*WEEKLY TEST QUESTION - 13/07/2026* *ANATOMY* * Bronchopulmonary segments *PHYSIOLOGY* * Neural regulation of respiration *BIOCHEMISTRY* * Cholestrol *BIOMECHANICS* * Explain the biomechanics of mandibular motions. *PSYCHOLOGY* * Define personality. Classify Personality. *SOCIOLOGY* * Define marriage. Explain types of marriage in detail.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Searching the Web
neural regulation of respiration respiratory centers medullary pontine physiology
Searching the Web
types of marriage sociology monogamy polygamy polyandry group marriage definition
Searching the Web
biomechanics of mandibular motions jaw movement hinge translation
Loading Image
Reading File
I now have comprehensive material across all six topics. Let me compile the complete weekly test answer.
📚 WEEKLY TEST ANSWERS — 13/07/2026
ANATOMY - Bronchopulmonary Segments
Definition
A bronchopulmonary segment is the area of lung supplied by a segmental (tertiary) bronchus and its accompanying branch of the pulmonary artery. Each segment is an independently functional unit - it is the smallest functionally independent region of a lung and the smallest area that can be isolated and surgically removed without affecting adjacent regions.
- Shape: Irregular cone, with the apex at the origin of the segmental bronchus and the base projected peripherally onto the lung surface
- Pulmonary veins run intersegmentally (between segments, not within them) - this is surgically important
Number of Segments
- 10 segments in the right lung
- 10 segments in the left lung (some fuse in the left lung, making it functionally 8-9)
Segments of the Right Lung (10)
| Lobe | Segment | Number |
|---|---|---|
