Correlate development ot tongue with its nerve supply
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
I now have everything needed for a thorough answer. Let me compile it.
Development of the Tongue and Correlation with Its Nerve Supply
The nerve supply of the tongue is a direct reflection of its embryological origin from four pharyngeal arches. Each region of the adult tongue carries the nerve of the arch from which it was derived - this is the key principle of the correlation.
1. Embryological Development
Week 4 - First Swellings Appear
Near the end of the 4th week, in the floor of the primordial pharynx (just rostral to the foramen cecum), three swellings arise from proliferating mesenchyme of the 1st pharyngeal arch:
- Median lingual swelling (tuberculum impar) - a midline triangular elevation
- Two lateral lingual swellings (distal tongue buds) - one on each side
The lateral lingual swellings rapidly enlarge, merge with each other, and overgrow the median lingual swelling. The fused lateral swellings form the anterior 2/3 (oral part) of the tongue. The median lingual swelling does not form a recognizable part of the adult tongue. The fusion site is marked externally by the midline groove and internally by the fibrous lingual septum.
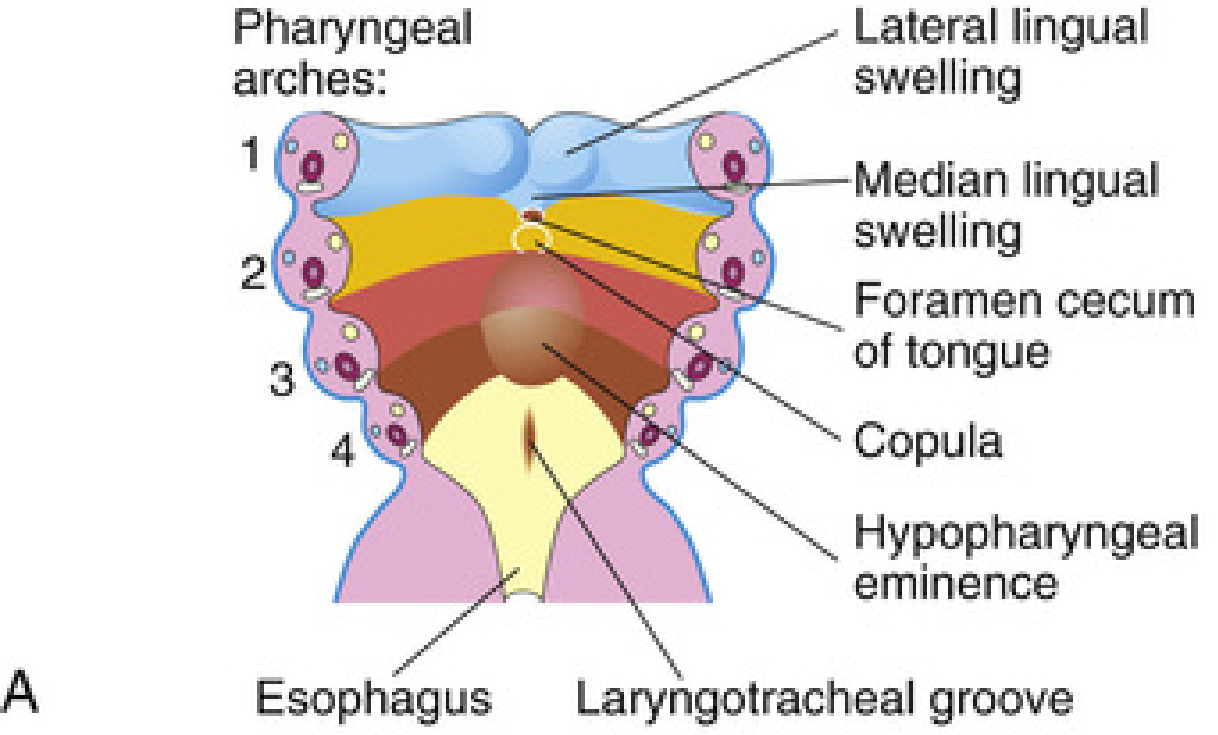
Posterior Third - 2nd, 3rd, and 4th Arch Contributions
Two midline elevations develop caudal to the foramen cecum:
- Copula - formed by fusion of ventromedial parts of the 2nd pharyngeal arch
- Hypopharyngeal eminence - develops caudal to the copula from mesenchyme of the 3rd and 4th pharyngeal arches
Critically, the copula is progressively overgrown by the hypopharyngeal eminence and disappears. As a result, the 2nd arch contributes nothing to the adult tongue mucosa - a fact that directly explains why CN VII (the 2nd arch nerve) does not supply tongue mucosa in general.
