent
- Combination therapy (topical biguanide + aromatic diamidine) remains the historical standard
- Emerging evidence supports PHMB monotherapy at higher concentrations (0.04-0.06%) with outcomes comparable to combination treatment, reducing complexity and patient burden
- Adjunctive therapies: Topical azoles, miltefosine, and delayed steroids (for inflammatory scleritis) may benefit refractory cases
- Therapeutic keratoplasty often required in advanced/non-responsive disease
- Pipeline therapies: Antimicrobial peptides, synthetic polymers, bioactive natural compounds, and UV-C therapy show early promise
8. THERAPEUTIC KERATOPLASTY - GUIDELINE POSITION (SYSTEMATIC REVIEW 2026)
- Overall infection control: 69-100%; globe preservation in 85-100% of cases
- Bacterial keratitis has higher cure rates and graft clarity than fungal or Acanthamoeba
- Larger grafts (>8 mm) associated with increased rejection and postoperative complications
- DALK offers higher graft survival and lower immunologic risk when Descemet's is spared - preferred over PKP when possible
- Early surgical intervention improves anatomical outcomes in severe fungal keratitis
- Visual outcomes are generally limited despite anatomical success - informed consent essential
9. BANDAGE CONTACT LENS vs AMNIOTIC MEMBRANE - UPDATED EVIDENCE (2025)
- Both BCL and AMG support corneal wound healing but through different mechanisms
- BCL is cost-effective, widely available, reversible; risk of superinfection requires close monitoring
- AMG provides anti-inflammatory, anti-scarring, and epitheliotrophic properties; beneficial in non-healing ulcers
- Current evidence does not definitively favour one over the other - patient and ulcer characteristics should guide choice
- AMG preferred for persistent defects post-infection, significant inflammation, or limbal stem cell involvement
10. SUMMARY OF KEY GUIDELINE CHANGES AND POSITIONS (2024-2026)
| Topic | Current Guideline Position |
|---|---|
| When to culture | AAO PPP 2024: infiltrate >2 mm, central, stromal, AC reaction, post-surgical, atypical, non-responsive. BPEI: culture ALL cases |
| Empirical antibiotic | Monotherapy fluoroquinolone (mild); fortified vancomycin + tobramycin or cephalosporin + aminoglycoside (severe) |
| Steroids in bacterial keratitis | After 48-72h of documented improvement; for central/severe ulcers only; no blanket recommendation for routine use |
| PACK-CXL | Adjunctive in melting/resistant cases; awaiting SCUT II RCT results |
| RB-PDAT | Not recommended as standard adjuvant (negative 2026 RCT - PMID 40907580) |
| Acanthamoeba | PHMB monotherapy (higher concentration) emerging as simpler alternative to combination; no formal standardised guidelines yet |
| Fungal keratitis | Natamycin first-line for filamentous; voriconazole for Aspergillus; no benefit from adding oral voriconazole (MUTT-II) |
| Therapeutic keratoplasty | Globe preservation in 85-100%; DALK preferred over PKP when Descemet's spared; early surgery for severe fungal |
| Metagenomic sequencing | Endorsed by BPEI as emerging tool for culture-negative/refractory cases |
| AI-assisted diagnosis | Promising for resource-limited settings; not yet standard of care |
| Neurotrophic keratopathy | Cenegermin (Oxervate) established; insulin eye drops under investigation (emerging, 2025 review) |
give me the note of bacterial corneal ulcer from basic to advanced level from the standard textbooks and add images to it, any clinical trials and recent advances. write it in chat and write about the viva questions that can be asked here
"bacterial keratitis" AND treatment
🦠 Bacterial Corneal Ulcer (Bacterial Keratitis)
Complete Clinical Notes - Basic to Advanced Level
1. DEFINITION
Kanski's 10th: "Bacterial keratitis usually develops only when ocular defences have been compromised. However, some bacteria... are able to penetrate a healthy corneal epithelium."
2. EPIDEMIOLOGY
- Bacterial keratitis accounts for ~44% of all infectious keratitis globally (range 29% in Africa to 61% in Oceania)
- Of ~25,000 bacterial isolates: 72% were Gram-positive
- Leading organisms globally:
- Pseudomonas aeruginosa: 17% (dominant in contact lens-related disease)
- Staphylococcus epidermidis: 15%
- Streptococcus pneumoniae: 13%
- Staphylococcus aureus: 10%
- Leading risk factors: trauma (~44%) and contact lens wear (~23%)
- ~20% of S. aureus isolates were MRSA - a growing concern
- Fluoroquinolone susceptibility for S. aureus was only ~77% - indicating rising resistance
3. NORMAL CORNEAL DEFENCE MECHANISMS
| Defence Layer | Mechanism |
|---|---|
| Intact epithelium | Physical barrier; tight junctions; rapid regeneration |
| Tear film | Lysozyme, lactoferrin, IgA, beta-lysin, defensins |
| Blinking mechanism | Mechanical clearance; even tear distribution |
| Mucin layer | Prevents bacterial adhesion |
| Limbal vascularity | Delivers neutrophils and immunoglobulins |
| Normal microbiome | Competitive inhibition of pathogens |
| Reflex lacrimation | Dilutes and washes out microorganisms |
- Neisseria gonorrhoeae
- Neisseria meningitidis
- Corynebacterium diphtheriae
- Haemophilus influenzae
4. PATHOGENS - DETAILED MICROBIOLOGY
4.1 Gram-Positive Organisms
- Gram-positive coagulase-positive cocci in clusters
- Commensal of nares, skin, conjunctiva
- Produces coagulase, haemolysin, exotoxins, and protein A (antiphagocytic)
- Produces leukocidin which destroys neutrophils
- Presents as focal, well-defined yellow-white infiltrate
- MRSA increasingly community-acquired; vancomycin is definitive treatment
- Blepharitis and chronic lid disease are important predisposing factors
- Gram-positive lancet-shaped diplococci
- Commensal of upper respiratory tract
- Often aggressive; associated with hypopyon
- Classic cause of hypopyon ulcer historically
- Produces pneumolysin, neuraminidase, capsule (antiphagocytic)
- Gram-positive chains
- Throat and vaginal commensal
- Often aggressive keratitis
- Coagulase-negative; commensal of skin/conjunctiva
- Common post-surgical (LASIK, cataract surgery) pathogen
- Lower virulence but important in immunocompromised
4.2 Gram-Negative Organisms
- Gram-negative rod (bacillus); ubiquitous environmental organism
- GI tract commensal; ubiquitous in moist environments
- Produces exotoxin A, proteases (elastase, alkaline protease), pyocyanin
- Proteases cause rapid corneal melting (keratolysis) - can perforate within 24-48 hours
- Responsible for >60% of contact lens-related bacterial keratitis (Kanski's)
- Classic appearance: aggressive, rapidly expanding dense infiltrate with mucopurulent discharge; ring infiltrate possible
- May form biofilm on contact lenses
- Large Gram-negative diplobacillus
- Associated with debilitated patients: alcoholism, malnutrition, chronic illness
- Typically indolent, inferior corneal location
- Responds well to beta-lactams
- Small Gram-negative coccobacillus
- Usually occurs in children with conjunctivitis
- Can penetrate intact epithelium
- Red pigment-producing Gram-negative rod
- Associated with contact lens wear and immunosuppression
4.3 Other Organisms
- Gram-positive filamentous, weakly acid-fast
- Post-refractive surgery (LASIK interface keratitis)
- Characteristic cracked windshield pattern at interface
- Modified Ziehl-Neelsen staining; treat with sulfonamides + amikacin
- Post-refractive surgery; slow-growing
- Acid-fast; Löwenstein-Jensen medium; treat with amikacin + clarithromycin
5. RISK FACTORS
High-risk (most important):
- Contact lens wear - especially extended wear, overnight use, soft lenses, poor hygiene, tap water use
- Ocular trauma - including vegetative matter (though this raises fungal concern too)
- Ocular surface disease - dry eye, blepharitis, meibomian gland dysfunction, trichiasis
- Previous ocular surgery - LASIK, keratoplasty, cataract surgery
- Topical steroid use - suppresses local immunity, promotes organism replication
Moderate-risk:
- Corneal anaesthesia (diabetic neuropathy, herpetic, CN V lesion)
- Systemic immunosuppression (HIV, diabetes, chemotherapy, systemic steroids)
- Neurotrophic or exposure keratopathy
- Bullous keratopathy
- Ocular cicatricial pemphigoid, Stevens-Johnson syndrome
Demographic/environmental:
- Agricultural/outdoor workers (trauma risk)
- Low-income/resource-limited settings (delayed care, malnutrition)
- Elderly (reduced immunity, tear production)
Kanski's 10th: "Contact lens wear, particularly if extended, is the most important risk factor. Corneal epithelial compromise secondary to hypoxia and minor trauma is thought to be important, as is bacterial adherence to the lens surface."
6. PATHOGENESIS
Epithelial breach
↓
Bacterial adhesion (via adhesins, fimbriae, surface proteins)
↓
Epithelial invasion and multiplication
↓
Stroma penetration → Keratocyte death → PMN recruitment
↓
Protease release (bacterial + host metalloproteinases)
↓
Collagen lysis → Stromal melting (keratolysis)
↓
Anterior chamber spillover → Sterile hypopyon (AC flare + cells)
↓
[If untreated] → Descemetocele → Perforation → Endophthalmitis
- Pseudomonas: Elastase + alkaline protease cleave collagen, IgA, and complement; exotoxin A inhibits protein synthesis; biofilm formation resists antibiotics
- S. aureus: Protein A binds IgG; leukocidin destroys WBCs; TSST-1 superantigen
- Streptococcus: Capsule inhibits phagocytosis; streptolysin, pneumolysin cause cell lysis
7. CLINICAL FEATURES
7.1 Symptoms (in order of frequency)
- Ocular pain - moderate to severe; may be acute onset
- Photophobia - due to ciliary spasm from associated iritis
- Lacrimation (watering)
- Mucopurulent discharge - more prominent than in viral or fungal
- Blurred vision / reduced visual acuity - especially if central
- Red eye (conjunctival injection + ciliary flush)
- Contact lens intolerance - sudden inability to wear lenses comfortably
- Lid swelling / periorbital oedema
7.2 Signs - Critical (Slit Lamp)
"Focal white opacity (infiltrate) in the corneal stroma associated with an epithelial defect and underlying stromal thinning/tissue loss."