| Superior (Upper) Lobe | Apical | S I |
| Posterior | S II | |
| Anterior | S III | |
| Middle Lobe | Lateral | S IV |
| Medial | S V | |
| Inferior (Lower) Lobe | Superior (Apical) | S VI |
| Medial basal | S VII | |
| Anterior basal | S VIII | |
| Lateral basal | S IX | |
| Posterior basal | S X |
Segments of the Left Lung (8-10)
| Lobe | Segment | Number |
|---|---|---|
| Superior (Upper) Lobe | Apicoposterior (fusion of S I + S II) | S I+II |
| Anterior | S III | |
| Superior lingular | S IV | |
| Inferior lingular | S V | |
| Inferior (Lower) Lobe | Superior (Apical) | S VI |
| Medial basal (often fused) | S VII | |
| Anterior basal | S VIII | |
| Lateral basal | S IX | |
| Posterior basal | S X |
Note: In the left lung, S I and S II fuse into the apicoposterior segment, and the lingular segments (S IV, S V) correspond to the right middle lobe. S VII (medial basal) is often absent or fused with S VIII on the left.
Bronchopulmonary Segments Diagram
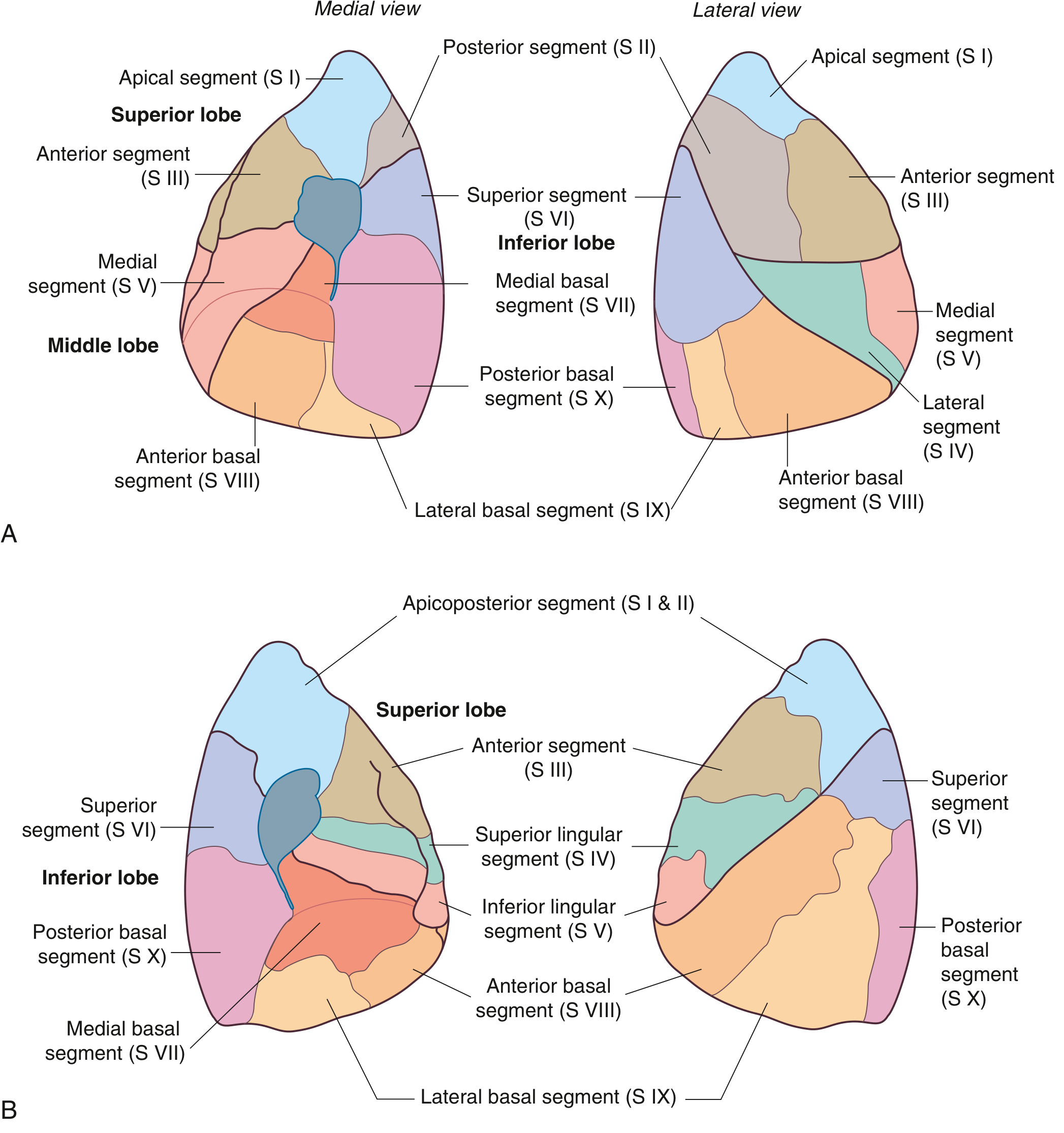
Fig. 3.49 - Bronchopulmonary segments of (A) right lung and (B) left lung, from medial and lateral views. - Gray's Anatomy for Students
Clinical Significance
- Bronchopulmonary segments are the basis for segmentectomy (surgical removal of individual segments)
- Postural drainage positions are designed to drain individual segments using gravity
- Knowledge of segments guides localization of abscesses, tumors, and collapse on imaging
PHYSIOLOGY - Neural Regulation of Respiration
Overview
Breathing is generated and regulated by specialized neurons in the brainstem - primarily the medulla oblongata and pons. These centers set the basic rhythm and adjust it based on metabolic demands, blood gases, and other inputs.