The posterior 1/3 (pharyngeal part) is formed from the rostral part of the hypopharyngeal eminence (3rd + 4th arches).
The boundary between anterior 2/3 and posterior 1/3 is marked by the V-shaped terminal sulcus, with the foramen cecum at its apex.
Muscles of the Tongue
Most tongue muscles are derived from myoblasts that migrate from the 2nd-5th occipital myotomes (not from pharyngeal arch mesenchyme). The hypoglossal nerve (CN XII) accompanies these myoblasts during migration and innervates the tongue muscles as they develop. Neural crest cells also migrate into the developing tongue, giving rise to its connective tissue and vasculature.
2. Nerve Supply - Development Correlation (The Core of the Question)
| Pharyngeal Arch | Arch Nerve | Embryological Contribution | Adult Nerve Supply |
|---|---|---|---|
| 1st arch | CN V3 (mandibular nerve) | Median + lateral lingual swellings → anterior 2/3 mucosa | Lingual nerve (CN V3) - general sensation, anterior 2/3 |
| 2nd arch | CN VII (facial nerve) | Copula - overgrown, disappears | Chorda tympani (CN VII) - taste only, anterior 2/3 (no mucosal territory) |
| 3rd arch | CN IX (glossopharyngeal) | Hypopharyngeal eminence (dominant) → posterior 1/3 | CN IX - general sensation + taste, posterior 1/3; also vallate papillae |
| 4th arch | CN X (vagus - superior laryngeal branch) | Small posterior contribution | CN X - small area anterior to epiglottis |
| Occipital myotomes | CN XII (hypoglossal) | All tongue musculature (not arch-derived) | CN XII - all intrinsic and extrinsic muscles |
3. Detailed Nerve Supply Analysis
Anterior 2/3 (Oral Part)
- General sensation (touch, pain, temperature): Lingual nerve, a branch of CN V3 - because this region developed from 1st arch swellings, and CN V3 is the nerve of the 1st arch.
- Taste: Chorda tympani (branch of CN VII, the 2nd arch nerve). This is an apparent exception - CN VII is the 2nd arch nerve, yet it supplies taste in the 1st arch territory. The explanation: the chorda tympani grows out and establishes contact with the developing taste buds in the anterior 2/3 before the copula is overgrown, securing a taste territory even though the 2nd arch loses its mucosal territory. The fungiform papillae develop near terminations of the chorda tympani.
- Vallate (circumvallate) papillae: Innervated by CN IX (glossopharyngeal), despite lying in the anterior part of the tongue. The usual explanation is that 3rd arch mucosa is pulled slightly anteriorly as the tongue develops, dragging 3rd arch innervation with it.
Posterior 1/3 (Pharyngeal Part)
- General sensation + taste: Glossopharyngeal nerve (CN IX) - this region developed from the 3rd arch component of the hypopharyngeal eminence.
- The vallate and foliate papillae appear first embryologically, close to terminal branches of CN IX.
Most posterior region (anterior to epiglottis)
- Small area supplied by internal laryngeal branch of superior laryngeal nerve (CN X) - reflecting 4th arch contribution.
All Muscles
- Hypoglossal nerve (CN XII) supplies all intrinsic and extrinsic muscles, except palatoglossus, which is supplied by the vagus nerve (CN X) via the pharyngeal plexus (the palatoglossus develops from pharyngeal arch mesenchyme rather than occipital myotomes).
4. Why CN VII is an Exception
The 2nd pharyngeal arch nerve is CN VII, yet CN VII does not supply general sensation to any part of the tongue mucosa. This is because:
- The 2nd arch derivative (copula) is completely overgrown by the 3rd arch hypopharyngeal eminence and leaves no mucosal territory.