Key slit lamp tip: "An examiner using a slit beam cannot see clearly through an infiltrate or ulcer to the iris, whereas stromal edema or mild anterior stromal scars are more transparent." - Wills Eye Manual
- Epithelial defect - stains bright green with fluorescein under cobalt blue light
- Stromal infiltrate - dense, white-grey, opaque; WBC and proteinaceous infiltration
- Surrounding oedema - hazy stroma surrounding infiltrate
- Mucopurulent discharge on lids and lashes
- Conjunctival injection - mixed ciliary (circumcorneal) + conjunctival
- Endothelial fibrin/cell deposition - keratic precipitates under infiltrate
- Anterior chamber reaction - flare and cells
- Hypopyon - horizontal fluid level of sterile pus; does NOT equal endophthalmitis
- Descemet's folds - indicate significant stromal oedema
- Posterior synechiae - in severe prolonged cases
- Raised IOP - in severe cases with angle involvement
- Lid oedema, upper lid ptosis - reactive
7.3 Organism-Specific Clinical Patterns
| Organism | Clinical Clue |
|---|---|
| Pseudomonas aeruginosa | Rapidly progressive; liquefactive necrosis; blue-green tinge (pyocyanin); ring infiltrate; severe mucopurulent discharge; contact lens history |
| Staphylococcus aureus | Focal, well-defined yellow-white infiltrate; blepharitis association; may progress slowly |
| Streptococcus pneumoniae | Aggressive; classically associated with large hypopyon ("hypopyon ulcer" of old texts); serpiginous edge |
| Moraxella | Inferior cornea; indolent; debilitated patient; oval ulcer |
| Serratia | Red pigment on culture; contact lens wearer |
| Nocardia | Post-LASIK; cracked windshield/branching infiltrate pattern |
8. KEY CLINICAL IMAGES
Bacterial keratitis - slit-lamp view:
Corneal scraping technique:

Bacterial growth on blood agar:

Large bacterial ulcer - fluorescein:
9. INVESTIGATIONS
9.1 When to Culture (AAO PPP 2024)
- Infiltrate >2 mm diameter
- Central location or involves visual axis
- Stromal depth involvement (middle-deep)
- ≥1+ cells in anterior chamber
- History of corneal surgery
- Appearance atypical (suggests fungal, Acanthamoeba, mycobacteria)
- Multiple infiltrates
- Chronic or unresponsive to initial therapy
9.2 Corneal Scraping Technique (Step-by-Step from Kanski's)
- Instil preservative-free topical anaesthetic (proxymetacaine 0.5%) - preservatives may reduce bacterial viability
- At slit lamp: use a No. 11 Bard-Parker scalpel blade, bent-tip hypodermic needle (20-21G), or Kimura spatula
- Remove loose mucus and necrotic tissue from ulcer surface first
- Scrape margins AND base of the ulcer (not just the surface)
- Thin smear on 1-2 glass slides for Gram stain and microscopy - air dry
- Re-scrape for each culture medium (flame sterilise between scrapes or use fresh blade)
- Inoculate directly onto media at slit lamp to maximise yield
9.3 Culture Media (Kanski's Table 7.2)
| Medium | Organisms Targeted |
|---|---|
| Blood agar | Most bacteria and fungi (not Neisseria, H. influenzae, Moraxella) |
| Chocolate agar | Fastidious bacteria: H. influenzae, Neisseria, Moraxella |
| Sabouraud dextrose agar | Fungi |
| Non-nutrient agar + E. coli | Acanthamoeba |
| Brain-heart infusion (BHI) | Difficult-to-culture organisms; streptococci; meningococci; yeasts |
| Cooked meat broth | Anaerobes; fastidious bacteria |
| Löwenstein-Jensen | Mycobacteria, Nocardia |
9.4 Staining Techniques
| Stain | Use |
|---|---|
| Gram stain | Primary stain; differentiates Gram+/- bacteria; ~60% sensitivity |
| Giemsa | Bacteria, fungi, multinucleated giant cells (HSV) |
| Ziehl-Neelsen (ZN) | Mycobacteria |
| Modified ZN (Kinyoun) | Nocardia (weakly acid-fast) |
| KOH prep | Rapid fungal diagnosis; highly sensitive |
| Calcofluor white | Fungi + Acanthamoeba (fluorescent stain) |
| PAS stain | Fungi, Acanthamoeba cysts |
| Methenamine silver | Fungi |
9.5 Advanced Diagnostic Tools
- PCR - for resistant/culture-negative cases; rapid pathogen identification + resistance genes
- Metagenomic Deep Sequencing (MDS) - endorsed by BPEI 2025; no prior organism hypothesis required; identifies all organisms + resistance; especially for culture-negative refractory cases
- In vivo Confocal Microscopy (IVCM) - non-invasive real-time imaging; high sensitivity for fungal/Acanthamoeba (can also visualise inflammatory infiltrates in bacterial keratitis but less organism-specific); limited by cost and expertise
- Anterior Segment OCT (AS-OCT) - quantifies infiltrate depth, corneal thinning; monitors treatment response; recommended in Indian PPG 2025
10. TREATMENT
10.1 General Principles
- All cultures before starting antibiotics
- Aggressive loading doses from the outset
- Never patch a patient with contact lens-related ulcer (worsens Pseudomonas infection explosively)
- Cycloplegia - cyclopentolate 1% or atropine 1% TID: prevents synechiae, reduces ciliary spasm pain
- Hospitalisation if: severe/vision-threatening, poor compliance, inability to self-administer, or pain is uncontrolled
- Review within 24-48 hours and modify if no improvement
10.2 Severity-Based Treatment Protocol (Wills Eye Manual)
Mild - Low Risk of Visual Loss
- Fluoroquinolone QID to q1h depending on severity
- Review in 24-48h
Borderline - Moderate Risk
- Fluoroquinolone (moxifloxacin, gatifloxacin, ciprofloxacin, besifloxacin, or levofloxacin) q1h around the clock
- Loading dose option: q5min × 5 doses, then q30min until midnight, then q1h
- Note (Wills Eye): "Moxifloxacin and besifloxacin have slightly better Gram-positive coverage. Gatifloxacin and ciprofloxacin have slightly better Pseudomonas and Serratia coverage."
Severe - Vision Threatening
- Fortified tobramycin 15 mg/mL OR gentamicin 15 mg/mL q1h, alternating with fortified cefazolin 50 mg/mL q1h
- = patient instils a drop every 30 minutes around the clock
- If Pseudomonas strongly suspected: fortified tobramycin q30min + fortified cefazolin q1h + consider ceftazidime q1h or fluoroquinolone q1h
- Vancomycin 25-50 mg/mL: reserved for MRSA, resistant organisms, penicillin/cephalosporin allergy
- Loading dose (Wills Eye): q5min × 5 doses, then q30-60min around the clock
10.3 AAO PPP 2024 Antibiotic Table (Full)
| Organism | Topical Agent | Concentration | Subconj Dose |
|---|---|---|---|
| Unknown / empirical | Fortified cefazolin | 50 mg/mL | 100 mg in 0.5 mL |
| Fortified tobramycin | 9-14 mg/mL | 20 mg in 0.5 mL | |
| OR fluoroquinolone | 3-6 mg/mL | N/A | |
| Gram-positive cocci | Cefazolin | 50 mg/mL | 100 mg in 0.5 mL |
| Vancomycin | 25-50 mg/mL | 25 mg in 0.5 mL | |
| Moxifloxacin/besifloxacin/levofloxacin | 5-6 mg/mL | N/A | |
| Gram-negative rods | Tobramycin | 9-14 mg/mL | 20 mg in 0.5 mL |
| Ceftazidime | 50 mg/mL | 100 mg in 0.5 mL | |
| Cipro/ofloxacin/moxifloxacin | Standard | N/A |
10.4 Preparation of Fortified Antibiotics (Kanski's Table 7.5)
| Antibiotic | Method | Concentration | Shelf-Life |
|---|---|---|---|
| Cefazolin 50 mg/mL | 500 mg parenteral + 2.5 mL sterile water + 7.5 mL preservative-free artificial tears | 50 mg/mL | 24h room temp; 4 days refrigerated |
| Gentamicin 15 mg/mL | 2 mL parenteral (40 mg/mL) + 5 mL commercial 0.3% gentamicin solution | 15 mg/mL | 14 days refrigerated |
10.5 Steroids in Bacterial Keratitis
- SCUT Trial (Steroids for Corneal Ulcers Trial): no significant improvement in VA at 3 months overall; trend toward benefit in severe central ulcers
- SCUT II Trial (Prajna VN et al., PMID 39208371, ongoing): testing difluprednate + PACK-CXL in bacterial keratitis
- Current AAO PPP 2024 guidance:
- Reduce/stop steroids if already using at presentation, until infection controlled
- May ADD steroids after 2-3 days of documented progressive improvement
- Preferably after pathogen identification
- Re-examine within 1-2 days of steroid initiation; monitor IOP
10.6 Systemic Antibiotics - When Indicated
| Indication | Drug |
|---|---|
| N. meningitidis | IM benzylpenicillin OR ceftriaxone/cefotaxime OR oral ciprofloxacin (life-saving prophylaxis) |
| N. gonorrhoeae | Ceftriaxone (3rd generation cephalosporin) + azithromycin |
| H. influenzae | Oral co-amoxiclav (amoxicillin + clavulanate) |
| Corneal thinning/impending perforation | Oral ciprofloxacin (antibacterial) + doxycycline 100 mg BD (anticollagenase effect - reduces stromal melting) |
| Scleral involvement | Oral or IV antibiotics |
10.7 Management of Treatment Failure (Kanski's)
- 24-48h no improvement → Review antibiotic regimen; contact microbiology lab for latest report
- No need to change therapy if favourable response even if cultures show resistant organism (high local tissue levels)
- 48h of continued failure → Consider 24h drug washout, then re-scrape with broader media and additional stains
- Consider non-bacterial pathogen (fungal, Acanthamoeba, viral)
- Cultures remain negative → Corneal biopsy for histology + culture
- Evidence of corneal melting/resistance → Consider PACK-CXL
- Medical failure → Surgical options
Kanski's: "Topical drug and preservative toxicity may cause a failure of corneal re-epithelialization, which can be confused with persistent infection."