I. Respiratory Centers in the Brainstem
A. Medullary Respiratory Center (Medulla Oblongata)
The medulla contains the basic rhythm generator for breathing and is divided into two groups:
1. Dorsal Respiratory Group (DRG)
- Location: Nucleus tractus solitarius (NTS) in the dorsal medulla
- Function: Primarily drives inspiration
- Mechanism: Sends impulses via the phrenic nerve (C3-C5) to the diaphragm and via intercostal nerves to the external intercostal muscles
- During normal quiet breathing, the DRG fires for ~2 seconds (inspiration), then becomes inactive for ~3 seconds allowing passive expiration
- Receives afferent inputs from peripheral chemoreceptors (via CN IX, X) and lung stretch receptors
2. Ventral Respiratory Group (VRG)
- Location: Nucleus ambiguus and nucleus retroambigualis in ventral medulla
- Contains the pre-Bötzinger complex - believed to be the primary rhythm-generating kernel
- Function: Controls both inspiration AND expiration, especially during forced/active breathing
- Inactive during quiet breathing; activated when ventilatory demand increases (exercise, hyperventilation)
- Drives muscles of active expiration (internal intercostals, abdominals)
B. Pontine Respiratory Group (PRG) - Pons
1. Pneumotaxic Center (Dorsal/Rostral Pons)
- Location: Kölliker-Fuse nucleus + parabrachial complex (dorsolateral rostral pons)
- Function: Terminates inspiration (inspiratory "off-switch")
- Prevents over-inflation of lungs by sending inhibitory signals to the DRG
- Decreases tidal volume, increases respiratory rate
- When the pneumotaxic center is destroyed → prolonged deep inspirations (apneusis)
2. Apneustic Center (Caudal Pons)
- Function: Stimulates prolonged inspiration ("apneusis")
- Normally held in check by the pneumotaxic center
- Increases depth of breathing, increases tidal volume
- Inhibited by Hering-Breuer reflex (lung stretch receptors via vagus nerve)
II. Chemical Regulation of Respiration
Central Chemoreceptors
- Location: Ventral surface of medulla
- Sensitive to: Changes in CSF pH (indirectly reflecting PaCO₂)
- Rising CO₂ → CO₂ crosses BBB → H₂O + CO₂ → H₂CO₃ → H⁺ + HCO₃⁻ → ↓ CSF pH → stimulates ventilation
- CO₂ is the most powerful regulator of respiration under normal conditions
Peripheral Chemoreceptors
- Location: Carotid bodies (CN IX - Hering's nerve) and aortic bodies (CN X)
- Sensitive to: ↓ PaO₂ (hypoxia), ↑ PaCO₂, ↓ pH
- Hypoxic drive becomes significant when PaO₂ < 60 mmHg
- Primary drivers of ventilation in patients with chronic CO₂ retention (COPD)
III. Reflex Regulation
| Reflex | Receptor | Effect |
|---|---|---|
| Hering-Breuer Inflation Reflex | Pulmonary stretch receptors (slowly adapting) | Inhibits inspiration when lungs over-inflate; prevents over-inflation |
| Deflation Reflex | Stretch receptors | Stimulates inspiration when lungs deflate |
| Irritant Reflex | Rapidly adapting receptors (RAR) | Cough, bronchoconstriction, hyperpnea |
| J-receptor (Juxtacapillary) Reflex | J-receptors in alveolar walls | Rapid shallow breathing, apnea; activated by pulmonary congestion/edema |
IV. Higher Centers and Voluntary Control
- The cerebral cortex can override brainstem centers for voluntary breath-holding, speech, singing
- The limbic system modulates breathing during emotional states
- These inputs descend through the corticospinal tract (voluntary) and reticulospinal tracts (automatic)
BIOCHEMISTRY - Cholesterol
I. Structure
Cholesterol is a 27-carbon sterol with a characteristic 4-ring steroid nucleus (perhydrocyclopentanophenanthrene ring system). Key features:
- Ring A: cyclohexane (with 3β-OH group)
- Ring B: cyclohexane
- Ring C: cyclohexane
- Ring D: cyclopentane
- An 8-carbon side chain at C-17
- Double bond between C-5 and C-6 (making it a Δ⁵-sterol)
The 3β-hydroxyl group and double bond are critical for its biological activity.
