Carcinoma ESOPHAGUS mgt stage waise
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Excellent! I now have very comprehensive content. Let me compile the full stage-wise management answer.
Carcinoma Esophagus - Stage-wise Management
TNM Staging Overview (AJCC 8th Edition)
| Category | Description |
|---|---|
| Tis | High-grade dysplasia / intraepithelial neoplasm (M1) |
| T1a | Invades lamina propria / muscularis mucosae (M2-M3) |
| T1b | Invades submucosa (SM1-SM3) |
| T2 | Invades muscularis propria |
| T3 | Invades adventitia |
| T4a | Invades pleura, pericardium, azygos vein, diaphragm, peritoneum (resectable) |
| T4b | Invades aorta, vertebral body, trachea (unresectable) |
| Stage IV | Distant metastasis |
Staging Workup
Before deciding treatment, staging investigations must include:
- EUS (Endoscopic Ultrasound) - best for T and N staging. Sensitivity: T1 82%, T2 81%, T3 91%, T4 92%
- 18F-FDG PET-CT - detects distant metastases
- Contrast-enhanced CT chest + abdomen
- EMR for nodular T1a lesions (EUS often understages these)
For N staging by EUS: sensitivity 80%, specificity 70%; improves with EUS-guided FNA.
Stage-wise Management
Stage 0 (Tis - High Grade Dysplasia)
- Endoscopic Eradication Therapy (EET) is the treatment of choice - preferred over esophagectomy
- Includes Endoscopic Mucosal Resection (EMR) + Radiofrequency Ablation (RFA)
- Esophagectomy is an alternative but reserved for those who fail endoscopic therapy
Stage I (T1a, N0 - Intramucosal)
- Endoscopic eradication therapy is a reasonable alternative to surgery
- M2/M3 (T1a) tumors: EMR + RFA adequate
- If nodularity present on T1a lesion by EUS - EMR is recommended as EUS often misses submucosal invasion
Stage I (T1b, N0 - Submucosal)
- Lymph node metastases found in >10% of T1b cases occultly
- Esophagectomy is generally advised
- Role of neoadjuvant chemoradiation in Stage I is unclear
Stage II-III (T2-T4a, or N+, resectable)
- Neoadjuvant chemoradiation followed by esophagectomy is the preferred approach
- The landmark CROSS trial demonstrated improved survival with carboplatin + paclitaxel + 41.4 Gy radiation before surgery
- Perioperative chemotherapy + esophagectomy (for distal adenocarcinoma) is an acceptable alternative - based on MAGIC trial (epirubicin + cisplatin + 5-FU)
- Definitive chemoradiation (without surgery) acceptable for SCC or non-surgical candidates
Esophagectomy Options
| Approach | Details |
|---|---|
| Transhiatal (THE) | Laparotomy + left cervical incision; lower morbidity, higher leak rate |
| Transthoracic / Ivor-Lewis (TTE) | Laparotomy + right thoracotomy; better lymph node dissection; intrathoracic anastomosis |
| McKeown (3-field) | Thoracotomy + laparotomy + cervical; used for mid-esophageal or higher tumors |
| Minimally Invasive (MIE) | Laparoscopy + thoracoscopy; gaining popularity at specialized centers |
- High-volume centers have significantly lower esophagectomy mortality - patients should be referred accordingly
Post-esophagectomy Adjuvant Therapy
- Adjuvant nivolumab (anti-PD-1): CheckMate-577 trial showed significantly improved disease-free survival (22.4 months vs. 11 months) in patients with residual pathologic disease after neoadjuvant chemoradiation + esophagectomy
- Given as 240 mg every 2 weeks or 480 mg every 4 weeks for 1 year
Stage T4b / Stage IV (Unresectable / Metastatic)
- Palliative approach is the goal
- Chemotherapy regimens (same as gastric cancer, given molecular similarity via TCGA data):
- HER2+ tumors: Trastuzumab + cisplatin/oxaliplatin + fluoropyrimidine (ToGA trial - improved OS 13.8 vs. 11.1 months)
- HER2-negative: FOLFOX, cisplatin + 5-FU, XELOX
- Ramucirumab (anti-VEGFR2): 2nd-line, improved OS in REGARD trial (5.2 vs. 3.8 months); combined with paclitaxel in RAINBOW trial (9.6 months)