10.8 Surgical Management
| Situation | Intervention |
|---|---|
| Small perforation (<1 mm), infection controlled | Bandage contact lens (BCL) |
| Small-moderate perforation (1-3 mm) | Cyanoacrylate tissue glue + BCL |
| Larger perforation / uncontrolled infection | Penetrating keratoplasty (PKP) or corneal patch graft |
| Medical failure, deep infection | PKP ("therapeutic keratoplasty") - "hot keratoplasty" has high rejection risk |
| Anterior stroma only, Descemet's spared | Deep anterior lamellar keratoplasty (DALK) - lower rejection risk |
| Persistent epithelial defect | Amniotic membrane graft (AMG), Gundersen flap, tarsorrhaphy |
- Infection control: 69-100%; globe preservation: 85-100%
- Bacterial keratitis has higher cure rates than fungal or Acanthamoeba
- DALK offers higher graft survival and lower rejection than PKP when Descemet's is spared
- Larger grafts (>8 mm) = increased rejection and complications
- Visual outcomes are generally limited
11. COMPLICATIONS (Severity Ladder)
- Corneal scarring - permanent if Bowman's layer breached; leukoma; irregular astigmatism
- Corneal vascularisation - complicates future transplantation
- Descemetocele - only Descemet's membrane remains; requires emergency intervention
- Corneal perforation - iris prolapse; flat anterior chamber; risk of endophthalmitis
- Hypopyon - usually sterile reactive; rarely indicates true intraocular infection
- Endophthalmitis - if perforation occurs or organism penetrates Descemet's
- Secondary glaucoma - inflammatory angle closure, synechiae
- Cataract - from sustained inflammation
- Phthisis bulbi - end-stage shrunken blind eye
12. MONITORING PARAMETERS
- Review daily initially during intensive phase
- Check VA, infiltrate size, epithelial defect size (measure and document with slit lamp)
- IOP - monitor especially if steroids added
- Watch for:
- Thinning / descemetocele formation
- Progression of hypopyon
- Signs of perforation (sudden pain relief, shallow AC, positive Seidel test)
- Drug toxicity (follicular conjunctivitis, punctate epitheliopathy)
13. RECENT CLINICAL TRIALS & ADVANCES
13.1 🔬 Cochrane Network Meta-Analysis - Best Topical Antibiotic (2025)
- Top 3 treatments by SUCRA ranking (time to healing):
- Vancomycin + ceftazidime (SUCRA 83.8) - fastest healing
- Moxifloxacin monotherapy (SUCRA 83.1) - nearly equal
- Cefazolin + tobramycin (SUCRA 71.3)
- All three showed ~6-7 days faster healing than ciprofloxacin
- Moxifloxacin emerged as the best fluoroquinolone option
- Certainty of evidence: moderate (moxifloxacin) to low (fortified combinations)
- Clinical implication: For monotherapy, moxifloxacin is preferred; for severe disease, vancomycin + ceftazidime or cefazolin + tobramycin
13.2 📊 Meta-Analysis: Fortified vs Fluoroquinolones (2024)
- 9 RCTs compared fortified antibiotics vs fluoroquinolones
- Cure rates equivalent (OR=0.99)
- Adverse events equivalent (OR=0.75, not significant)
- Time to cure shorter with fluoroquinolones (MD -0.96 days shorter)
- Conclusion: "It seems reasonable to use fluoroquinolones as the preferred treatment for bacterial keratitis" - simpler preparation, commercially available, fewer refrigeration/preparation issues
13.3 🌍 Global Burden Meta-Analysis (2026)
- ~20% of S. aureus are MRSA - mandates vancomycin for severe/resistant Gram-positive keratitis
- Fluoroquinolone susceptibility for S. aureus only ~77% - increasing resistance
- Gram-negative isolates: >90% susceptible to aminoglycosides and cephalosporins
- Gram-positive: >95% susceptibility to vancomycin
- Empirical therapy must target MRSA AND Pseudomonas simultaneously in high-risk settings
13.4 🔷 PACK-CXL for Infectious Keratitis (2025)
- PACK-CXL (photoactivated chromophore corneal cross-linking with riboflavin + UVA): has direct antimicrobial and anti-collagenolytic (anti-melting) effects
- Adjuvant PACK-CXL is NOT inferior to standard antibiotic therapy alone
- May be superior for faster epithelial healing in some cases (especially fungal, but bacterial data also exists)
- Limitations: no uniform protocol, heterogeneous results across studies
- Not yet standard of care; used for refractory/melting cases
- The SCUT II trial will provide higher-quality evidence specifically for bacterial keratitis
13.5 ⚠️ SCUT II Trial (Ongoing, 2024)
- International, randomized, double-masked, multicenter RCT
- Tests riboflavin CXL AND/OR topical difluprednate (potent steroid) as adjuncts to antibiotics in smear-positive bacterial ulcers
- 280 patients enrolled; India + USA
- Baseline data published 2024; outcome data awaited
- Important finding: ~10% of unilateral bacterial keratitis patients have a blind fellow eye (preexisting cataract/glaucoma in India) - at risk of bilateral blindness
- Results will define the role of CXL + steroids in bacterial keratitis evidence-based practice
13.6 🤖 AI for Bacterial Keratitis Diagnosis (2023)
- AI deep learning models applied to slit-lamp photography can classify infectious keratitis type (bacterial vs fungal vs viral) with reasonable accuracy
- Potential to assist diagnosis in resource-limited settings before microbiological results
- Not yet validated as standalone clinical tool; adjunct role only
13.7 🧬 Metagenomic Deep Sequencing (MDS)
- Endorsed by Bascom Palmer Eye Institute as the emerging gold standard for culture-negative/refractory keratitis
- Identifies all organisms from a corneal swab + antibiotic resistance genes without prior culture
- No organism hypothesis required - simultaneous pan-pathogen detection
- Currently limited to specialist centres; rapidly becoming more accessible
14. DIFFERENTIAL DIAGNOSIS OF BACTERIAL KERATITIS
| Condition | Key Distinguishing Feature |
|---|---|
| Fungal keratitis | Trauma (vegetable matter); satellite lesions; feathery borders; gradual onset; less discharge |
| Acanthamoeba keratitis | Severe pain >> signs; radial perineuritis; contact lens + tap water; pseudo-dendrites early |
| HSV epithelial keratitis | Dendritic ulcer with terminal buds; recurrent history; reduced corneal sensation |
| Marginal keratitis | Peripheral; clear gap from limbus; staphylococcal hypersensitivity; minimal discharge |
| Contact lens infiltrate (CLPU) | Small peripheral infiltrate; mild/no discharge; minimal AC reaction; resolves with lens removal |
| Corneal abrasion | History of injury; no infiltrate; heals in 24-48h |
| Sterile/autoimmune ulcer (Mooren's) | Progressive peripheral; overhanging edge; no organisms; idiopathic autoimmune |
| Interstitial keratitis | Deep stromal vascularisation; syphilis/Cogan's; no true epithelial ulcer |
15. PREVENTION
- Educate contact lens wearers: no overnight wear, no tap water, no swimming with lenses
- Prefer daily disposable lenses over extended-wear
- Proper lens hygiene protocol (hydrogen peroxide-based systems are preferred over multipurpose solutions for high-risk users)
- Protective eyewear for agricultural/industrial work
- Treat predisposing ocular surface disease (blepharitis, dry eye, entropion)
- Systemic management of diabetes and immunosuppression
- Lid hygiene for chronic blepharitis patients
- Prophylactic antibiotics post-ocular surgery if risk factors present
🎓 VIVA QUESTIONS - BACTERIAL KERATITIS
🔵 BASIC LEVEL
A: Bacterial infection of the corneal stroma, occurring when bacteria invade the stroma through a breach in the epithelial barrier. It requires breakdown of the normal defence mechanisms (epithelial integrity, tear film, blinking) to establish infection. Some organisms (N. gonorrhoeae, N. meningitidis, C. diphtheriae, H. influenzae) can penetrate an intact epithelium.
A: Vary by geography and risk factors. Globally (Singh et al. meta-analysis 2026): Pseudomonas aeruginosa (~17%), S. epidermidis (~15%), S. pneumoniae (~13%), S. aureus (~10%). In contact lens wearers, Pseudomonas aeruginosa dominates (>60%). Gram-positives account for ~72% overall.
A: Contact lens wear, especially extended/overnight use with soft lenses. The mechanism involves: corneal hypoxia from lens-induced epithelial compromise, bacterial adherence to the lens surface, and physical trauma during insertion/removal.
A: Pain (moderate-severe, acute onset), photophobia, lacrimation, mucopurulent discharge, blurred vision, red eye, and acute contact lens intolerance.
A: A focal white stromal infiltrate associated with an epithelial defect - the infiltrate is completely opaque and you cannot see the iris through it (unlike stromal oedema or scar which is more translucent). This is accompanied by surrounding oedema, AC reaction, and often hypopyon in severe cases.
A: Hypopyon is a horizontal sterile fluid level of white blood cells in the anterior chamber. In bacterial keratitis, it represents a sterile inflammatory reaction (not true endophthalmitis) - WBCs and protein leak from the inflamed iris/ciliary body into the AC. Aqueous/vitreous tap is NOT needed unless intraocular surgery, perforating trauma, or sepsis coexists (AAO PPP 2024). It signals severe infection but NOT necessarily intraocular involvement.
A: Blood agar → most bacteria; Chocolate agar → fastidious organisms (H. influenzae, Neisseria, Moraxella); Sabouraud's → fungi; Non-nutrient agar + E. coli → Acanthamoeba; Löwenstein-Jensen → Mycobacteria/Nocardia; Brain-heart infusion → difficult organisms, anaerobes.
🟡 INTERMEDIATE LEVEL
A: For small (<2 mm), peripheral, mild infiltrates in straightforward contact lens wearers without AC reaction or significant symptoms - empirical treatment may be started. All other cases meeting AAO PPP criteria (central, stromal, >2 mm, AC reaction, post-surgical, atypical, unresponsive) should be cultured.
A: Four organisms: Neisseria gonorrhoeae, Neisseria meningitidis, Corynebacterium diphtheriae, and Haemophilus influenzae. They are typically associated with severe conjunctivitis. N. gonorrhoeae in particular is important to recognise as it can cause rapid corneal perforation and has systemic implications.
A: (i) Instil preservative-free topical anaesthetic (proxymetacaine 0.5%). (ii) At slit lamp, using sterile No.11 blade/Kimura spatula/bent 21G needle. (iii) Remove loose mucus and necrotic tissue first. (iv) Scrape margins AND base of ulcer. (v) Thin smear on glass slides for Gram stain. (vi) Re-scrape for each culture medium, inoculating directly onto plates at slit lamp. (vii) Do NOT break the gel surface of agar.
A: Fortified tobramycin 15 mg/mL alternating with fortified cefazolin 50 mg/mL every 30 minutes (i.e., each every 1 hour, alternating = one drop every 30 minutes). Loading dose: q5min × 5 doses, then q30min. Add cyclopentolate 1% for cycloplegia. If MRSA risk, use vancomycin instead of/in addition to cefazolin.
A: Patching creates a warm, anaerobic, nutrient-rich environment ideal for bacterial proliferation - especially Pseudomonas aeruginosa, which can cause explosive growth and rapid corneal liquefaction and perforation under a patch within hours.
A: (i) Prevents formation of posterior synechiae between iris and lens. (ii) Relieves ciliary spasm, which is the main source of pain and photophobia. (iii) Stabilises the blood-aqueous barrier. Options: cyclopentolate 1%, homatropine 2%, or atropine 1% TID.
A: Moxifloxacin and besifloxacin have better Gram-positive coverage (including MRSA activity for moxifloxacin). Ciprofloxacin and gatifloxacin have better Gram-negative/Pseudomonas coverage. For empirical therapy in a contact lens wearer (suspect Pseudomonas), ciprofloxacin or gatifloxacin may be preferred; for a post-surgical case (suspect Gram-positive), moxifloxacin is preferred.
A: They are ciprofloxacin calcium precipitates deposited at the epithelial defect site. They do NOT indicate treatment failure or worsening infection. Treatment should be continued. This is a known and benign side effect of ciprofloxacin eye drops.
A: Systemic antibiotics are not routine. Indications: (1) N. meningitidis - systemic prophylaxis (benzylpenicillin/ceftriaxone) is life-saving; (2) N. gonorrhoeae - ceftriaxone systemically; (3) H. influenzae - co-amoxiclav; (4) Corneal thinning/threatened perforation - oral doxycycline 100 mg BD for its anticollagenase effect (inhibits matrix metalloproteinases, reduces stromal melting); (5) Scleral involvement.