II. Sources
- Dietary cholesterol (exogenous): ~300-500 mg/day - absorbed in small intestine; packaged into chylomicrons
- Endogenous synthesis: ~800-1000 mg/day - synthesized in nearly all cells, primarily the liver and intestine
- Occurs in the cytosol and smooth ER (SER)
- Starting material: Acetyl-CoA (from glucose, fatty acids, or amino acid catabolism)
III. Biosynthesis - Key Steps
All 27 carbons of cholesterol are derived from acetyl-CoA. The pathway occurs in several stages:
Stage 1: Formation of Mevalonate (Rate-Limiting Stage)
- 2 Acetyl-CoA → Acetoacetyl-CoA (thiolase)
- Acetoacetyl-CoA + Acetyl-CoA → HMG-CoA (HMG-CoA synthase) [cytosolic isoform]
- HMG-CoA → Mevalonate (HMG-CoA reductase) - RATE-LIMITING STEP
- Requires 2 NADPH; irreversible
- This is the target of statins (lovastatin, atorvastatin, etc.)
Stage 2: Mevalonate → Isopentenyl Pyrophosphate (IPP)
- Mevalonate → 5-phosphomevalonate → 5-pyrophosphomevalonate → IPP (5-carbon isoprene unit, requires ATP)
Stage 3: IPP → Squalene
- IPP ⇌ DMAPP (dimethylallyl-PP) [isomerase]
- IPP + DMAPP → GPP (geranyl-PP, 10C)
- GPP + IPP → FPP (farnesyl-PP, 15C)
- 2 FPP → Squalene (30C) [squalene synthase]
Stage 4: Squalene → Lanosterol → Cholesterol
- Squalene → Squalene-2,3-epoxide (squalene epoxidase, requires O₂ and NADPH)
- → Lanosterol (first sterol intermediate; cyclization)
- → Cholesterol (19 additional steps, ~20 enzymes)
IV. Regulation of HMG-CoA Reductase
The enzyme is regulated at multiple levels:
| Mechanism | Effect |
|---|---|
| SREBP-2 transcription factor (activated when SER cholesterol is low) | ↑ gene expression → ↑ synthesis |
| INSIG binding (when SER cholesterol is high) | Retains SCAP-SREBP complex in ER → ↓ transcription |
| Proteasomal degradation (sterol excess) | ↓ enzyme amount |
| AMPK phosphorylation (high AMP/low ATP) | Inactive form → ↓ activity |
| Insulin | Dephosphorylation → active form → ↑ synthesis |
| Glucagon/epinephrine | Phosphorylation → inactive form → ↓ synthesis |
V. Transport - Lipoproteins
| Lipoprotein | Density | Origin | Function | Key Apolipoprotein |
|---|---|---|---|---|
| Chylomicrons | Lowest | Intestine | Exogenous dietary TAG & cholesterol → periphery | Apo B-48 |
| VLDL | Very low | Liver | Endogenous TAG → periphery | Apo B-100 |
| IDL | Intermediate | VLDL remnant | Intermediate | Apo B-100, Apo E |
| LDL | Low | IDL | Cholesterol → peripheral tissues; "bad cholesterol" | Apo B-100 |
| HDL | High | Liver/intestine | Reverse cholesterol transport; "good cholesterol" | Apo A-I |
VI. Fates of Cholesterol
- Structural component of cell membranes (regulates fluidity)
- Precursor of bile acids/salts (chenodeoxycholic acid, cholic acid) - primary fate in liver; only route of cholesterol excretion
- Precursor of steroid hormones (glucocorticoids, mineralocorticoids, sex hormones)
- Precursor of vitamin D (7-dehydrocholesterol in skin → cholecalciferol by UV light)
- Cholesteryl esters formed for storage (via ACAT) and transport (via LCAT in plasma)
VII. Clinical Relevance
- Hypercholesterolemia: Risk factor for atherosclerosis and CAD - LDL oxidation → foam cell formation → atherosclerotic plaques
- Statins: Competitively inhibit HMG-CoA reductase → ↓ endogenous synthesis → upregulation of LDL receptors → ↓ plasma LDL
- Ezetimibe: Blocks intestinal NPC1L1 cholesterol transporter → ↓ absorption
- Familial hypercholesterolemia: Defective LDL receptor gene → very high LDL, premature CAD
BIOMECHANICS - Mandibular Motions
I. Introduction
The mandible is the only movable bone of the skull. Mandibular movements are enabled by the Temporomandibular Joint (TMJ) - a synovial, condylar, bilateral joint with an articular disc dividing it into two compartments. Mandibular kinematics involve 6 degrees of freedom and are unique in that two joints (right and left TMJ) must move simultaneously.