- However, the chorda tympani branch of CN VII still provides taste to the anterior 2/3 - it established this connection before the copula disappeared.
This is one of the most tested points in anatomy - the 2nd arch nerve has taste but no touch territory on the tongue.
5. Lingual Papillae Development - Timeline
| Papilla Type | Appears | Nerve Relationship |
|---|---|---|
| Vallate + foliate | ~End of 8th week | Near CN IX terminal branches |
| Fungiform | Later in 8th week | Near chorda tympani (CN VII) terminations |
| Filiform | 10-11 weeks | Touch afferents (CN V3) |
| Taste buds | 11-13 weeks | Develop by inductive interaction with chorda tympani, CN IX, and CN X fibers |
Summary Mnemonic
"1V, 2 taste only, 3 back, 4 epiglottis, 12 muscles"
- 1st arch / CN V3 = anterior 2/3 general sensation
- 2nd arch / CN VII (chorda tympani) = taste only, anterior 2/3
- 3rd arch / CN IX = posterior 1/3 + vallate papillae
- 4th arch / CN X = small area near epiglottis
- Occipital myotomes / CN XII = all muscles (except palatoglossus via CN X)
Source: The Developing Human: Clinically Oriented Embryology, pp. 501-505
Specity development or thyrola
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I have all the content needed. Here is the full, structured answer.
Development of the Thyroid Gland
The thyroid gland is the first endocrine gland to develop in the embryo. Its development involves both a median component (from the floor of the pharynx) and two lateral components (from the 4th pharyngeal pouch).
1. Origin and First Appearance
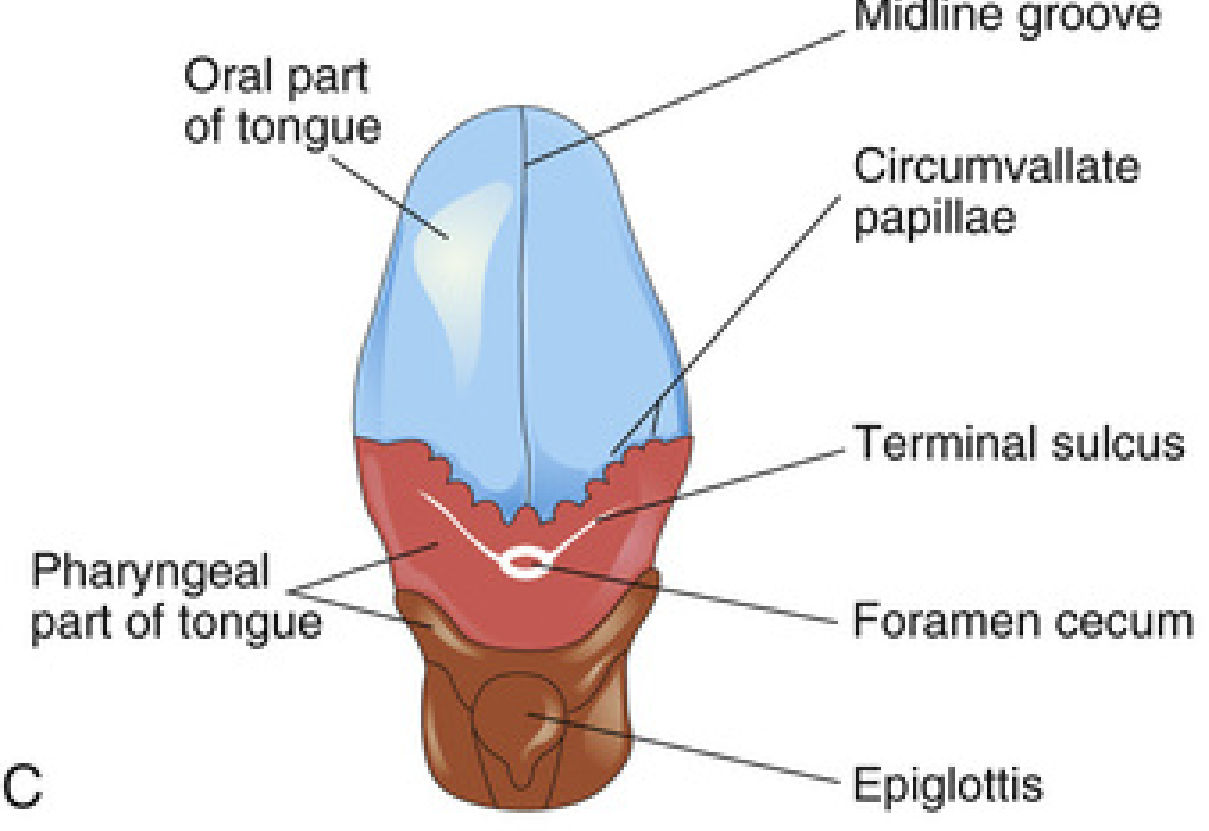
- Begins approximately day 24 after fertilization (end of week 3/beginning of week 4)
- Arises from a median endodermal thickening in the floor of the primordial pharynx, at the point that will become the foramen cecum (the junction between the anterior 2/3 and posterior 1/3 of the tongue)
- This thickening soon forms a small outpouching - the thyroid primordium (median anlage)
- Development is regulated by the Notch and Hedgehog signaling pathways
- Key transcription factors involved: TTF1, FOXE1, PAX8, TSHR, DUOX2
2. Descent of the Thyroid