🔴 ADVANCED LEVEL
A: Dual mechanism - bacterial and host: (1) Bacterial proteases (especially Pseudomonas elastase and alkaline protease) directly cleave collagen fibrils. (2) Host matrix metalloproteinases (MMPs) - particularly MMP-2 and MMP-9 - released by inflammatory cells and keratocytes degrade corneal stroma. The net result is liquefactive stromal necrosis. This is why doxycycline (tetracycline class) is used as adjunctive treatment - it inhibits MMPs regardless of antibiotic effect on bacteria.
A: The Steroids for Corneal Ulcers Trial (SCUT) was an international, randomised, double-masked, placebo-controlled trial that evaluated topical prednisolone phosphate 1% (started after 48h of antibiotics) vs placebo in bacterial keratitis. Main finding: no significant difference in best spectacle-corrected VA at 3 months overall. However, patients with severe disease (count-fingers VA or large ulcers involving the central 4 mm of cornea) showed a trend toward benefit. This established that steroids are not for routine use but may benefit the most severe cases.
A: Photoactivated Chromophore for infectious Keratitis - Corneal Collagen Cross-Linking. Uses riboflavin (photosensitiser) + UVA light to: (a) cross-link corneal collagen (increases stromal resistance to protease digestion/melting), and (b) directly kill bacteria via reactive oxygen species generation. Current evidence (Farhadi et al. umbrella review, BMC Ophthalmol 2025): not inferior to standard antibiotic therapy; potentially faster healing in some cases; no uniform protocol; heterogeneous results. Current role: adjunctive treatment for resistant infections and corneal melting. SCUT II trial will provide more definitive data.
A: The NMA (Song A et al., Cochrane 2025, 23 RCTs, 2,692 patients) ranked: (1) Vancomycin + ceftazidime SUCRA 83.8 - fastest healing, excellent broad spectrum; (2) Moxifloxacin monotherapy SUCRA 83.1 - nearly as effective, commercially available, simpler. Both showed ~6-7 day faster healing than ciprofloxacin (moderate certainty). Clinical implications: (i) Moxifloxacin should be preferred over ciprofloxacin for mild-moderate disease; (ii) For severe disease, vancomycin + ceftazidime is evidence-based; (iii) The older evidence equating ciprofloxacin and fortified antibiotics needs revision; (iv) Fluoroquinolone resistance (~23% for S. aureus) supports more aggressive empirical coverage.
A: The 2026 meta-analysis (Singh et al.) found ~20% of S. aureus isolates were MRSA. MRSA is resistant to all beta-lactams (penicillins AND cephalosporins). This means: (1) Standard fortified cefazolin will fail for MRSA cases; (2) Vancomycin 25-50 mg/mL topically is the treatment of choice for MRSA; (3) Moxifloxacin has some MRSA activity but not sufficient alone in severe MRSA keratitis; (4) Community-acquired MRSA is increasing - always consider in severe unresponsive S. aureus infections.
A: Both present with a peripheral corneal infiltrate. Key differences:
| Feature | Bacterial Keratitis | Marginal Keratitis |
|---|---|---|
| Aetiology | Active infection (S. aureus, Pseudomonas etc.) | Hypersensitivity to staphylococcal exotoxins (sterile) |
| Infiltrate position | Any position | Peripheral; clear gap (lucid interval) between infiltrate and limbus |
| Epithelial defect | Yes, at presentation | Absent initially; may develop late |
| AC reaction | Usually present | Usually absent/mild |
| Discharge | Mucopurulent | Minimal |
| Treatment | Intensive antibiotics | Topical steroid + antibiotic combination (the steroid is the main treatment) |
A: (1) Review history and clinical findings - is the diagnosis bacterial keratitis or could it be fungal/Acanthamoeba/HSV? (2) Contact microbiology for latest culture/sensitivity report. (3) Exclude drug toxicity mimicking persistent infection (ciprofloxacin precipitates, worsening SPK from preservatives). (4) If organisms identified: change to organism-specific agent; consider fortified antibiotics if not started. (5) If cultures negative and no improvement at 48-72h: consider 24h antibiotic washout + re-scraping with broader media, additional stains (KOH, calcofluor white, ZN). (6) Consider PCR, MDS for atypical organisms. (7) If MRSA suspected: switch to vancomycin. (8) Consider PACK-CXL if corneal melting. (9) Biopsy if cultures remain negative. (10) Surgical options if medical failure is confirmed.
A: Indications: (i) Failure of aggressive medical therapy with progressive disease; (ii) Impending or actual corneal perforation not manageable with glue/BCL; (iii) Corneal perforation with iris prolapse. Timing: "Hot keratoplasty" (during active infection) carries high graft failure/rejection risk due to extensive inflammation, neovascularisation, and ongoing infection. Ideally: control infection first if possible. When performed during active disease, use large enough graft to excise all infected tissue with clear margins. PKP preferred for deep disease; DALK for anterior-mid stromal disease if Descemet's spared (evidence: Onofrei 2026 - DALK shows higher graft survival).
A: Doxycycline is a tetracycline antibiotic used not for its antibacterial effect in this context, but for its anticollagenase (anti-MMP) effect. Mechanism: tetracyclines inhibit matrix metalloproteinases (MMP-2, MMP-9) that are responsible for collagen degradation and stromal melting. Dose: 100 mg orally twice daily. Indication: impending or actual corneal perforation with significant thinning, or severe keratolysis. Combined with systemic ciprofloxacin (for antibacterial effect) in perforation situations.
A: P. aeruginosa forms biofilms on contact lens surfaces and potentially within corneal tissue. Biofilms: (i) resist antibiotic penetration (organisms within biofilm can tolerate 100-1000× higher antibiotic concentrations than planktonic bacteria); (ii) prevent phagocytic killing; (iii) provide a reservoir for repeated seeding. Clinical implications: (a) Contact lenses and cases MUST be discarded and cultured; (b) Fluoroquinolone resistance within biofilm even if sensitivity testing suggests susceptibility; (c) Explains why some CL-related Pseudomonas infections fail monotherapy; (d) PACK-CXL may be helpful as UV disrupts biofilm structure.
give me the note of viral corneal ulcer from basic to advanced level from the standard textbooks and add images to it, any clinical trials and recent advances. write it in chat and write about the viva questions that can be asked here
"herpes simplex keratitis" AND treatment
"herpetic keratitis" OR "herpes zoster ophthalmicus" AND antiviral treatment
"herpes simplex keratitis" AND recurrence prevention acyclovir valacyclovir HEDS
🦠 Viral Corneal Ulcer (Viral Keratitis)
Complete Clinical Notes - Basic to Advanced Level
1. OVERVIEW & IMPORTANCE
Kanski's 10th: "Herpetic eye disease is the most common infectious cause of corneal blindness in developed countries. As many as 60% of corneal ulcers in developing countries may be the result of herpes simplex virus and 10 million people worldwide may have herpetic eye disease. Approximately 10% of those who have any history of herpes simplex keratitis (HSK) will eventually have a final visual acuity of less than 6/60."
| Virus | Type | Corneal Involvement |
|---|---|---|
| Herpes Simplex Virus Type 1 (HSV-1) | DNA - Herpesviridae | Dendritic, geographic, disciform, stromal, neurotrophic keratitis |
| Herpes Simplex Virus Type 2 (HSV-2) | DNA - Herpesviridae | Neonatal; rarely in adults above waist |
| Varicella Zoster Virus (VZV) | DNA - Herpesviridae | Herpes Zoster Ophthalmicus (HZO) - pseudo-dendrite, stromal, neurotrophic |
| Adenovirus | DNA - Adenoviridae | Epidemic keratoconjunctivitis (EKC) - subepithelial infiltrates, no true ulcer |
| Epstein-Barr Virus (EBV) | DNA - Herpesviridae | Rare interstitial keratitis |
| Cytomegalovirus (CMV) | DNA - Herpesviridae | Endothelitis/keratitis in immunocompromised |
2. PART A: HERPES SIMPLEX KERATITIS (HSK)
2.1 THE VIRUS
- Enveloped, linear double-stranded DNA virus
- Icosahedral capsid; surrounded by tegument and lipid envelope
- Two subtypes:
- HSV-1: infections above the waist; principally face, lips, eyes
- HSV-2: sexually acquired; genital herpes; rarely ocular (neonatal conjunctivitis)
- Resides latent in virtually all neuronal ganglia - particularly the trigeminal (Gasserian) ganglion for ocular disease
- Transmission: droplet spread, direct inoculation, contact with infected secretions
- Ubiquitous: >90% of adults worldwide are HSV-1 seropositive
2.2 PATHOGENESIS & LIFECYCLE
Primary infection (usually childhood, subclinical)
↓
Virus travels retrograde along sensory axons
↓
Establishes LATENCY in trigeminal ganglion
↓
Reactivation triggers (stress, UV, illness, immunosuppression, fever, trauma, menstruation)
↓
Anterograde axonal transport to cornea/skin
↓
Active viral replication in corneal epithelium
↓
[Type depends on host immune response + site]
↓
Epithelial keratitis (active viral lysis) OR
Stromal/Disciform keratitis (immune-mediated)
- Epithelial keratitis = direct viral cytopathic effect; active virus replication; responds to antivirals
- Stromal/immune keratitis = T-cell mediated hypersensitivity to viral antigen; minimal active virus; responds to steroids (with antiviral cover)
2.3 PRIMARY HSV INFECTION
- Mild fever, malaise, URTI symptoms
- Blepharitis and follicular conjunctivitis
- Vesicular eyelid lesions
- Mild, self-limiting dendritic corneal ulcer may occur
2.4 RECURRENT HSK - CLINICAL PATTERNS
A. EPITHELIAL KERATITIS - DENDRITIC ULCER (Most Common)
- Mild-to-moderate ocular discomfort (NOT severe pain - because corneal anaesthesia reduces sensation)
- Redness, photophobia, watering
- Blurred vision
- Foreign body sensation
- Swollen opaque epithelial cells in coarse punctate or stellate pattern (earliest sign)
- Central desquamation → classic dendritic (branching) ulcer, usually central
- Branches have characteristic terminal end-bulbs (club-shaped terminal buds) - pathognomonic
- Bed of ulcer stains with fluorescein (green - epithelial defect)
- Margins stain with rose Bengal (viral-laden cells at ulcer edge are devitalised)
- Reduced corneal sensation (hypesthesia) - a key distinguishing feature
- Mild subepithelial haze underneath the ulcer
- Mild AC reaction (usually not severe)
- Vesicular eyelid lesions may coincide
- Follicular conjunctivitis (may also be caused by topical antivirals)
- IOP may be elevated (tonometry on unaffected eye first)
- Following healing: persistent punctate epithelial erosions (PEE) settle spontaneously
IMAGE: HSV Dendritic Ulcer - Fluorescein
B. GEOGRAPHIC / AMOEBOID ULCER
- Dendritic ulcer is treated with topical steroids inadvertently (most common cause)
- May also enlarge spontaneously in severe disease or immunosuppression
IMAGE: HSV Geographic Ulcer (post-steroid enlargement)
C. DISCIFORM KERATITIS (Endothelial / Stromal - Immune Mediated)