- Immunotherapy: Nivolumab + chemotherapy (CheckMate-649) and pembrolizumab approved in 1st-line metastatic disease
Special Case: Squamous Cell Carcinoma (SCC) vs Adenocarcinoma
| Feature | SCC | Adenocarcinoma |
|---|---|---|
| Location | Upper/mid esophagus | Lower esophagus/GEJ |
| Neoadjuvant preference | Definitive CRT (can avoid surgery) | Neoadjuvant CRT + surgery preferred |
| HER2 testing | Less relevant | Yes - test all metastatic cases |
| Siewert classification | N/A | Used for GEJ tumors to guide approach |
Palliative/Symptom Management (Advanced Disease)
- Esophageal stenting - for malignant dysphagia in non-surgical candidates
- Radiation for dysphagia palliation
- Brachytherapy as an alternative to external beam
Summary Algorithm
Diagnosis confirmed (EGD + biopsy)
↓
Staging: EUS + PET-CT + CT
↓
Tis / T1a N0 → Endoscopic therapy (EMR + RFA)
T1b N0 → Esophagectomy
T2+ or N+ → Neoadjuvant CRT → Esophagectomy → Adjuvant Nivolumab (if residual disease)
(or definitive CRT for SCC / unfit patients)
T4b / M1 → Palliative chemo ± targeted therapy ± immunotherapy ± stenting
Sources: Yamada's Textbook of Gastroenterology, 7th ed.; Sabiston Textbook of Surgery; Cummings Otolaryngology
Explain in details about stage 4
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, detailed content from multiple authoritative sources. Here is the full detailed breakdown of Stage 4 carcinoma esophagus management:
Stage IV Carcinoma Esophagus - Detailed Management
Stage IV disease includes:
- T4b (tumor invades aorta, vertebral body, trachea - unresectable)
- Any T, Any N, M1 (distant metastasis present)
The goal shifts entirely to palliation - improving quality of life and relieving symptoms. Surgery with curative intent is not offered.
Step 1: Mandatory Biomarker Testing (Before Any Systemic Therapy)
Every patient with Stage IV esophageal/GEJ cancer must undergo:
| Biomarker | Test Method | Purpose |
|---|---|---|
| HER2/ERBB2 | IHC, FISH, or NGS | Guides trastuzumab / T-DXd use |
| PD-L1 (CPS score) | IHC | Guides immunotherapy |
| MSI / dMMR | IHC / NGS | Guides pembrolizumab monotherapy |
| TMB (Tumor Mutational Burden) | NGS | High TMB → ICI benefit |
| NTRK gene fusion | NGS | Larotrectinib / entrectinib eligible |
| RET fusion | NGS | Selpercatinib eligible |
| BRAF V600E | NGS | Dabrafenib + trametinib eligible |
This molecular profiling is now standard of care for all metastatic esophageal cancers.
Step 2: Systemic Therapy - First-line
A. HER2-Positive Adenocarcinoma (~20-25% of cases)
Standard: Trastuzumab + Platinum-Fluoropyrimidine chemotherapy
- ToGA Trial: Trastuzumab + cisplatin + 5-FU/capecitabine
- Median OS: 13.8 months (vs. 11.1 months with chemo alone)
- Addition of Pembrolizumab (for progression-free survival improvement) in HER2+ disease is increasingly used
- Pertuzumab (anti-HER2) can be combined with trastuzumab
B. HER2-Negative Adenocarcinoma
Standard chemotherapy backbones:
- Cisplatin + 5-FU (CF) - classic first-line
- FOLFOX (Folinic acid + Oxaliplatin + 5-FU) - better tolerability
- XELOX / CAPOX (Oxaliplatin + Capecitabine) - noninferior to CF, oral convenience
- Adding Docetaxel (DCF/FLOT regimen) improves outcomes but higher toxicity
Plus immunotherapy based on PD-L1:
- If PD-L1 CPS ≥ 10: Add nivolumab or pembrolizumab to chemotherapy (CheckMate-649, KEYNOTE-590)
C. Squamous Cell Carcinoma (SCC)
ICIs show greater efficacy in SCC than adenocarcinoma:
- Nivolumab + chemotherapy or Nivolumab + Ipilimumab - first-line for advanced SCC
- Pembrolizumab + chemotherapy - approved first-line (KEYNOTE-590)
- PD-L1 CPS ≥ 10: higher benefit from immunotherapy
⚠️ Overall survival on chemotherapy in metastatic disease is generally < 12 months despite treatment.