As the embryo and tongue grow, the thyroid primordium descends in the neck, passing ventral to the developing hyoid bone and then ventral to the laryngeal cartilages.
During descent, the gland remains connected to the tongue by a narrow hollow tube called the thyroglossal duct.
3. Lateral Components (Ultimopharyngeal Bodies)
Two lateral thyroid primordia arise from the 4th pharyngeal pouch (ultimopharyngeal bodies / lateral anlage) and fuse with the midline primordium:
- The lateral components primarily provide the parafollicular (C) cell population - which secrete calcitonin
- The midline (median) component provides the majority of follicular cells - which produce T3/T4
4. Final Shape and Position
- By 7 weeks, the gland has assumed its definitive shape and reached its final position in the neck
- It divides into right and left lobes connected by the isthmus, which lies anterior to the 2nd and 3rd tracheal rings
- The thyroglossal duct degenerates by week 7; its proximal opening persists as the foramen cecum on the dorsum of the tongue
- A pyramidal lobe extends superiorly from the isthmus in ~50% of people - it represents a persistent portion of the inferior end of the thyroglossal duct that has formed thyroid tissue
5. Histogenesis (Structural Maturation)
| Stage | Event |
|---|---|
| Initially | Solid mass of endodermal cells |
| Invaded by vascular mesenchyme | Breaks into a network of epithelial cords |
| Week 10 | Cords divide into small cell clusters; a lumen forms in each - these become thyroid follicles |
| Week 11 | Colloid appears in follicles; iodine concentration and thyroid hormone synthesis begin |
| Week 11 | Thyroxine detectable in fetal serum |
| Week 16 | TSH becomes the principal regulator of hormone biosynthesis |
| Week 17.5 | Structural maturity of the thyroid achieved |
| Week 20 | Fetal TSH and thyroxine levels begin to increase |
| Week 24 | T3 detectable |
| Week 35 | TSH and thyroxine reach adult levels |
| Birth | Gland weighs ~1.5 g |
Note: Thyroid hormone is required by the fetal brain as early as the first trimester, before the fetal thyroid is functional - it is provided entirely by the mother until the fetal gland begins working at week 11. The NIS (sodium-iodine symporter) plays a key role in onset of thyroid functioning.