- Gradual onset blurred vision (haloes around lights)
- Discomfort and redness - milder than purely epithelial disease
- Clear past history of epithelial ulceration is NOT always present
- Central zone of stromal oedema with overlying epithelial oedema (the defining feature)
- Large (granulomatous) keratic precipitates (KPs) underlying the oedema
- Descemet membrane folds in severe cases
- Wessely immune ring - ring of deep stromal haze from deposition of viral antigen + host antibody complexes; this is a ring precipitate and is pathognomonic
- IOP may be elevated (secondary herpetic uveitis/trabeculitis)
- Reduced corneal sensation
- Healed lesions: faint ring of stromal/subepithelial opacification + thinning
- Repeated episodes: progressive stromal/subepithelial scarring + superficial/deep vascularisation
IMAGES: Disciform Keratitis
D. NECROTISING STROMAL KERATITIS
- Less common; most destructive form
- Direct viral invasion of stroma (unlike disciform which is immune-mediated)
- Dense stromal infiltrate with necrosis and tissue loss
- May lead to stromal melting, perforation
- May occur with or without an overlying epithelial defect
- Often associated with severe anterior uveitis and hypopyon
- Treatment: antivirals + careful use of steroids + cycloplegia
E. NEUROTROPHIC KERATOPATHY (Post-herpetic)
- Occurs from corneal nerve damage from repeated herpetic episodes
- Leads to persistent epithelial defect with sterile oval/round ulcer (not from active virus)
- Oval or elliptical ulcer with rolled, heaped edges (not infiltrated)
- Located inferior to visual axis typically
- No infiltrate - this is the key distinguishing feature from active infection
- Progressive thinning → descemetocele → perforation
- Treatment: lubricants, BCL, tarsorrhaphy, cenegermin (NGF drops)
2.5 INVESTIGATIONS
| Test | Finding |
|---|---|
| Corneal scraping + Giemsa stain | Multinucleated giant cells (Tzanck cells) |
| Rose Bengal staining | Stains devitalised cells and viral-laden ulcer margins |
| Viral culture (viral transport medium) | HSV isolation |
| PCR (aqueous/corneal scraping) | Highly sensitive; gold standard when diagnosis uncertain |
| Immunocytochemistry | HSV antigen detection |
| HSV serology (IgG/IgM) | Rises only on PRIMARY infection; confirms past exposure (IgG) |
| Corneal sensation testing | Reduced (cotton wisp test; aesthesiometry) |
2.6 TREATMENT
Epithelial Keratitis (Dendritic / Geographic) - Active Virus
- Aciclovir 3% ointment - 5 times daily for 14 days (or 3 days after healing)
- Ganciclovir 0.15% gel - 5 times daily; better tolerated; no preservative toxicity
- Duration: minimum 2 weeks; stop 3-5 days after healing to avoid toxicity
- Aciclovir 400 mg 5x/day OR valaciclovir 500 mg TDS - for geographic ulcers or if topical poorly tolerated
- Oral route achieves higher aqueous humour levels for stromal disease
- Topical steroids in epithelial/active viral keratitis → expand dendritic to geographic ulcer → can cause severe, progressive ulceration and corneal destruction
- Historical method (removing virus-laden epithelium); less used now; topical antivirals preferred
- May be used as adjunct in large geographic ulcers
- Cyclopentolate 1% or atropine 1% if significant AC reaction
Disciform Keratitis (Immune-Mediated Stromal) - NOT active virus
- Prednisolone 0.5-1% QID, tapering slowly over weeks-months
- CRITICAL: Must never withdraw steroids abruptly - risk of rebound inflammation
- Taper very slowly; most patients require long-term low-dose maintenance
- Topical aciclovir 3% ointment 3x/day OR
- Oral aciclovir 400 mg BD (prophylactic dose) - ensures epithelial disease does not reactivate under steroid cover
Necrotising Stromal Keratitis
- Oral aciclovir (high dose: 400 mg 5x/day)
- Topical steroids with antiviral cover (more cautious than in disciform)
- Cycloplegia
- Consider PKP if progressive/unresponsive
Neurotrophic Keratopathy (Post-herpetic)
- Preservative-free lubricants hourly
- Bandage contact lens (supervised carefully)
- Tarsorrhaphy for persistent defects
- Cenegermin 0.002% (Oxervate) - recombinant human nerve growth factor (NGF); approved for Stage 2-3 neurotrophic keratopathy; promotes epithelial healing and nerve regeneration
- Autologous serum drops - contains growth factors; promotes epithelial healing
2.7 LONG-TERM PROPHYLAXIS (SECONDARY PREVENTION)
- HEDS I: Oral aciclovir 400 mg BD for 12 months reduces HSK recurrence by ~50% in patients with ≥1 episode of stromal disease
- HEDS Prophylaxis Trial: Oral aciclovir 400 mg BD significantly reduced: recurrences of stromal keratitis (by 28%), recurrences of all HSK (by 45%), and recurrences with vision-threatening complications
- Prolonged antivirals vs placebo: RR 0.56 (95% CI 0.45-0.70), NNT=6 for preventing ocular recurrences
- Aciclovir better than placebo: RR 0.59, NNT=8
- Aciclovir equivalent to valaciclovir (RR 1.0)
- Stromal keratitis reduction: RR 0.55 (95% CI 0.35-0.85), NNT=17
- No difference in adverse effects
- Evidence quality: HIGH for ocular and non-ocular recurrences
- Oral aciclovir 400 mg BD (twice daily) - for 12 months or longer in patients with:
- ≥2 recurrences per year
- Any stromal disease
- Pre-keratoplasty or post-keratoplasty
- Severe or vision-threatening disease
- Oral valaciclovir 500 mg OD - equivalent, better bioavailability, once-daily dosing is more convenient
3. PART B: HERPES ZOSTER OPHTHALMICUS (HZO) / VZV KERATITIS
3.1 THE VIRUS & PATHOGENESIS
- Enveloped linear double-stranded DNA virus; Herpesviridae family
- Primary infection = Chickenpox (varicella) - usually childhood
- Virus then establishes latency in dorsal root ganglia and cranial nerve ganglia (including trigeminal)
- Reactivation = Herpes Zoster (shingles)
- Risk factors for reactivation: advancing age, immunosuppression, stress, malignancy
- The most important cranial nerve involvement in zoster
- Incidence increases markedly after age 50
- Risk of ophthalmic complications is ~50% in HZO
3.2 HUTCHINSON'S SIGN
If VZV involves the nasociliary branch of V1 → produces vesicles on the tip and side of the nose (Hutchinson's sign)
IMAGE: Herpes Zoster Ophthalmicus - skin rash

3.3 OCULAR FEATURES OF HZO
- Papillary or follicular conjunctivitis
- Episcleritis / scleritis (acute or chronic)
| Type | Features |
|---|---|
| Pseudodendrites (early) | Raised, mucous plaques on epithelium; no true terminal buds; shorter, thicker than HSV dendrites; stain poorly with fluorescein but stain with rose Bengal |
| Epithelial keratitis | Coarse punctate epithelial erosions; mucous plaques |
| Nummular (coin-shaped) keratitis | Multiple discrete anterior stromal infiltrates (granular, coin-shaped) - most characteristic of VZV |
| Disciform keratitis | Similar to HSV disciform; central stromal oedema + granulomatous KPs |
| Interstitial keratitis | Diffuse stromal inflammation with vascularisation |
| Neurotrophic keratopathy | Late complication; persistent epithelial defect from V1 anaesthesia |
- Iritis/iridocyclitis - common; may cause posterior synechiae
- Sector iris atrophy (loss of sphincter pattern) - from ischaemia of iris vessels by VZV; pathognomonic of HZO
- Raised IOP (trabeculitis)
- Vitritis, retinitis (acute retinal necrosis - ARN - in immunocompromised)
- Optic neuritis (rare)
- Ophthalmoplegia (CN III, IV, VI palsy from nerve invasion)
- Postherpetic neuralgia
3.4 KEY DIFFERENCE: HSV vs VZV KERATITIS
| Feature | HSV Dendrite | VZV Pseudo-dendrite |
|---|---|---|
| Morphology | True branching dendrite; linear | Raised mucous plaque; stellate; irregular |
| Terminal buds | Present (pathognomonic) | Absent |
| Fluorescein staining | Strong (epithelial defect) | Weak or absent (mucus overlying intact epithelium) |
| Rose Bengal | Positive at margins | Positive (devitalised cells) |
| Corneal sensation | Reduced | Reduced |
| Associated skin rash | No rash OR cold sore | Dermatomal V1 rash |
| Bilaterality | Never bilateral (except immunosuppressed) | Never bilateral |
3.5 TREATMENT OF HZO
Systemic Antiviral (First-line) - Must start within 72 hours ideally
| Drug | Dose | Duration |
|---|---|---|
| Valaciclovir (preferred) | 1 g TDS | 7-10 days |
| Famciclovir | 250-500 mg TDS | 7-10 days |
| Aciclovir | 800 mg 5x/day | 7-10 days |
| Brivudine | 125 mg OD (some countries) | 7 days - NEVER with 5-fluorouracil (fatal interaction) |
Topical Ophthalmic Treatment
- Topical aciclovir 3% ointment or ganciclovir 0.15% gel for corneal epithelial disease
- Topical steroids (with antiviral cover) for disciform/stromal keratitis
- Cycloplegia for uveitis
- IOP-lowering drops if trabeculitis/glaucoma (avoid prostaglandins)
- Lubricants for neurotrophic keratopathy
Systemic Steroids (Controversial)
- E.g. Prednisolone 60 mg daily × 4 days → 40 mg × 4 days → 20 mg × 4 days
- Confer moderate reduction in acute pain and accelerated skin healing
- Do NOT reduce incidence or severity of postherpetic neuralgia
- Avoid in immunodeficiency
3.6 POSTHERPETIC NEURALGIA (PHN)
- Persistent pain in V1 distribution >3 months after acute HZO
- Occurs in ~10-15% of HZO patients
- Management: gabapentin, pregabalin, tricyclic antidepressants, capsaicin patches, lidocaine patches
- VZV vaccine significantly reduces PHN risk
4. THE ZOSTER EYE DISEASE STUDY (ZEDS) - LANDMARK 2025 RCT
Design:
- International, multicenter, randomised, double-masked, placebo-controlled trial
- 95 sites; 527 participants; November 2017 - June 2024
- Population: immunocompetent adults with history of HZO rash, documented active keratitis or iritis within 1 year
- Intervention: suppressive valacyclovir 1000 mg daily × 12 months vs placebo
- Primary outcome: time to first new or worsening stromal keratitis (SK), endothelial keratitis (EK), iritis, or dendriform epithelial keratitis (DEK)
ZEDS Results - Corneal/Ocular Disease:
- Placebo: 33% experienced primary endpoint
- Valacyclovir: 28% experienced primary endpoint
- HR 0.77 (95% CI 0.56-1.05; P = 0.09) - not significant
- Placebo: 40% | Valacyclovir: 32%
- HR 0.73 (95% CI 0.55-0.97; P = 0.03) - significant
- Also significant: reduced number of multiple episodes at both 12 and 18 months (HR 0.70, P=0.02)
ZEDS Results - Postherpetic Neuralgia:
- Valacyclovir did NOT significantly reduce prevalence of PHN at 12 months (38% vs 40%)
- BUT: patients <60 years with chronic HZO had lower pain scores at 12 and 18 months
- Pain duration significantly reduced with valacyclovir at 18 months (13.6 vs 18.7 months, P=0.046)
- Total daily neuropathic pain medication lower with valacyclovir at 12 and 18 months
ZEDS Clinical Implication:
"Although the primary outcome did not show a benefit of suppressive valacyclovir treatment, secondary study outcomes showed treatment superiority at the 18-month endpoint and reduced number of multiple episodes of keratitis or iritis at both 12 and 18 months. These results support consideration of 1 year of suppressive valacyclovir treatment for HZO."
