Fibrolamellar carcinoma liver
Reading File
Finding Sources
Searching PubMed
fibrolamellar carcinoma liver
Reading File
Reading File
Reading File
Reading Article
PMID: 39814265
Reading File
Reading Article
PMID: 39289102
Reading File
Loading Image
I now have comprehensive data from three textbooks plus recent PubMed literature. Here is a full synthesis:
Fibrolamellar Carcinoma (FLC) of the Liver
Overview
Fibrolamellar carcinoma is a rare primary liver malignancy that is now recognized as a distinct entity from conventional hepatocellular carcinoma (HCC). It accounts for approximately 0.85% of all primary hepatic malignancies in the United States, with an incidence of ~0.02 cases per 100,000 population.
Epidemiology & Risk Factors
- Affects children and young adults, typically age 10-35 years (some sources cite 5-35 years)
- Arises in a non-cirrhotic, otherwise normal liver - no underlying chronic liver disease
- No known predisposing factors (no viral hepatitis, alcohol, or metabolic liver disease association)
- Slightly more common in females
- Roughly equal incidence worldwide (no strong geographic predilection)
Pathogenesis & Molecular Genetics
This is the defining feature that makes FLC unique:
- DNAJB1::PRKACA gene fusion is present in 80-100% of cases - a ~400 kb deletion on chromosome 19 that fuses the heat shock protein gene DNAJB1 with the protein kinase A catalytic subunit gene PRKACA
- This fusion oncogene leads to constitutive activation of protein kinase A (PKA) signaling
- Very few additional mutations exist (<10% of cases have other alterations) - FLC has a remarkably simple mutational landscape compared to conventional HCC
- A small subset of cases (without the fusion) carry inactivating mutations in PRKAR1A (the regulatory subunit of PKA), sometimes associated with Carney complex
- The DNAJB1::PRKACA fusion is now central to diagnosis and is being targeted therapeutically
Recent update (2025): The fusion has also been reported in intraductal oncocytic papillary neoplasm and intraductal papillary mucinous neoplasm, so molecular analysis alone is insufficient for diagnosis - morphology + IHC + molecular testing are all required (Einarsson & Graham, Modern Pathology 2025, PMID 39814265).
Pathology & Histology
Gross appearance:
- Solitary, large, lobulated, well-demarcated tumor
- Characteristic central fibrous scar (radiating fibrous bands)
- Punctate calcification within the scar in >50% of cases
Microscopy:
- Large, polygonal hepatocytes with abundant granular eosinophilic (oncocytic) cytoplasm (due to abundant mitochondria)
- Round nuclei with prominent, centrally-placed macronucleoli
- Separated by parallel lamellae of dense fibrous tissue (the "fibrolamellar" pattern - this is the eponymous feature)
- Pale bodies (cytoplasmic inclusions) and ground-glass inclusions may be present
Immunohistochemistry:
- Positive: CK7, CK19, HepPar-1, CD68, DNAJB1 (C-terminus antibody useful)
- Loss of PRKAR1A expression on IHC is a useful diagnostic marker
- AFP is typically negative or weakly positive (unlike conventional HCC)
Clinical Presentation
- Abdominal pain or discomfort (right upper quadrant)
- Palpable abdominal mass
- Weight loss, malaise, fatigue
- Symptoms often present late (large tumor at diagnosis)
- AFP is usually normal - this is clinically important because it makes screening and monitoring difficult
- Gynecomastia (due to aromatase production by the tumor) has been reported
- Lymph node metastases are common at presentation (~50% of patients)
Imaging
(Grainger & Allison's Diagnostic Radiology)
CT:
- Well-defined, lobulated low-attenuation mass on unenhanced CT
- Central scar with even lower attenuation and radial linear components