II. Basic Types of Movement
All mandibular movements are combinations of two fundamental mechanical movements:
A. Rotational Movement (Hinge Movement)
- Movement of the mandible around a fixed axis
- In the TMJ, occurs in the lower joint compartment (between condyle and disc)
- The only "pure" rotational movement is around the horizontal hinge axis during the initial phase of mouth opening
- The horizontal axis passes through both condylar heads - the "terminal hinge axis"
- Terminal hinge position = mandible rotates in CR (centric relation) without any translation; interincisal opening limited to ~20 mm
B. Translational Movement (Gliding)
- Movement in which every point of the object moves simultaneously in the same direction and at the same rate
- Occurs in the upper joint compartment (between disc and articular eminence of temporal bone)
- The condyle-disc complex glides anteriorly and inferiorly along the articular eminence
- Mandibular protrusion is the classic example of pure translation
- Pure translation does NOT naturally occur in isolation in the mandible
In practice, most mandibular movements are combinations of rotation and translation occurring simultaneously
III. Three Axes of Rotation
| Axis | Plane | Movement Description | Clinical Note |
|---|---|---|---|
| Horizontal (Hinge) Axis | Sagittal plane | Opening/closing; passes through both condyles | Only true "pure" rotation; terminal hinge position at ~20 mm opening |
| Vertical (Long) Axis | Horizontal plane | Lateral (side-to-side) movements; one condyle pivots while the other translates | Seen during chewing; "working side" vs "balancing side" |
| Sagittal (Frontal) Axis | Frontal plane | One condyle drops inferiorly while the other remains fixed | Does not occur naturally in isolation; always combined |
IV. Mandibular Movements and Border Movements
The envelope of motion describes the maximum range of mandibular movement in all directions. There are specific border movements in each plane:
A. Sagittal Plane Border Movements (Posselt's Envelope)
Traced by the mandibular incisor point:
- CR (Centric Relation) → hinge opening along terminal hinge arc (pure rotation, ~20 mm interincisal)
- Maximum opening - condyles at maximum forward and downward translation; ~40-60 mm interincisal in adults
- Maximum protrusion → maximum anterior translation
- Return to centric occlusion (CO/ICP)
B. Horizontal Plane Border Movements
- Maximum protrusion - both condyles translate forward equally
- Right and left lateral excursions - one condyle (working side) rotates; the other (balancing side/"Bennett movement side") translates medially
C. Frontal Plane Border Movements
- Show the lateral swing and vertical range of the mandible
V. Specific Functional Movements
| Movement | Description | Muscles Involved |
|---|---|---|
| Depression (Opening) | Combined rotation + translation; first ~20 mm is rotation in CR, then translation | Lateral pterygoid (inferior head), digastric, geniohyoid, mylohyoid |
| Elevation (Closing) | Reverse sequence - translation then rotation | Masseter, medial pterygoid, temporalis |
| Protrusion | Both condyles translate anteriorly; mandible moves forward | Lateral pterygoid (both heads), medial pterygoid |
| Retrusion | Condyles move posteriorly back to CR | Posterior fibers of temporalis, digastric |
| Lateral excursion | Working-side condyle rotates; non-working condyle moves forward, down and medially (Bennett movement) | Ipsilateral temporalis + contralateral pterygoids |
| Chewing (Mastication) | Complex cycle: opening → lateral → closing → medial crossing | All muscles of mastication in coordinated sequence |
VI. Bennett Movement
- The movement of the non-working (balancing) condyle during lateral excursion
- It translates anteriorly, inferiorly, and medially
- The Bennett angle = angle between the sagittal plane and the path of the moving condyle
- Important in occlusal adjustment and prosthetic design
VII. Centric Relation vs Centric Occlusion