Step 3: Second-line Systemic Therapy
| Indication | Agent | Trial |
|---|---|---|
| HER2+ after 1st line | Trastuzumab deruxtecan (T-DXd) - antibody-drug conjugate | Improved OS: 12.5 vs. 8.4 months |
| GEJ Adeno, chemo-refractory | Ramucirumab (anti-VEGFR2) alone | REGARD trial: OS 5.2 vs. 3.8 months |
| GEJ Adeno, chemo-refractory | Ramucirumab + Paclitaxel | RAINBOW trial: OS 9.6 months vs. placebo+paclitaxel |
| PD-L1+ or MSI-H, 2nd line | Pembrolizumab monotherapy | FDA approved |
| SCC, 2nd line | Nivolumab monotherapy | FDA approved |
Step 4: Rare/Niche Targeted Therapies
| Alteration | Drug |
|---|---|
| NTRK gene fusion | Larotrectinib / Entrectinib |
| RET fusion | Selpercatinib |
| BRAF V600E mutation | Dabrafenib + Trametinib |
| MSI-H / dMMR | Pembrolizumab monotherapy or Nivolumab + Ipilimumab |
Step 5: Palliation of Dysphagia (Critical in Stage IV)
Dysphagia (difficulty swallowing) is the cardinal symptom that profoundly impairs quality of life. Several modalities are available:
1. Self-Expanding Metal Stents (SEMS) - First-line for dysphagia
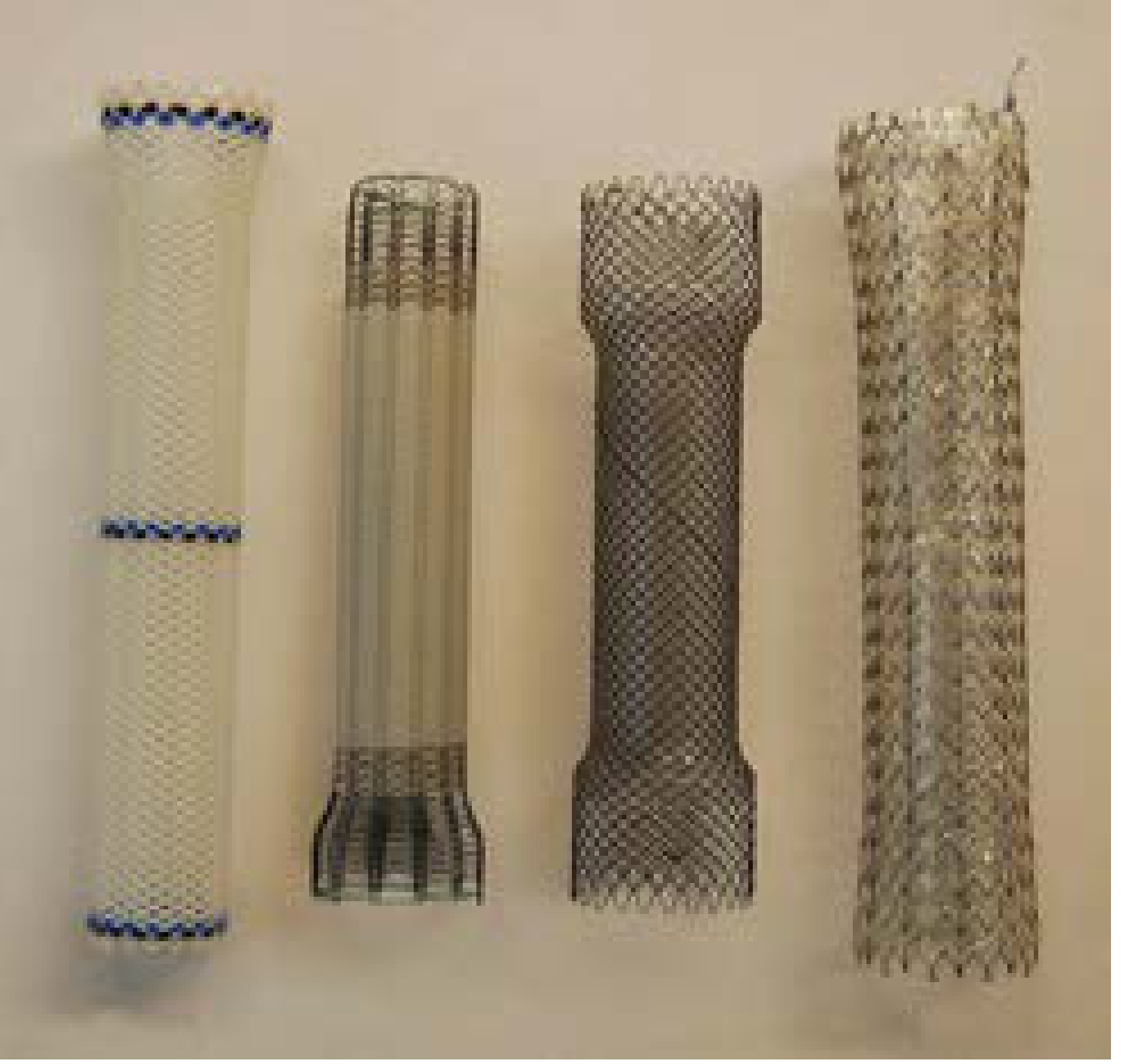
- Fully covered SEMS (fc-SEMS) are the stents of choice
- Lower tumor ingrowth vs uncovered SEMS