5. HEDS TRIALS (HISTORICAL LANDMARK - STILL GOLD STANDARD FOR HSK)
| HEDS Trial | Finding |
|---|---|
| HEDS I - Acyclovir Prevention Trial | Oral aciclovir 400 mg BD × 12 months: reduced recurrence of HSK by 45%; reduced stromal keratitis by 28% |
| HEDS - Topical Steroids for Stromal Keratitis | Topical steroids accelerate resolution of stromal keratitis and reduce treatment failure |
| HEDS - Debridement for Dendritic Keratitis | No significant benefit of debridement when added to topical antiviral |
| HEDS - Iridocyclitis Trial | Oral aciclovir added to topical steroid did NOT reduce risk of iridocyclitis |
6. SYSTEMATIC REVIEW - PROLONGED ANTIVIRALS FOR HSK (2025)
| Outcome | Result | Certainty |
|---|---|---|
| Ocular HSK recurrences | RR 0.56 (0.45-0.70) NNT=6 | HIGH |
| Non-ocular herpetic recurrences | RR 0.56 (0.44-0.71) NNT=6 | HIGH |
| Recurrences with stromal keratitis | RR 0.55 (0.35-0.85) NNT=17 | HIGH |
| Adverse effects | RR 0.96 (not significant) | LOW |
| Aciclovir vs valaciclovir | RR 1.0 - equivalent | Moderate |
| Visual acuity outcomes | No data available | - |
7. ADENOVIRAL KERATITIS (EKC)
- Caused by adenoviruses 8, 19, 37 (all group D adenoviruses)
- Highly contagious; spread by direct contact, fomites, contaminated instruments
- Phase 1 (day 1-14): Acute follicular conjunctivitis, watery discharge, lid oedema, preauricular lymphadenopathy
- Phase 2 (day 5-14): Subepithelial infiltrates (SEIs) appear - small, coin-shaped, multifocal, diffuse - from immune reaction to viral antigen in Bowman's layer; SEIs can persist for months/years and affect vision
- No true ulcer - but epithelial pseudo-membrane formation can occur
- No specific treatment - self-limiting; lubricants, cold compresses
- Topical steroids for vision-threatening SEIs only (with careful monitoring - do NOT clear SEIs permanently, may prolong course)
- Povidone-iodine 1% - emerging antiviral; reduces duration
8. CMV KERATITIS / ENDOTHELITIS
- Rare; mainly in immunocompromised (post-transplant, HIV)
- Linear or coin-shaped endothelial precipitates tracking along endothelium
- Corneal oedema from endothelial dysfunction
- Unilateral; resistant to conventional treatment
- Diagnosis: PCR of aqueous humor for CMV DNA
- Treatment: Topical ganciclovir + systemic valganciclovir
9. COMPLICATIONS
- Corneal scarring - permanent leukoma after each recurrence; cumulative after multiple episodes
- Corneal vascularisation (superficial + deep) - from chronic stromal inflammation
- Corneal anaesthesia - CN V damage → neurotrophic keratopathy
- Recurrent episodes - each episode adds scarring; ~10% eventually reach VA <6/60
- Persistent epithelial defect - neurotrophic origin
- Secondary bacterial/fungal superinfection - particularly in neurotrophic ulcers
- Herpetic iridocyclitis - posterior synechiae, raised IOP, angle closure
- Steroid-induced complications - glaucoma, cataract from long-term topical steroids (necessary for disciform)
- Corneal graft failure - recurrence in graft is common; prophylactic aciclovir reduces this risk
10. KEY MANAGEMENT PEARLS
- Never use topical steroids in active viral epithelial keratitis - the single most important rule
- Topical steroids ARE the treatment for disciform keratitis - but always with antiviral cover
- Reduced corneal sensation is the clue to herpetic origin in any unusual corneal ulcer
- The Wessely immune ring = viral antigen-antibody complex deposition; pathognomonic of disciform HSV/VZV keratitis
- VZV pseudodendrite vs HSV dendrite: VZV has no terminal buds, raised plaque, weak fluorescein, strong rose Bengal
- IOP must be monitored at every herpetic keratitis visit - herpetic trabeculitis is common
- Hutchinson's sign (nasal tip vesicles) = predict high risk of ocular involvement in HZO
- Long-term prophylactic aciclovir 400 mg BD - NNT=6 to prevent recurrence; consider in any patient with ≥2 recurrences or stromal disease
- Ganciclovir 0.15% gel is preferred over aciclovir ointment by many centres (better tolerability, no greasy film)
- Prostaglandin analogues for IOP - use with caution; may theoretically trigger HSV reactivation (case reports)
🎓 VIVA QUESTIONS - VIRAL CORNEAL ULCER
🔵 BASIC LEVEL
A: HSV-1 (most common; dendritic, geographic, disciform keratitis), VZV (HZO; pseudodendrites, disciform, neurotrophic), and rarely EBV, CMV (endothelitis in immunocompromised). Adenovirus causes EKC but true stromal ulcers are uncommon.
A: In the trigeminal (Gasserian) ganglion for ocular disease. After primary infection, virus travels retrograde along sensory axons to the ganglion where it persists in a latent state. On reactivation triggers (stress, UV, fever, illness, immunosuppression, menstruation, trauma), the virus travels anterograde back to the cornea and skin.
A: A linear-branching (dendritic) epithelial ulcer, most frequently central. It has characteristic terminal end-bulbs (club-shaped tips) which are pathognomonic. The bed of the ulcer stains bright green with fluorescein. The virus-laden cells at the margins stain with rose Bengal. There is reduced corneal sensation. Mild subepithelial haze is typically present.
A: Topical aciclovir 3% ointment 5x daily for 14 days (or 3 days after healing). Alternatively, ganciclovir 0.15% gel 5x daily - better tolerated. Oral aciclovir (400 mg 5x/day) or valaciclovir for geographic ulcers. Cycloplegia if AC reaction. NEVER topical steroids.
A: Vesicles on the tip and side of the nose in HZO, indicating involvement of the nasociliary branch of V1. This branch also supplies the eye via the long ciliary nerves. Hutchinson's sign positive predicts ~76% risk of ocular complications (vs ~34% without), including keratitis, uveitis, and raised IOP.
A: Oral valaciclovir 1 g TDS (preferred for convenience and bioavailability) or famciclovir 500 mg TDS or aciclovir 800 mg 5x/day for 7-10 days. Must start within 72 hours of rash onset (or still at vesicular stage). Reduces severity, duration, ophthalmic complications by ~50%, and risk of PHN.
A: HSV dendrite: true branching pattern, terminal end-bulbs present, bed stains strongly with fluorescein (true epithelial defect), margins stain with rose Bengal, associated with cold sore history. VZV pseudodendrite: raised mucous plaque, no true terminal buds, weak or absent fluorescein staining (mucus overlying mostly intact epithelium), stains with rose Bengal, associated with V1 dermatomal rash.
🟡 INTERMEDIATE LEVEL
A: Disciform keratitis is immune-mediated stromal disease caused by T-cell hypersensitivity to HSV or VZV antigens trapped in the stroma. It is NOT active viral replication. The key distinction: (1) Dendritic keratitis = active viral lysis of epithelial cells - responds to antivirals, steroids are harmful; (2) Disciform keratitis = immune reaction in stroma - steroids are the main treatment, antivirals are used only as cover. Signs: central disc of stromal oedema, granulomatous KPs, Wessely ring, elevated IOP, reduced corneal sensation.
A: A deep stromal ring of grey-white haze surrounding the central oedema in disciform keratitis. It represents precipitation of HSV (or VZV) viral antigens with host antibodies in the deep stroma - a type III (immune complex-mediated) hypersensitivity reaction. It is virtually pathognomonic of herpetic disciform keratitis.
A: Topical steroids suppress the host immune response that limits viral replication. In active epithelial disease, this allows: (1) Uncontrolled viral replication; (2) Expansion of the dendritic ulcer into a large geographic/amoeboid ulcer with scalloped edges; (3) Deeper stromal invasion; (4) Possible corneal perforation. The geographic ulcer from steroid use is the result of viral lysis of large areas of epithelium uncontrolled by host immunity. Management: immediately start intensive topical antiviral; stop steroid; monitor closely for progression.
A: The Herpetic Eye Disease Study (HEDS) was a series of NIH-funded RCTs: (1) HEDS Prevention Trial: Oral aciclovir 400 mg BD × 12 months reduced HSK recurrence by 45% overall; reduced stromal keratitis by 28%. (2) HEDS Stromal Trial: Topical steroids accelerated resolution of stromal disease and reduced treatment failure. (3) Debridement trial: No added benefit of debridement when topical antiviral is used. Clinical application: aciclovir 400 mg BD prophylaxis for ≥12 months in patients with ≥2 recurrences per year, any stromal disease, pre/post-keratoplasty, or vision-threatening HSK.
A: Aciclovir is an acyclic guanosine analogue (purine nucleoside analogue). (1) It enters virus-infected cells and is first phosphorylated by viral thymidine kinase (TK) to aciclovir monophosphate - this step is highly selective for infected cells. (2) Host cellular kinases phosphorylate it to aciclovir triphosphate (active form). (3) Aciclovir triphosphate competitively inhibits viral DNA polymerase and acts as a chain terminator when incorporated into viral DNA - the 3'-OH group required for chain elongation is absent. (4) Net effect: selective inhibition of HSV DNA replication in infected cells only. Valaciclovir is the L-valyl ester prodrug of aciclovir with ~3-5x higher oral bioavailability.
A: This is disciform keratitis with herpetic trabeculitis/uveitis causing raised IOP. Management: (1) Topical prednisolone 1% QID to treat the immune-mediated inflammation; (2) Mandatory antiviral cover: oral aciclovir 400 mg BD or topical aciclovir 3% ointment TDS; (3) IOP lowering: topical beta-blocker (timolol 0.5%) + topical carbonic anhydrase inhibitor (dorzolamide); consider acetazolamide oral if very high. Do NOT use prostaglandin analogues (theoretical risk of HSV reactivation). (4) Cycloplegia (atropine/cyclopentolate) for associated uveitis. (5) Monitor IOP every 1-2 weeks; taper steroid very slowly (risk of rebound). Tonometry: use disposable applanation tip; do the normal eye first.