- Punctate calcification within the scar (present in >50%) - this is a key distinguishing feature from FNH
- Non-specific arterial enhancement; delayed enhancement of the scar may occur (mimicking FNH)
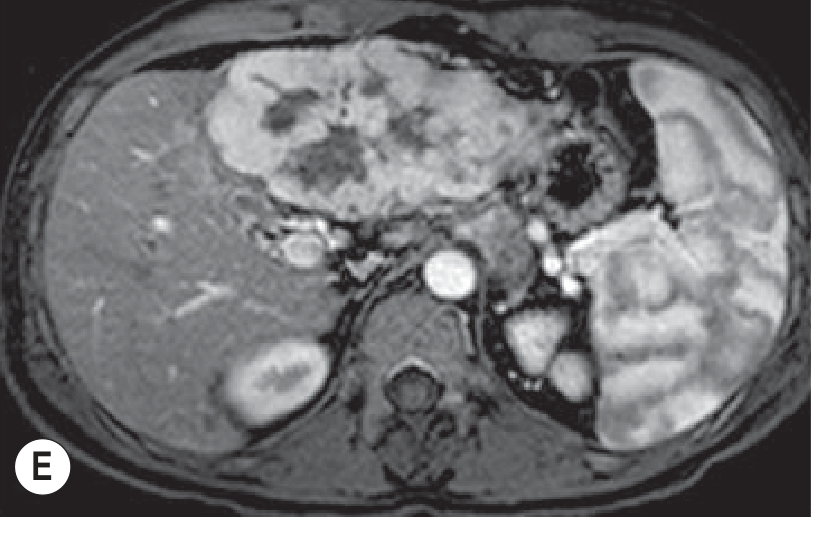
MRI:
- Central scar is low signal on both T1 and T2 - this distinguishes FLC from FNH (where the scar is typically high signal on T2)
- Punctate calcification is rarely demonstrated on MRI
- Heterogeneous mass with fibrous central region showing limited enhancement post-contrast
Ultrasound:
- Increased echogenicity (hyperreflective mass)
- Central scar and calcification may be visible
The axial MRI below (arterial phase T1-weighted) demonstrates a large heterogeneous liver mass with central fibrous region and limited central enhancement:
Key imaging differentiator from FNH:
| Feature | FLC | FNH |
|---|---|---|
| Central scar T2 signal | Low | High |
| Calcification | Common (>50%) | Rare |
| Patient age | 10-35 yrs | 40-50 yrs (F) |
| Malignant behavior | Yes | No |
Diagnosis
A combined approach is required:
- Morphology (histology as above)
- IHC - loss of PRKAR1A, positive DNAJB1 C-terminus staining
- Molecular analysis - DNAJB1::PRKACA fusion by FISH, PCR, or next-generation sequencing
Misdiagnosis is common; differential diagnoses include conventional HCC, intrahepatic cholangiocarcinoma, and hepatic adenoma.
Staging & Prognosis
- FLC has a better prognosis than conventional HCC, partly because of younger patient age and absence of cirrhosis (allows more aggressive resection)
- 5-year survival after resection: ~60%
- Median survival after resection: ~70 months (retrospective series of 575 cases)
- At advanced (unresectable) stages: expected survival <20 months
- Recurrence is common, even after R0 resection; lymph node metastases and peritoneal spread are frequent patterns
- Distant metastases to lung, bone, and adrenal glands occur
Treatment
Surgery (mainstay):
- Surgical resection is the primary treatment - indications are less restrictive than for HCC since the underlying liver is normal
- R0 resection offers the best chance of cure
- Liver transplantation has been explored for unresectable disease; the EASL 2024 position paper notes it as an option for selected cases
Systemic therapy:
- No established standard systemic therapy for advanced/recurrent FLC
- FLC does not respond well to conventional HCC regimens (sorafenib, lenvatinib)
- Clinical trials are focused on:
- Kinase inhibitors targeting the PRKACA fusion protein (e.g., PKA inhibitors)
- Immunotherapy (checkpoint inhibitors - pembrolizumab, nivolumab) given the relatively immune-infiltrated microenvironment
- Targeted therapies based on the unique molecular profile
The 2024 EASL position paper (PMID 39289102) highlights FLC as one of the rare primary liver cancers requiring dedicated collaborative research, as clinical trial data remain sparse.
Summary Table
| Feature | Fibrolamellar Carcinoma |
|---|---|
| Age | 10-35 years |
| Background liver disease | None (non-cirrhotic) |
| Key mutation | DNAJB1::PRKACA fusion |
| AFP | Usually normal |
| Histology | Eosinophilic hepatocytes + fibrolamellar stroma |
| Central scar on imaging | Low T2 signal (vs. FNH = high T2) |
| Calcification | >50% |
| Treatment | Surgical resection |
| 5-year survival (resected) | ~60% |
| Systemic therapy | No standard; trials ongoing |
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), p. 556-558
- Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 853
- Grainger & Allison's Diagnostic Radiology, p. 649-652
- Einarsson & Graham, Modern Pathology 2025 (PMID 39814265)
- Wege et al., EASL Position Paper on Rare Primary Liver Cancers, J Hepatol 2024 (PMID 39289102)
This is a shared conversation. Sign in to Orris to start your own chat.