- Lower migration risk vs fully plastic stents
- Provides prompt, immediate dysphagia relief
- Indicated for moderate-to-severe dysphagia not amenable to other modalities
2. Brachytherapy
- Single-dose intraluminal brachytherapy provides longer-lasting dysphagia relief than stenting
- Higher QOL scores and fewer major complications (13% vs 25% for SEMS)
- However: frequent need for rescue stents - enthusiasm has declined
- Best for: patients with mild-moderate dysphagia and longer expected survival
3. External Beam Radiation Therapy (EBRT)
- Palliative radiation for pain, dysphagia, and bleeding
- Used when stenting is not feasible or as adjunct
4. Photodynamic Therapy (PDT)
- Endoluminal obstruction management
- Less commonly used but available in specialist centres
5. Endoscopic Laser Therapy (Nd:YAG)
- Ablates intraluminal tumor tissue
- Provides temporary dysphagia relief
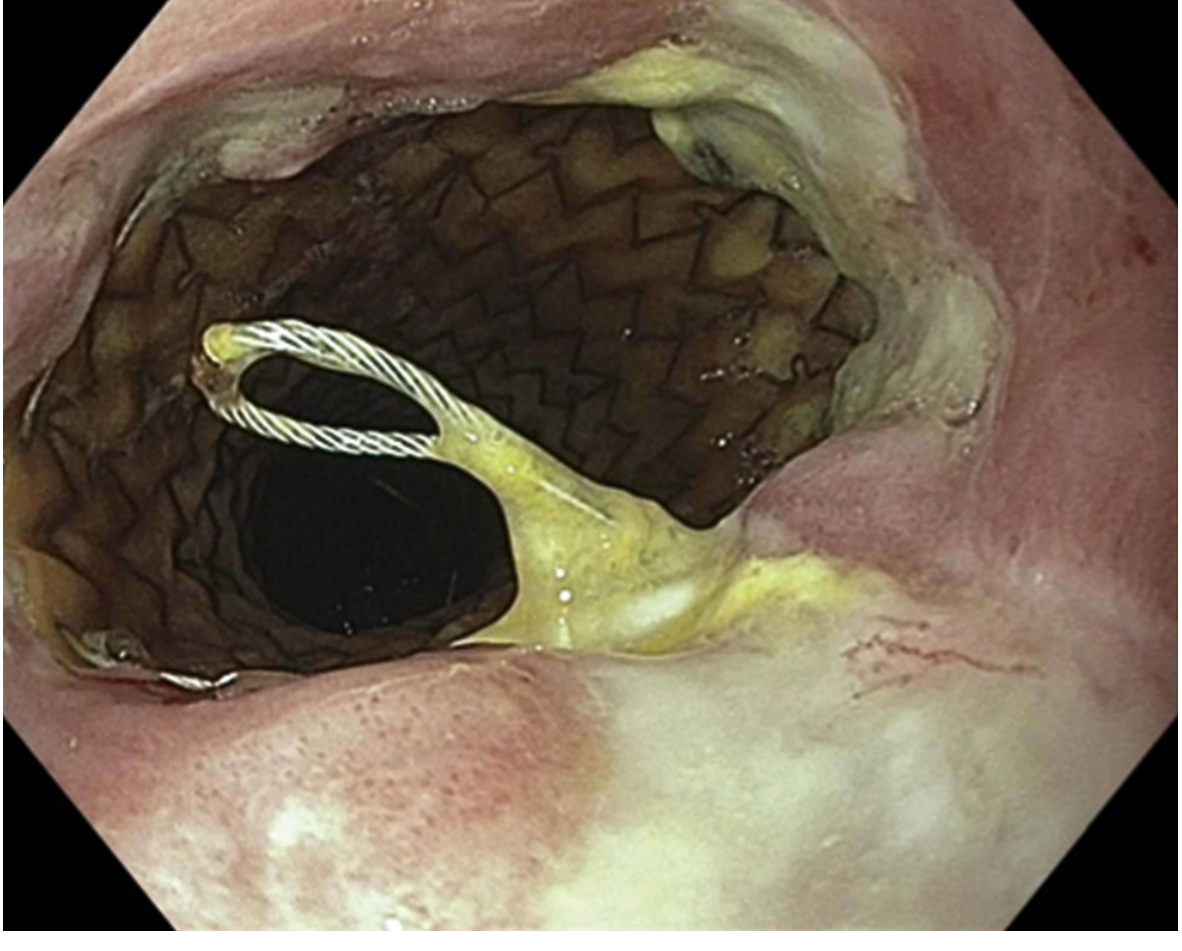
Step 6: Management of Malignant Tracheoesophageal Fistula (TEF)
TEF complicates ~5-10% of advanced esophageal cancers (T4b into trachea):
- Suspend oral intake immediately
- Drain involved spaces (pleura/mediastinum)
- Insert fully covered SEMS (fc-SEMS) - method of choice for sealing fistula
- Fistula closure rates >70% with fc-SEMS
- "Dual stenting" (esophageal + tracheal stent simultaneously) is largely avoided due to risk of lethal vascular erosions from synergistic pressure necrosis
- Amplatzer ASD occluder has been used off-label for closure in limited studies
Step 7: Nutritional Support
Malnutrition is near-universal in Stage IV esophageal cancer:
- Enteral feeding via nasojejunal tube - temporary
- Percutaneous Endoscopic Gastrostomy (PEG) - if no surgical resection planned
- Jejunostomy feeding tube - standard when gastrostomy is not feasible
- IV nutritional support as needed
Step 8: Best Supportive Care (BSC)
For patients with poor performance status (ECOG PS 3-4) or those who cannot tolerate systemic therapy:
- Pain management (WHO analgesic ladder; opioids for severe pain)
- Antiemetics, appetite stimulants
- Palliative sedation if refractory symptoms
- Hospice/end-of-life care coordination
- Multidisciplinary involvement: oncology, gastroenterology, palliative care, dietetics, psychology
Key point: BSC is always indicated in Stage IV regardless of whether active treatment is also given. It is not synonymous with "giving up" - it reduces suffering and can improve survival.