A: Neurotrophic keratopathy is a non-infectious complication from CN V damage. There is NO active virus. Treatment: (1) Preservative-free lubricants - frequent, at least q1-2h; (2) Preservative-free antibiotic ointment at night (prophylaxis against secondary infection); (3) Bandage contact lens - mechanical protection; supervise closely; (4) Tarsorrhaphy (temporary lateral or medial) or botulinum toxin ptosis for large persistent defects; (5) Cenegermin 0.002% (Oxervate) - recombinant human NGF; FDA approved; promotes corneal nerve regeneration and epithelial healing; (6) Autologous serum drops (20-50%) contain EGF, substance P, NGF; promotes epithelial healing; (7) AMG for non-healing cases.
🔴 ADVANCED LEVEL
A: (Cohen EJ et al., JAMA Ophthalmol, 2025; 527 participants, 95 sites, double-masked RCT). Design: Suppressive valacyclovir 1000 mg daily × 12 months vs placebo in immunocompetent adults with HZO and active keratitis/iritis within 1 year. Primary outcome: time to first new or worsening stromal/endothelial keratitis, iritis, or dendriform epithelial keratitis. Results: Primary outcome at 12 months: not significant (HR 0.77, P=0.09). Secondary outcome at 18 months: significant (HR 0.73, P=0.03). Multiple episodes of keratitis/iritis reduced at both 12 and 18 months. PHN (companion paper): no reduction in PHN prevalence, but pain duration reduced and neuropathic medication dose reduced in the valacyclovir group at 18 months. Implication: 1 year of daily suppressive valacyclovir 1g is reasonable for HZO patients with active keratitis/iritis - reduces recurrences of inflammatory eye disease and may reduce PHN burden.
A: FOR (evidence): (1) HEDS Stromal Keratitis Trial: topical prednisolone 1% (added to antiviral cover) significantly accelerated resolution of stromal disease and reduced treatment failure compared to placebo; (2) Pathogenetically rational: stromal disease is T-cell mediated, not active viral - steroids directly address the pathology; (3) Reduces scarring by limiting inflammatory collagen destruction. AGAINST: (1) Risk of activating epithelial disease if antiviral cover lapses; (2) Risk of steroid glaucoma (IOP already elevated in many herpetic eyes); (3) Risk of steroid cataract from long-term use; (4) Rebound inflammation on withdrawal requires very slow tapering; (5) Risk of promoting secondary infection. Current practice: topical steroids ARE indicated for stromal disease with mandatory antiviral cover and very slow taper.
A: PHN mechanism: VZV causes acute ganglionic inflammation with neuronal destruction in the trigeminal ganglion. This leads to: (1) Peripheral sensitisation from axonal damage; (2) Central sensitisation from persistent nociceptive input; (3) Loss of inhibitory interneurons; (4) Abnormal spontaneous discharge from damaged nerve fibres. Classic features: allodynia (pain from non-painful stimuli), burning or lancinating pain, hypersensitivity to cold/wind. ZEDS implication for PHN: suppressive valacyclovir 1g OD does NOT prevent PHN prevalence but reduces pain duration (13.6 vs 18.7 months) and reduces neuropathic medication requirements. Most benefit in younger patients (<60 years) with chronic HZO. Practice change: consider 12 months of suppressive valacyclovir for ALL HZO patients with documented keratitis or iritis, not just for corneal disease but also to reduce PHN burden.
A: Two vaccines available: (1) Zostavax (live attenuated, single dose): reduces zoster incidence by ~51% and PHN by ~67% in adults ≥60; (2) Shingrix (recombinant zoster vaccine, RZV) - two-dose series: >90% efficacy against HZO and PHN; approved for immunocompetent adults ≥50; preferred over Zostavax. VZV vaccine (varicella vaccine in childhood) also reduces primary chickenpox. RZV is now recommended for all adults ≥50 including those with prior zoster episode - provides superior protection and longer duration than Zostavax. Impact: as vaccination rates increase, the incidence of HZO and its ocular complications (including keratitis and neurotrophic ulcers) should decline significantly.
A: HSV recurrence in a corneal graft is a major risk: (1) Virus latent in the trigeminal ganglion can reactivate; (2) Surgical stress + immunosuppressive drops (steroids) prescribed post-graft both trigger reactivation; (3) Recurrence in the graft is the leading non-immunological cause of graft failure in HSV patients. Prophylaxis: oral aciclovir 400 mg BD (or valaciclovir 500 mg OD) indefinitely while on topical steroids, and for at least 1-2 years post-transplant. Evidence: HEDS showed aciclovir reduces recurrence by 45%; additional evidence from keratoplasty-specific studies confirms this. Some centres continue lifelong. Without prophylaxis, recurrence rate post-graft is ~30-50% at 5 years; with prophylaxis, this is reduced by ~50%.
A:
| Feature | Epithelial (Dendritic) | Disciform | Necrotising Stromal |
|---|---|---|---|
| Mechanism | Direct viral cytopathic effect - active replication in epithelium | T-cell immune reaction to viral antigen in stroma | Direct viral invasion of stroma |
| Active virus? | Yes - lots | No (or minimal) | Yes |
| Main treatment | Topical antiviral (aciclovir/ganciclovir) | Topical steroid + antiviral cover | Oral antiviral (high dose) + cautious steroid |
| Steroids role | CONTRAINDICATED | Indicated (main treatment) | Cautious, adjunctive |
| Antivirals role | Main treatment | Cover/prophylaxis only | Main treatment |
| Prognosis | Good; heals in 2 weeks | Good with treatment; recurrences add scarring | Worst; may cause perforation |
| Slit lamp | Dendritic ulcer, terminal buds, + fluorescein | Stromal oedema, granulomatous KPs, Wessely ring | Dense stromal infiltrate + necrosis |
Search for latest clinical guidelines on herpetic keratitis management 2025-2026
"herpetic keratitis" AND guidelines management
herpetic keratitis HSV herpes simplex clinical guidelines 2025 2026 AAO ophthalmology management recommendations
herpetic keratitis HSV VZV guidelines treatment antiviral steroid prophylaxis 2025 2026
"herpes simplex keratitis" OR "herpes zoster ophthalmicus" management review 2025
AAO preferred practice pattern herpes simplex keratitis 2024 2025 update herpetic eye disease guideline antiviral prophylaxis
herpetic keratitis HSV VZV management antiviral dosing prophylaxis steroid ZEDS post-surgical recommendations
"herpes simplex keratitis" antiviral recurrence suppression valacyclovir 2025
📋 Latest Clinical Guidelines on Herpetic Keratitis Management (2025-2026)
1. OVERVIEW OF CURRENT GUIDELINE LANDSCAPE
| Organisation / Document | Year | Scope |
|---|---|---|
| AAO - HSV Keratitis Treatment Guideline (White ML, Chodosh J) | 2014 (still reference standard; no major full update) | HSV keratitis; antiviral dosing; prophylaxis |
| AAO - Cornea/External Disease Summary Benchmarks | December 2024 | Incorporates HEDS evidence + ZEDS |
| RANZCO - HSK Prescribing Protocol & Treatment Guideline | 2020 | Australian/NZ guidance for HSK management |
| NICE / AAO / CDC / ICMR | Various | HZO: early antivirals + ophthalmic referral; universally aligned |
| ZEDS (NCT03134196) | Published April 2025 | Suppressive valacyclovir in HZO - now influencing practice |
| Review of Ophthalmology - Infectious Keratitis Guidelines | September 2025 | Practical synthesis of current evidence |
| Survey of Ophthalmology - Peri-surgical HSV/HZV guidelines | 2025 (PMID 39961450) | Prophylaxis around ocular surgery |
Key point: No new standalone AAO PPP specifically for HSV keratitis has been published since 2014. The 2014 AAO guideline (White/Chodosh) remains the primary reference document, with the AAO Cornea Benchmarks 2024 incorporating updated evidence. HEDS data + ZEDS 2025 are now the principal evidence base.
2. PART A: HSV KERATITIS - CURRENT GUIDELINE POSITIONS
2.1 Treatment by Disease Type (AAO 2014 + HEDS + 2025 Updates)
A. EPITHELIAL (DENDRITIC/GEOGRAPHIC) KERATITIS
| Treatment | Agent | Dose & Duration |
|---|---|---|
| Topical antiviral (first-line for dendrites) | Ganciclovir 0.15% gel (preferred) | 5x daily until 3 days post-healing; max 21 days |
| Aciclovir 3% ointment | 5x daily × 14 days | |
| Oral antiviral (for geographic/severe/intolerant of topical) | Aciclovir | 400 mg 5x daily |
| Valaciclovir | 500 mg TDS | |
| Avoid | Topical steroids | Absolutely contraindicated |
| Avoid | Prolonged topical antiviral | Toxicity: whorled epithelial changes, follicular conjunctivitis |
B. STROMAL KERATITIS WITHOUT ULCERATION (DISCIFORM / IMMUNE STROMAL)
| Component | Recommendation |
|---|---|
| Topical steroid | Start prednisolone 1% QID to q2h (depending on severity); slow taper |
| Steroid taper duration | BEYOND 10 weeks (HEDS showed high treatment failure at 6-week mark; AAO guideline recommends extended taper) |
| Antiviral cover (mandatory) | Oral aciclovir 400 mg BD (prophylactic dose) OR valaciclovir 500 mg OD |
| Duration of antiviral | For the entire duration of steroid use |
| Topical antivirals for steroid cover | NOT recommended long-term - excessive corneal toxicity |
| IOP monitoring | Every visit; treat if elevated; avoid prostaglandins |
| Cycloplegia | If AC reaction present |
Review of Ophthalmology 2025 (Aguwa et al.): "Stromal and endothelial disease require combined antiviral therapy and topical corticosteroids, as supported by the Herpetic Eye Disease Study."
C. STROMAL KERATITIS WITH ULCERATION (NECROTISING)
| Agent | Dose |
|---|---|
| Aciclovir (oral) | 800 mg 5x daily (same as HZO therapeutic dose) |
| Valaciclovir (oral) | 1 g TDS |
From Review of Optometry (HEDS-ZEDS synthesis 2025): "Those with stromal keratitis with ulceration should receive a more aggressive oral antiviral dose. The HZV therapeutic antiviral dose is recommended (e.g., acyclovir 800mg five times a day) and minimal topical steroid to start such as BID."
D. HSV ENDOTHELIITIS
| Agent | Dose |
|---|---|
| Aciclovir | 400 mg 3-5x daily |
| Valaciclovir | 500 mg BD |
| Famciclovir | 250 mg BD |
| Topical steroid | q1-2h (high frequency initially) with slow taper |
| Antiviral cover | For entire steroid course |
2.2 Oral Antiviral Dosing Summary (Critical for Exams and Practice)
| Indication | Aciclovir Dose | Valaciclovir Equivalent |
|---|---|---|
| Epithelial keratitis (therapeutic) | 400 mg 5x daily | 500 mg TDS |
| Stromal keratitis with ulceration (therapeutic) | 800 mg 5x daily | 1 g TDS |
| Disciform/immune stromal (antiviral cover with steroid) | 400 mg BD (prophylactic) | 500 mg OD |
| Prophylaxis/suppression (recurrence prevention) | 400 mg BD | 500 mg OD |
| Endotheliitis | 400 mg 3-5x daily | 500 mg BD |
| Post-keratoplasty (indefinite while on steroids) | 400 mg BD | 500 mg OD |
Key principle from AAO/HEDS guidelines: HSV oral antiviral doses are generally HALF those used for HZV. For HZV (HZO), therapeutic doses are higher (valaciclovir 1 g TDS; aciclovir 800 mg 5x daily).