- Centric Relation (CR): The position where the condylar heads are in their most superior, anterior position in the glenoid fossa - a bone-to-bone reference; reproducible
- Centric Occlusion (CO) / Intercuspal Position (ICP): Maximum intercuspation of teeth regardless of condylar position
- The discrepancy between CR and CO is called the "long centric" or CR-CO slide
PSYCHOLOGY - Personality
I. Definition
Personality is a complex, multidimensional psychological concept. The most widely cited definition is by Gordon Allport:
"Personality is the dynamic organization within the individual of those psychophysical systems that determine his/her unique adjustment to his/her environment."
Breaking down this definition (as per Kaplan & Sadock's Comprehensive Textbook of Psychiatry):
- "Dynamic organization" - personality is an organized, constantly evolving system ("unitas multiplex")
- "Within the individual" - refers to intrapsychic processes, not comparisons between persons
- "Psychophysical" - neither exclusively mental nor exclusively neural, but a combination of both
- "Unique adjustment to environment" - each individual has a unique mode of adaptation and survival
- "Determine" - personality traits are determining dispositions that limit behavioral repertoire
Updated/Modified Definition: Human personality is the dynamic organization of the biopsychosocial systems by which a person shapes and adapts in a unique way to a changing internal and external environment - emphasizing self-awareness, plasticity, and proactive planning.
II. Key Characteristics of Personality
- Consistent - relatively stable across situations and time
- Distinctive - unique to each individual
- Dynamic - evolves through interaction of heredity and environment
- Predictive - allows prediction of behavior in new situations
III. Determinants of Personality
- Genetic: ~30-50% of variance in personality traits is heritable (higher in twin studies due to epistasis)
- Environment: Unique environmental experiences (non-shared), parental rearing, sociocultural norms
- Epigenetics: Gene-environment interaction shapes personality over the lifespan
- Self-awareness: Humans can deliberately modify behavioral patterns (Flynn effect analog for personality)
IV. Classification of Personality
A. Allport's Classification (Trait Theory)
Based on the prevalence and influence of traits:
| Type | Description | Example |
|---|---|---|
| Cardinal traits | Single dominant trait that defines the person | Gandhi's nonviolence; Hitler's cruelty |
| Central traits | 5-10 key traits that characterize an individual | Honesty, kindness, shyness |
| Secondary traits | Less consistent, situational traits | Nervous in public speaking only |
B. Type Theory (Historical)
Hippocratic/Galenic Humoral Types (based on body humors):
| Humor | Type | Characteristics |
|---|---|---|
| Blood | Sanguine | Optimistic, social, cheerful, energetic |
| Yellow bile | Choleric | Ambitious, leader, irritable, aggressive |
| Black bile | Melancholic | Analytical, perfectionist, sad, anxious |
| Phlegm | Phlegmatic | Calm, relaxed, consistent, unexpressive |
Sheldon's Somatotype Theory (body build and personality):
| Somatotype | Body Type | Personality |
|---|---|---|
| Endomorph | Soft, round, fat | Viscerotonic - sociable, relaxed, comfort-loving |
| Mesomorph | Muscular, athletic | Somatotonic - assertive, adventurous, energetic |
| Ectomorph | Thin, lean | Cerebrotonic - introverted, anxious, restrained |
Kretschmer's Types (psychiatric correlation):
| Body Type | Psychiatric Correlation |
|---|---|
| Pyknic (short, rounded) | Cyclothymic/manic-depressive |
| Asthenic/Leptosomic (thin, narrow) | Schizothymic/schizophrenia |
| Athletic (muscular) | Epileptoid |
| Dysplastic (mixed/abnormal) | Mixed |
C. Eysenck's Dimensional Model (PEN Model)
Three major dimensions:
- Extraversion-Introversion (E): Outward vs. inward orientation
- Neuroticism-Stability (N): Emotional instability vs. stability
- Psychoticism (P): Tough-mindedness, antisocial tendencies
Combining E and N produces four temperament quadrants closely paralleling Galenic types.