Prognosis
| Stage | 5-Year Survival |
|---|---|
| Local (T1-2, N0) | ~41% |
| Regional (N+) | ~23% |
| Distant (Stage IV) | ~5% |
| Overall (all stages) | ~19% |
- The most important prognostic factors are T stage (depth of invasion) and N stage (lymph node involvement)
- Histologic type, degree of differentiation, and tumor location also affect survival
Summary Flow for Stage IV
Stage IV confirmed (M1 or T4b)
↓
Full molecular profiling (HER2, PD-L1, MSI, TMB, NGS panel)
↓
Good PS (ECOG 0-1)?
YES → Systemic therapy:
HER2+ → Trastuzumab + chemo (± pembrolizumab)
HER2- → Chemo + anti-PD1 (if PD-L1+)
SCC → Nivolumab + chemo or nivolumab + ipilimumab
NO → Best supportive care alone
↓
Dysphagia present?
→ fc-SEMS first-line for moderate-severe
→ Brachytherapy for mild-moderate (longer survival expected)
↓
TEF present? → fc-SEMS + stop oral intake
↓
Malnutrition? → PEG / jejunostomy tube
↓
2nd-line on progression:
HER2+ → Trastuzumab deruxtecan (T-DXd)
Adeno → Ramucirumab ± paclitaxel
PD-L1+ → Pembrolizumab monotherapy
Sources: Sabiston Textbook of Surgery 21e; Harrison's Principles of Internal Medicine 22e (2025); Yamada's Textbook of Gastroenterology 7e; Sleisenger & Fordtran's GI Disease; Current Surgical Therapy 14e
In her2 Neu positive we can directly add pembrolizumab?
Finding Sources
Searching PubMed
HER2 positive esophageal gastroesophageal pembrolizumab trastuzumab first line
Reading Article
PMID: 37871604
Reading Article
PMID: 36603169
Reading File
Excellent - I have the definitive answer from the KEYNOTE-811 trial and the 2023 ASCO Guideline. Here is a precise, evidence-based answer:
HER2+ Esophageal/GEJ Cancer: Can You Add Pembrolizumab Directly?
Short answer: Yes - but NOT as pembrolizumab alone. It must be the triple combination: Pembrolizumab + Trastuzumab + Chemotherapy.
The KEYNOTE-811 Trial (Lancet, 2023) - The Key Evidence
This is the Phase 3 RCT that settled this question definitively.
| Parameter | Pembrolizumab arm | Placebo arm |
|---|---|---|
| Regimen | Pembro + Trastuzumab + Chemo | Placebo + Trastuzumab + Chemo |
| Median PFS | 10.0 months | 8.1 months (HR 0.72, p=0.0002) |
| Median OS | 20.0 months | 16.9 months |
| Population | HER2+ gastric or GEJ adenocarcinoma, 1st line |
- Pembrolizumab 200 mg IV every 3 weeks
- Combined with: trastuzumab + fluoropyrimidine (5-FU or capecitabine) + platinum (cisplatin or oxaliplatin)
- Up to 35 cycles
PFS benefit was statistically significant. OS showed a trend favoring pembrolizumab (HR 0.87) but did not cross the significance threshold at the second interim analysis - final OS data are still maturing.
2023 ASCO Guideline Recommendation (Level 1 Evidence)
The ASCO guideline (J Clin Oncol, 2023) explicitly states:
"For patients with HER2-positive gastric or GEJ previously untreated, unresectable or metastatic adenocarcinoma, trastuzumab plus pembrolizumab is recommended, in combination with chemotherapy."
This is now standard of care in the first-line metastatic setting.