2.3 Suppressive Prophylaxis (Long-term) - Current Evidence Base 2025
- Patients with ≥2 recurrences per year of any HSK
- Any patient with stromal keratitis (history of)
- Pre- and post-corneal transplant (keratoplasty)
- Post-refractive surgery (LASIK, PRK) in patients with HSV history
- During any topical steroid course for immune stromal disease
- Pre- and post-cataract surgery in high-risk patients
- Immunocompromised patients with HSK history
- Minimum 12 months (HEDS evidence)
- Post-keratoplasty: indefinitely while on topical steroids; consider 2 years minimum
- Many corneal specialists continue indefinitely in patients with prior stromal disease
- Aciclovir/valaciclovir equivalent: RR 1.0 (no difference between the two)
- Both reduce ocular recurrences by 44% (NNT=6)
- Reduce stromal keratitis recurrences by 45% (NNT=17)
- No additional adverse effects vs placebo
3. PART B: PERI-SURGICAL HSV/HZV PROPHYLAXIS (NEW 2025 GUIDELINE)
3.1 Cataract Surgery
- Surgical stress (UV exposure, inflammation, steroid drops post-op)
- Topical steroids prescribed post-operatively
- Concurrent NSAIDs (reduce corneal innervation)
- Start oral aciclovir 400 mg BD (or valaciclovir 500 mg OD) at the time of surgery
- Continue for at least 1 month postoperatively or until topical anti-inflammatory agents discontinued
- Patients already on oral antivirals: maintain dose or increase for peri-operative period
- Patients with active stromal disease on steroids: increase steroids 1 week pre-operatively + continue oral antiviral throughout
3.2 Penetrating Keratoplasty (PKP) / Corneal Transplant
- Pre-operative: Oral aciclovir 400 mg BD (or valaciclovir) should be started pre-operatively and continued
- Post-operative: Continue prophylaxis for as long as the patient is on topical steroids (minimum 1-2 years; many centres continue indefinitely)
- Without prophylaxis: 27-50% recurrence rate at 2 years post-PKP
- With prophylaxis: recurrence rate reduced to ~0-5% at 16 months (AAO 2014 guideline data)
- HEDS data shows: The protective effect of 1 year of prophylaxis extends even beyond the treatment year - most recurrences occur in the first year post-graft
3.3 Corneal Cross-Linking (CXL)
- UV-A and riboflavin used in CXL can trigger HSV reactivation (UV is a known reactivation trigger)
- Recommendation: Screen for HSV history; provide oral antiviral prophylaxis for at least 4 weeks peri-CXL
3.4 LASIK / Refractive Surgery
- Flap creation, UV exposure, and post-op steroid drops are reactivation triggers
- History of HSK: oral aciclovir 400 mg BD for 1 month perioperatively
- Monitor carefully for flap interface HSK post-LASIK (cracked windshield infiltrate pattern)
3.5 Glaucoma Surgery (Trabeculectomy, Tube Implants)
- Post-operative inflammation and steroid use trigger reactivation
- Prophylactic oral antiviral peri-operatively in high-risk patients
4. PART C: HZO (VZV KERATITIS) - CURRENT GUIDELINE POSITIONS 2025
4.1 Acute HZO - Multi-Society Consensus
| Priority | Recommendation |
|---|---|
| 1. Speed | Start systemic antivirals within 72 hours of rash onset (benefit extends to vesicular stage) |
| 2. Antiviral choice | Valaciclovir 1 g TDS × 7-10 days (preferred for convenience) OR famciclovir 500 mg TDS OR aciclovir 800 mg 5x/day |
| 3. Ophthalmic referral | Same day/urgent referral if Hutchinson's sign, eye pain, vision changes, or periocular involvement |
| 4. Examination | Slit-lamp examination within 24 hours of diagnosis if ocular involvement suspected |
| 5. Immunocompromised | IV aciclovir 10 mg/kg TID; infective disease specialist input |
4.2 Suppressive Therapy for HZO - ZEDS 2025 (Major Guideline Change)
"These results support consideration of 1 year of suppressive valacyclovir treatment for HZO" - ZEDS authors (JAMA Ophthalmol 2025)
| Patient Group | Recommendation |
|---|---|
| HZO with documented keratitis or iritis within 1 year | Consider valaciclovir 1000 mg OD × 12 months suppression |
| Recurrent or chronic HZO keratitis | Suppressive valaciclovir 1g daily (ZEDS: reduces multiple episodes; HR 0.70, P=0.02 at 12 months) |
| HZO + postherpetic neuralgia, age <60, chronic disease | Strongest indication for suppression (reduced pain scores, duration, medication use) |
| Immunocompetent, single episode, no recurrence | Individualise; suppression may still be considered |
4.3 Ocular Manifestation-Specific Treatment
| Manifestation | Treatment |
|---|---|
| Pseudodendrites | Oral antivirals (systemic, same as acute HZO); topical ganciclovir/aciclovir adjunctive |
| Disciform/stromal keratitis | Topical prednisolone 1% + oral antiviral cover; slow taper |
| Nummular keratitis (coin lesions) | Topical steroids (low-moderate dose) + antiviral; lesions may persist for years |
| Neurotrophic keratopathy | Cenegermin (Oxervate), lubricants, tarsorrhaphy; no active virus |
| Uveitis/iritis | Topical steroids + cycloplegia + IOP monitoring; systemic antiviral if active HZO |
| Raised IOP (trabeculitis) | Beta-blockers, CAI; avoid prostaglandins; treat underlying HZO |
5. PART D: NEUROTROPHIC KERATOPATHY - 2025-2026 GUIDELINE POSITION
| Stage | Features | Treatment |
|---|---|---|
| Stage 1 | Superficial punctate keratopathy, epithelial irregularity | Intensive preservative-free lubricants; discontinue toxic drops |
| Stage 2 | Persistent epithelial defect | Cenegermin 0.002% eye drops 6x daily × 8 weeks + lubricants + BCL |
| Stage 3 | Deep stromal ulcer, risk of perforation | Cenegermin 6x daily × 8 weeks + tarsorrhaphy ± AMG |
6. BIOMARKERS & EMERGING THERAPEUTICS (2026)
- High recurrence rates despite antiviral use (30-50% recur off prophylaxis)
- Long-term steroid adverse effects (glaucoma, cataract)
- No reliable way to predict recurrence risk
| Biomarker | Clinical Utility |
|---|---|
| Aptamer-based detection tools | Rapid bedside HSV antigen detection from corneal scrapings; may replace culture |
| Heparanase activity assays | Heparanase promotes HSV entry into cells; elevated levels predict viral activity and recurrence |
| Matrix metalloproteinases (MMP-2, MMP-9) | Correlate with stromal disease severity and corneal melting risk; potential monitoring tool |
| Approach | Status |
|---|---|
| HSV vaccine development | Multiple platforms under clinical development (subunit, mRNA, vector); none yet approved for ocular disease |
| Gene silencing (siRNA) | Targeting HSV ICP0 and ICP34.5 to prevent reactivation; preclinical |
| CRISPR-Cas9 | Disruption of HSV genome in latently infected trigeminal ganglion cells; animal studies |
| Topical povidone-iodine (0.6-1%) | Antiviral + antibacterial; adjunctive for EKC; under trial for HSV epithelial keratitis |
| Ultraviolet-A therapy | Growing interest (PMID 40177280 bibliometric analysis shows burst keyword "ultraviolet A" since 2018); PACK-CXL as anti-HSV adjunct |
7. SUMMARY TABLE: KEY GUIDELINE POSITIONS 2025-2026
| Clinical Question | Current Guideline Position | Source |
|---|---|---|
| First-line for dendritic ulcer | Ganciclovir 0.15% gel 5x/d OR aciclovir 3% ointment 5x/d for 14 days | AAO 2014; RANZCO 2020 |
| Preferred oral antiviral for epithelial HSK | Valaciclovir 500 mg TDS (better bioavailability) | RANZCO 2020; AAO 2024 Benchmarks |
| Steroid in dendritic ulcer | ABSOLUTELY CONTRAINDICATED | All guidelines |
| Steroid taper duration for stromal HSK | >10 weeks (slow taper beyond HEDS' original 10 weeks) | AAO guideline 2025 update |
| Antiviral during steroid course | Oral aciclovir 400 mg BD (or valaciclovir 500 mg OD) for ENTIRE steroid course | AAO; HEDS |
| Prophylaxis dose for HSK | Aciclovir 400 mg BD or valaciclovir 500 mg OD | AAO 2014; Ruiz Sifre 2025 |
| Duration of prophylaxis | ≥12 months; indefinitely if post-keratoplasty on steroids | AAO 2014; HEDS |
| Acute HZO antiviral | Valaciclovir 1 g TDS × 7-10 days within 72h | AAO; CDC; NICE; ICMR |
| Suppressive valaciclovir for HZO | Valaciclovir 1000 mg OD × 12 months - now supported by ZEDS 2025 | ZEDS 2025 (PMID 40048183) |
| Pre-surgical prophylaxis (HSV history) | Start aciclovir 400 mg BD at time of surgery; continue ≥1 month | Ghafarian 2025 (PMID 39961450) |
| Post-PKP prophylaxis | Indefinitely while on steroids; minimum 2 years | AAO 2014; Ghafarian 2025 |
| Neurotrophic keratopathy | Cenegermin (Oxervate) 0.002% 6x daily × 8 weeks (Stage 2-3) | FDA; NICE approved |
| Prostaglandins in herpetic uveitis/glaucoma | Use with caution (theoretical reactivation risk) | Expert consensus |
8. WHAT IS CURRENTLY LACKING / GAPS
- No updated standalone AAO PPP for HSV keratitis since 2014 - the 2014 document is still the reference
- No head-to-head RCT comparing ganciclovir gel vs aciclovir ointment at scale for dendritic ulcers (though ganciclovir is increasingly preferred based on tolerability)
- ZEDS primary endpoint was not significant - the 1 year suppressive valaciclovir recommendation is based on secondary endpoints and clinical judgment
- No approved antiviral to eradicate HSV latency - all current treatments are suppressive, not curative
- Optimal duration of suppression post-keratoplasty remains undefined by RCT (most expert centres: as long as on topical steroids + 1 additional year)
- Biomarkers for predicting recurrence risk (heparanase, MMPs) not yet validated for clinical use
- CRISPR/siRNA latency-targeting approaches are years from clinical application
give me the note of fungal corneal ulcer from basic to advanced level from the standard textbooks and add images to it, any clinical trials and recent advances. write it in chat and write about the viva questions that can be asked here
"fungal keratitis" AND treatment natamycin voriconazole