6. Developmental Timeline Summary
| Time | Event |
|---|---|
| Day 10 | Endodermal thickening seen |
| Day 16-17 | Median and lateral anlage discernible |
| Day 24 | Median anlage forms flask-like diverticulum from floor of buccal cavity |
| Day 30 | Bi-lobulated structure forms |
| Day 40 | Median and lateral anlage fuse; thyroglossal duct begins degenerating into fibrous stalk |
| Day 50 | Lateral expansion; descent complete; precolloid phase starts |
| Day 60 | Definite shape; follicle formation; thyroglobulin expression begins |
| Week 10 | Colloid phase; thyroglossal stalk disappears |
| Week 11 | Histogenesis virtually complete; T4 detectable in serum |
| Week 17.5 | Structural maturity |
7. Congenital Anomalies (Due to Developmental Errors)
| Anomaly | Mechanism |
|---|---|
| Thyroglossal duct cyst | Failure of the thyroglossal duct to degenerate; most common at/below the hyoid bone; presents as a painless, midline, movable swelling that moves with swallowing and tongue protrusion |
| Thyroglossal duct sinus | Perforation of an infected cyst; opens in the midline of the neck, anterior to laryngeal cartilages |
| Lingual thyroid | Failure of the thyroid to descend; gland remains at the base of the tongue near the foramen cecum; may be the only functioning thyroid tissue |
| Ectopic thyroid | Thyroid tissue along any point on the descent path (sublingual, suprahyoid, infrahyoid, intrathoracic) |
| Thyroid hemiagenesis | Failure of one lobe to form; left lobe more commonly absent |
| Agenesis | Complete absence of thyroid - mutations in TSH receptor genes |
| Congenital hypothyroidism | Most common metabolic disorder in neonates; may result from mutations in TTF1, TTF2, PAX8, or TSH receptor genes; causes neurodevelopmental disorders if untreated |
Key Points to Remember
- Thyroid is the first endocrine gland to develop
- Starts at day 24 from the floor of the pharynx (future foramen cecum)
- Descends connected to tongue via thyroglossal duct - duct normally disappears by week 7
- Median anlage → follicular cells (T3/T4); Lateral anlage (4th pouch) → parafollicular C cells (calcitonin)
- Colloid appears and thyroid hormone synthesis begins at week 11
- Pyramidal lobe = remnant of inferior thyroglossal duct, present in ~50%
- Foramen cecum = permanent marker of thyroid's original site of origin on the tongue
Sources: The Developing Human: Clinically Oriented Embryology, pp. 491-499; Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Chapter 53
What is clett palate. List its types with their embryological basıs
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have all the content needed. Here is the complete answer.
Cleft Palate - Definition, Types, and Embryological Basis
What is Cleft Palate?
A cleft palate is a congenital malformation in which the palatine shelves (lateral palatine processes) fail to fuse with each other, with the primary palate, and/or with the nasal septum during embryonic development. The result is a persistent opening in the roof of the mouth, which may range from a notched uvula to a complete split of the entire palate communicating with the nasal cavity.
- Frequency: approximately 1 in 2500 births
- More common in girls (unlike cleft lip, which is more common in boys)
- May occur alone or in combination with cleft lip
The incisive fossa (located behind the incisor teeth) is the key embryological landmark used to classify all palate clefts, because it marks the boundary between the primary palate (anterior) and the secondary palate (posterior).
Normal Palate Development (Brief Overview)
Understanding cleft palate types requires knowing how the palate forms normally:
- Primary palate (premaxilla/anterior palate): Develops from the median palatine process of the frontonasal prominence, forms the triangular wedge of hard palate anterior to the incisive fossa and carries the 4 upper incisor teeth. Forms at week 6.
- Secondary palate (posterior palate): Develops from two lateral palatine processes (palatal shelves) that grow medially from the maxillary prominences. Initially they project downward on either side of the tongue, then at week 7-8 they elevate to a horizontal position and fuse with each other in the midline, with the primary palate anteriorly, and with the nasal septum above. This fusion proceeds anteriorly to posteriorly, completing by week 10-12.