Important Nuances You Must Know
1. PD-L1 requirement - does it matter here?
In HER2-negative patients, pembrolizumab requires CPS ≥ 10 to be added. But in HER2-positive patients, the KEYNOTE-811 trial enrolled regardless of PD-L1 status - so theoretically pembrolizumab is added even in PD-L1 low/negative HER2+ cases. In practice, PD-L1 CPS ≥ 1 patients showed the largest benefit.
2. The triple combination, not double
You cannot just give:
- Trastuzumab alone → not enough
- Pembrolizumab alone → not enough
- Trastuzumab + Pembrolizumab without chemo → not studied in this setting
The correct regimen is: Pembrolizumab + Trastuzumab + Fluoropyrimidine + Platinum
3. Chemotherapy backbone options
| Backbone | Details |
|---|---|
| Cisplatin + 5-FU | Classic; more nephrotoxicity |
| Oxaliplatin + Capecitabine (XELOX) | Oral, better tolerated |
| Oxaliplatin + 5-FU (FOLFOX) | IV, widely used |
4. This applies to GEJ and gastric - not pure SCC
- KEYNOTE-811 enrolled adenocarcinoma of gastric/GEJ origin
- For pure esophageal SCC, HER2 is rarely overexpressed and pembrolizumab/nivolumab are used differently (with chemo, without trastuzumab)
5. Second-line after HER2+ first-line
After progression on trastuzumab + pembrolizumab + chemo:
- Trastuzumab deruxtecan (T-DXd) is the standard 2nd-line (DESTINY-GastricO2/01 trials: OS 12.5 vs 8.4 months)
Summary Regimen for HER2+ Stage IV
HER2+ (IHC 3+ or IHC 2+/FISH amplified) Esophageal/GEJ Adeno
↓
1st Line: Pembrolizumab 200mg q3w
+ Trastuzumab 6mg/kg q3w (8mg/kg loading)
+ Platinum (cisplatin/oxaliplatin)
+ Fluoropyrimidine (5-FU/capecitabine)
↓ (progression)
2nd Line: Trastuzumab Deruxtecan (T-DXd)
Bottom line: You cannot add pembrolizumab alone to a HER2+ regimen. The evidence is specifically for the triple combination - pembrolizumab + trastuzumab + chemo together from the first line. This is now the ASCO-recommended standard of care.
Sources: KEYNOTE-811 Phase 3 RCT (Janjigian et al., Lancet 2023, PMID: 37871604); ASCO Guideline (Shah et al., J Clin Oncol 2023, PMID: 36603169); Harrison's Principles of Internal Medicine 22e (2025)
Role of this in stage 2/3 if residual disease Is present
Finding Sources
Searching PubMed
nivolumab adjuvant esophageal residual pathologic disease neoadjuvant chemoradiation
Reading File
Reading File
Reading File
I now have everything needed from multiple authoritative sources. Here is the complete, detailed answer:
Role of Immunotherapy (Nivolumab) in Stage II/III with Residual Disease - The CheckMate-577 Trial
Context: What is "Residual Disease" Here?
This refers to patients who:
- Had Stage II or III esophageal / GEJ cancer
- Received neoadjuvant chemoradiation (e.g. CROSS regimen: carboplatin + paclitaxel + 41.4 Gy)
- Underwent R0 esophagectomy (complete resection, clear margins)
- But on final pathology - still had residual viable tumor in the specimen
These patients did NOT achieve a pathological complete response (pCR). They are designated ypT+ or ypN+ (i.e., not ypT0N0M0). This group has a known high risk of recurrence and poor survival.
The CheckMate-577 Trial - Key Evidence
| Parameter | Details |
|---|---|
| Design | Phase III, randomized, double-blind, placebo-controlled |
| Population | Stage II/III esophageal cancer (SCC + Adenocarcinoma), post neoadjuvant CRT + R0 resection, residual pathologic disease |
| Intervention | Adjuvant Nivolumab 240 mg every 2 weeks OR 480 mg every 4 weeks |
| Duration | Up to 1 year (16 cycles at q2w dosing) |
| Primary endpoint | Disease-free survival (DFS) |
Results
| Outcome | Nivolumab | Placebo |
|---|---|---|
| Median DFS | 22.4 months | 11.0 months |
| Hazard Ratio | 0.69 (CI 0.56-0.86) | |
| Metastasis-free survival | Also significantly improved | |
| OS | Trend favoring nivolumab (mature data pending) |
The DFS benefit was doubled - from 11 months to 22.4 months. This was consistent across both SCC and adenocarcinoma histologies.