D. The Big Five (Five-Factor Model / OCEAN)
The most widely researched modern model:
| Factor | Description |
|---|---|
| O - Openness | Curiosity, creativity, willingness to try new things |
| C - Conscientiousness | Organization, dependability, self-discipline |
| E - Extraversion | Sociability, assertiveness, positive emotions |
| A - Agreeableness | Cooperation, trust, empathy |
| N - Neuroticism | Emotional instability, anxiety, moodiness |
E. DSM-5 Personality Disorders Classification
Organized into three Clusters:
| Cluster | Descriptor | Disorders |
|---|---|---|
| Cluster A | "Odd/Eccentric" | Paranoid, Schizoid, Schizotypal |
| Cluster B | "Dramatic/Emotional" | Antisocial, Borderline, Histrionic, Narcissistic |
| Cluster C | "Anxious/Fearful" | Avoidant, Dependent, Obsessive-Compulsive |
SOCIOLOGY - Marriage
I. Definition
Marriage is a socially and often legally recognized union between individuals that establishes rights and obligations between them, their children, and their in-laws.
Sociological definitions:
- Marriage is a sacred social institution that establishes the family unit, legitimizes reproduction, and regulates sexual behavior within a defined social framework
- It creates roles, responsibilities, economic arrangements, and kinship ties between partners and their respective families
- As per Park's Textbook of Preventive and Social Medicine: "Marriage is a sacred institution. It is the usual social custom... Monogamy is the most universal form of marriage."
Marriage is universal - found in every known human society, though its forms vary greatly across cultures.
II. Functions of Marriage
- Regulation of sexual behavior - defines socially acceptable sexual partners
- Procreation and legitimacy - provides legitimate status to children
- Socialization of children - establishes who is responsible for child-rearing
- Economic cooperation - division of labor, pooling of resources
- Emotional support - companionship and psychological security
- Status assignment - confers social roles and rank
III. Types of Marriage
A. On the Basis of Number of Spouses
1. Monogamy
- One man married to one woman at a time
- Most universal and legally recognized form worldwide
- Two subtypes:
- Straight monogamy: One spouse for life (no remarriage after death/divorce)
- Serial (Sequential) monogamy: Multiple marriages over a lifetime, but only one spouse at a time (after divorce or death of spouse) - common in Western societies
2. Polygamy (marriage to multiple spouses simultaneously)
Polygamy has three major forms:
a. Polygyny (most common form of polygamy)
- One man married to multiple women simultaneously
- Practiced in parts of Africa, the Middle East, some South Asian communities, and certain religious groups (historically Mormons)
- Two subtypes:
- Sororal polygyny: Co-wives are biological sisters (e.g., among Todas of India)
- Non-sororal polygyny: Co-wives are unrelated women
- Practiced for cultural, economic (larger labor force), religious, or political reasons (alliances)
- Legal in approximately 58 countries
b. Polyandry
- One woman married to multiple husbands simultaneously
- Rarest form of marriage; found primarily in:
- Himalayan regions: Toda tribe (Nilgiris, India), Khasas of Jaunsar-Bawar (India), Tibetan and Nepali communities
- Common reason: fraternal brothers sharing a wife to prevent land fragmentation
- Two subtypes:
- Fraternal (Adelphic) polyandry: Husbands are brothers (most common form)
- Non-fraternal polyandry: Husbands are unrelated men
- More common in societies with resource scarcity, male-skewed sex ratios, or high male mortality
c. Group Marriage (Cenogamy)