Types of Cleft Palate with Embryological Basis
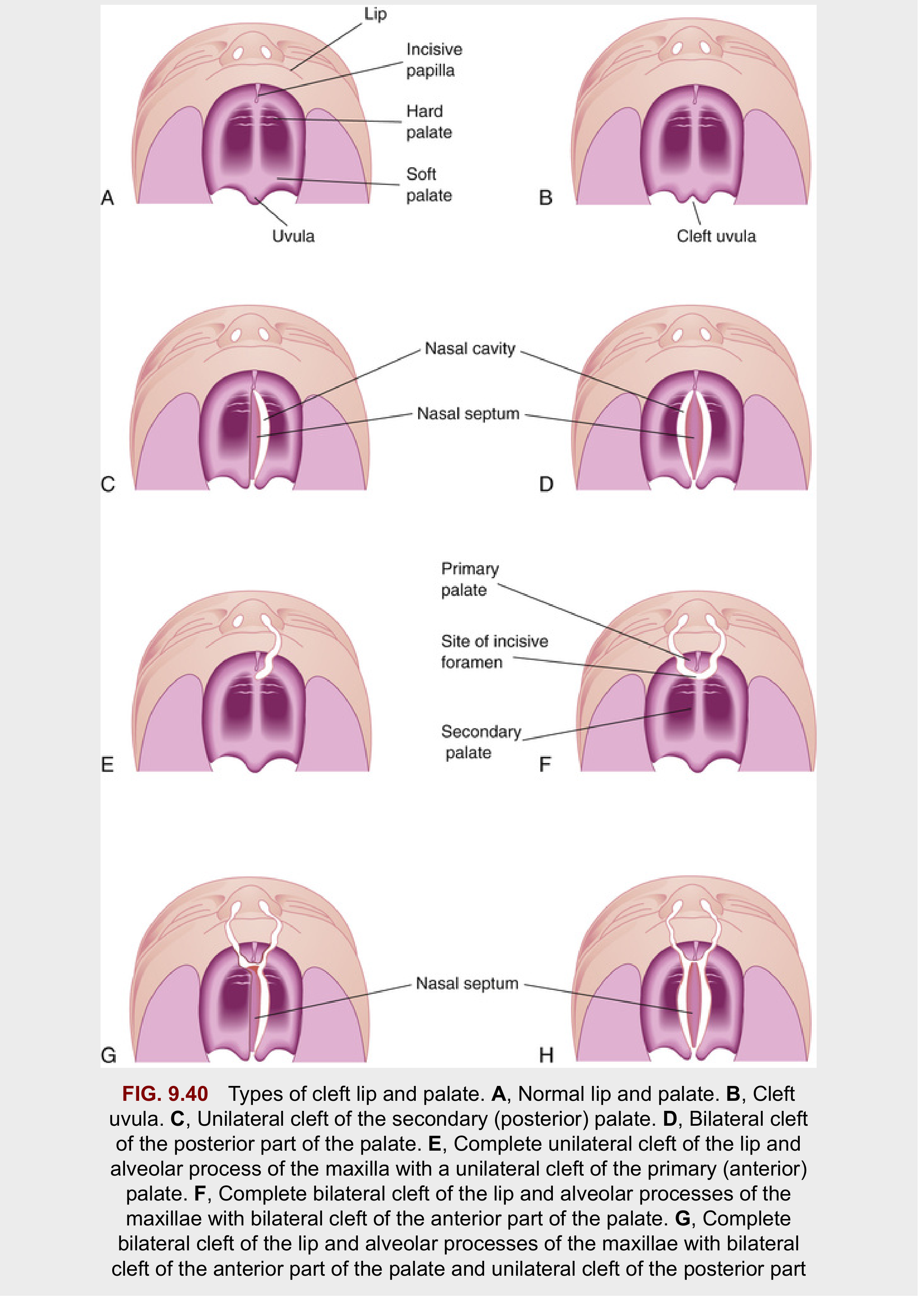
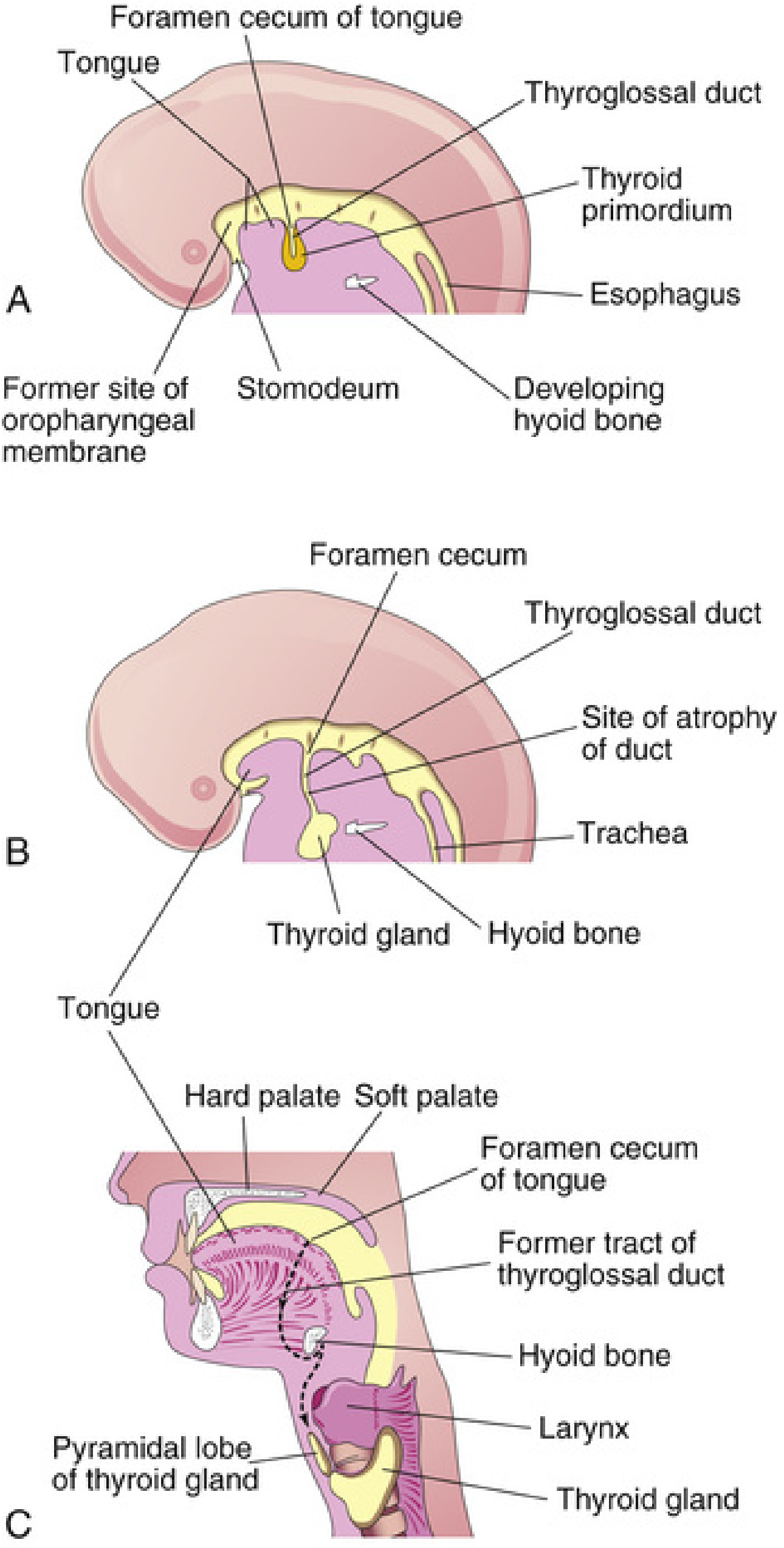
Clefts of the palate are classified into two major groups based on the incisive fossa as reference landmark:
GROUP 1 - Anterior Cleft Defects (Primary Palate Clefts - anterior to incisive fossa)
These involve structures derived from the primary palate.
| Type | Description | Embryological Basis |
|---|---|---|
| Cleft lip only | Unilateral or bilateral notch in upper lip | Failure of the maxillary prominence to merge with the merged medial nasal prominences; the epithelium in the labial groove stretches and breaks down |
| Cleft lip + alveolar cleft | Cleft extends through lip and alveolar process of maxilla up to the incisive fossa | Deficiency of mesenchyme in maxillary prominences and median palatine process; failure to fill labial groove |
| Complete anterior cleft | Cleft through lip, alveolar process, extending to incisive fossa | Failure of mesenchymal masses in lateral palatal processes to meet and fuse with mesenchyme in the primary palate |
- Unilateral anterior cleft: failure on one side only
- Bilateral anterior cleft: failure on both sides; the median palatal process hangs free and projects anteriorly
GROUP 2 - Posterior Cleft Defects (Secondary Palate Clefts - posterior to incisive fossa)
These involve structures derived from the secondary palate (lateral palatine processes).