Why Nivolumab and NOT Pembrolizumab Here?
This is an important distinction to understand - the question asked about pembrolizumab:
| Drug | Setting | Trial |
|---|---|---|
| Nivolumab | Adjuvant after neoadjuvant CRT + R0 resection with residual disease (Stage II/III) | CheckMate-577 |
| Pembrolizumab | First-line metastatic HER2+ disease | KEYNOTE-811 |
So in Stage II/III with residual disease, the correct drug is nivolumab, not pembrolizumab. Pembrolizumab has not been studied in this specific adjuvant post-resection setting.
Who Exactly Qualifies - Strict Criteria
| Criteria | Required |
|---|---|
| Prior neoadjuvant chemoradiation | YES - must have received it |
| R0 resection completed | YES - negative margins required |
| Residual pathologic disease on specimen | YES - not ypT0N0M0 |
| Distant metastasis absent | YES - Stage II/III only |
| Histology | Both SCC and Adenocarcinoma |
| PD-L1 status required? | NO - benefit seen regardless of PD-L1 |
Key point: If the patient achieved a complete pathological response (ypT0N0M0), they do NOT receive adjuvant nivolumab. This drug is specifically for those with remaining disease.
What About Patients Who Had Perioperative Chemo (Not CRT)?
This is an important nuance:
- CheckMate-577 specifically enrolled patients after chemoRADIATION followed by surgery
- Patients who received perioperative chemotherapy alone (FLOT/MAGIC regimen) and have residual disease are not covered by this trial's indication
- For those patients, the adjuvant role of immunotherapy is being explored in trials like VESTIGE (EORTC 1707) - which randomized HER2- gastric/GEJ patients with ypN+ or R1 after perioperative chemo to adjuvant nivolumab + ipilimumab vs. chemo (PMID: 39542422, Ann Oncol 2025)
Ongoing Trials Exploring Neoadjuvant Immunotherapy (Future Landscape)
| Trial | Drug | Setting |
|---|---|---|
| MATTERHORN | Durvalumab + FLOT perioperatively | Gastric/GEJ adeno, neoadjuvant + adjuvant |
| CheckMate-648 | Nivolumab + chemo OR nivolumab + ipilimumab | Advanced esophageal SCC |
| Perioperative nivolumab + chemo (2025 Phase II) | Nivolumab + chemo | Locally advanced SCC, with ctDNA monitoring [PMID: 40375301] |
These trials may further shift management in Stage II/III toward incorporating immunotherapy even before surgery.
Current Standard of Care Summary for Stage II/III
Stage II/III esophageal / GEJ cancer
↓
Neoadjuvant CRT (CROSS: Carboplatin + Paclitaxel + 41.4 Gy)
↓
R0 Esophagectomy
↓
Pathology result?
↙ ↘
ypT0N0M0 Residual disease present
(pCR achieved) (ypT+ or ypN+)
↓ ↓
Surveillance ADJUVANT NIVOLUMAB
only 240mg q2w OR 480mg q4w
× 1 year (16 cycles)
→ Median DFS: 22.4 months
(vs 11 months without)
FDA Approval Status
Nivolumab is FDA approved specifically for:
Completely resected esophageal or GEJ cancer with residual pathologic disease who received neoadjuvant chemoradiation - based on CheckMate-577.
This approval covers both SCC and adenocarcinoma and does not require PD-L1 testing for eligibility.
Sources: Sabiston Textbook of Surgery 21e; Current Surgical Therapy 14e; Harrison's Principles of Internal Medicine 22e (2025); VESTIGE trial (PMID: 39542422, Ann Oncol 2025)
This is a shared conversation. Sign in to Orris to start your own chat.