- Multiple men married to multiple women simultaneously - all partners are considered married to each other
- Extremely rare; not customary in any known society as a dominant practice
- Considered a theoretical/borderline category in sociology
B. On the Basis of Social Rules
3. Endogamy
- Marriage within a defined social group (caste, clan, tribe, religion, village)
- Rules mandate marrying within one's own group
- Examples: caste endogamy in India (must marry within one's varna/jati)
- Preserves group identity, cultural practices, and property within the group
4. Exogamy
- Marriage outside one's own group (clan, gotra, totem group)
- Rules prohibit marriage within the group; must marry outside
- Examples: Gotra exogamy in Hindus (cannot marry within same gotra); clan exogamy in tribal societies
- Prevents inbreeding; establishes alliances between different groups
- Most societies practice clan exogamy combined with caste endogamy simultaneously
5. Cross-Cousin Marriage
- Marriage between children of a brother and a sister (permitted or preferred in many South Indian, Dravidian communities)
- Common in Tamil Nadu, Andhra Pradesh, Karnataka
6. Parallel Cousin Marriage
- Marriage between children of two brothers or two sisters
- Common in Arab/Middle Eastern cultures
C. On the Basis of Economic Transactions
7. Arranged Marriage
- Families (parents, elders) select partners for young people
- Historically dominant globally; still very common in South Asia, Middle East, Africa
- Ranges from fully arranged (no choice for individuals) to semi-arranged (family suggests, individuals consent)
8. Love Marriage / Self-Selection
- Individuals choose their own partners based on mutual attraction and consent
- Dominant in Western societies; increasingly common globally
9. Dowry System (Dahej)
- Bride's family transfers property/wealth to groom/groom's family
- Practiced in India (illegal under Dowry Prohibition Act 1961, but persists)
10. Bride Price (Bridewealth)
- Groom's family pays the bride's family (opposite of dowry)
- Common in sub-Saharan Africa
D. Other Types
11. Levirate Marriage
- A widow marries her dead husband's brother
- Found in the Old Testament (Jewish law); some African and South Asian societies
- Ensures continued support for the widow and children
12. Sororate Marriage
- A widower marries his dead wife's sister
- Ensures children are raised by a close relative of their mother
13. Child Marriage
- Marriage before the age of 18 (girls) or 21 (boys)
- Prohibited in India (Child Marriage Restraint Act 1978; PCMA 2006)
- Legal minimum age in India: 18 for girls, 21 for boys
- Gradually declining; national average for effective age at marriage in India was 22.3 years (2016)
IV. Summary Table
| Type | Spouses | Key Feature |
|---|---|---|
| Monogamy | 1+1 | Most universal; one spouse at a time |
| Serial monogamy | 1+1 (sequentially) | Multiple marriages but one at a time |
| Polygyny | 1 man + multiple women | Most common polygamy form |
| Polyandry | 1 woman + multiple men | Rarest; mainly fraternal |
| Group marriage | Multiple men + multiple women | Theoretical; extremely rare |
| Endogamy | Within group | Preserves group identity |
| Exogamy | Outside group | Prevents inbreeding; creates alliances |
Sources: Gray's Anatomy for Students; Lippincott's Illustrated Reviews: Biochemistry 8th ed.; Kaplan & Sadock's Comprehensive Textbook of Psychiatry; Park's Textbook of Preventive and Social Medicine; JoVE Core Anatomy & Physiology; Frontiers in Neural Circuits (PMC5368202); Pocket Dentistry - Mechanics of Mandibular Movement
This is a shared conversation. Sign in to Orris to start your own chat.