| Type | Description | Embryological Basis |
|---|---|---|
| Cleft uvula | Mildest form; bifid uvula ("fishtail" appearance) | Failure of fusion at the most posterior point of the soft palate - the last point where palatine processes fuse |
| Cleft soft palate only | Cleft limited to the soft palate | Failure of mesenchymal masses in the lateral palatine processes to meet and fuse with each other in the posterior portion |
| Unilateral cleft of posterior palate | Cleft through soft palate and extends anteriorly through part of the hard palate (posterior to incisive fossa) on one side | Failure of lateral palatine process mesenchyme to fuse with each other and the nasal septum on one side |
| Bilateral cleft of posterior palate | Cleft on both sides of the secondary palate | Bilateral failure of lateral palatine processes to meet each other and the nasal septum |
| Complete posterior cleft | Cleft extends through entire soft palate and hard palate to the incisive fossa | Failure of lateral palatine process mesenchyme to meet and fuse with each other and nasal septum - maximum degree of posterior clefting |
GROUP 3 - Combined (Anterior + Posterior) Cleft Defects
These are the most severe forms, involving both primary and secondary palate.
| Type | Embryological Basis |
|---|---|
| Complete unilateral cleft of lip + alveolus + entire palate | Failure of mesenchymal masses in the lateral palatine processes to fuse with: (1) the primary palate, (2) each other, and (3) the nasal septum - on one side |
| Complete bilateral cleft of lip + alveolus + entire palate | Same failure bilaterally - most severe form; nasal septum hangs freely between the two palatal halves |
The embryological basis is: failure of mesenchymal masses in the lateral palatine processes to meet and fuse with mesenchyme in the primary palate, with each other, AND with the nasal septum.
Summary Table - Types and Embryological Basis
| Type | Structure Affected | Key Developmental Failure |
|---|---|---|
| Cleft uvula | Uvula only | Incomplete fusion at the posterior tip of the secondary palate |
| Cleft soft palate | Soft palate | Lateral palatine processes fail to fuse with each other posteriorly |
| Cleft hard palate (posterior) | Hard palate, posterior to incisive fossa | Lateral palatine processes fail to fuse with each other + nasal septum |
| Cleft lip (anterior) | Lip | Maxillary prominence fails to merge with medial nasal prominence |
| Cleft lip + alveolus (anterior) | Lip + alveolus + primary palate | Mesenchyme deficiency in maxillary prominence + median palatine process |
| Complete unilateral cleft | Lip + alveolus + entire palate | Unilateral total failure of palatine process fusion |
| Complete bilateral cleft | Both sides of lip + alveolus + entire palate | Bilateral total failure - most severe |
Causes and Risk Factors
- Multifactorial inheritance - most common cause (combination of multiple genetic + environmental factors)
- IRF6 gene (interferon regulatory factor 6) - specifically linked to isolated cleft palate
- Chromosomal syndromes: particularly trisomy 13
- Single gene mutations: TTF2, PAX8 related syndromes (e.g., Mohr syndrome - median cleft lip)
- Teratogens: anticonvulsant drugs (e.g., phenytoin, valproate), steroids, alcohol
- Recurrence risk: ~4% in siblings when neither parent is affected; cleft lip + palate is more strongly genetic than isolated cleft palate
Clinical Significance
- Cleft palate alone is more common in girls; cleft lip ± palate is more common in boys
- A sibling of a child with cleft palate has elevated risk of cleft palate but no increased risk of cleft lip (they are embryologically and genetically distinct entities)
- Complete bilateral clefts cause significant deformity because of loss of continuity of the orbicularis oris muscle
- Early recognition is important: affects feeding, speech, hearing (Eustachian tube dysfunction), and dental development
Source: The Developing Human: Clinically Oriented Embryology, pp. 537-548
This is a shared conversation. Sign in to Orris to start your own chat.