Maple's breathing system with easier and, uh, detailed explanation, especially D, E, and F.
Reading File
Asking for Preferences
Maples on
It looks like your message got cut off! Could you finish your thought? For example:
- "Maples on a diagram..."
- "Maples on page X of my textbook..."
- "Maples on breathing / respiration..."
Also, what are D, E, and F referring to - labels on a diagram, steps in a process, or something else? Feel free to share an image if you have one!
Mapleson
Finding Sources
Searching the Web
Mapleson breathing circuits D E F explanation anesthesia
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have everything needed for a thorough, easy-to-understand explanation. Here it is:
Mapleson Breathing Circuits - Complete Guide
What is a Mapleson Circuit?
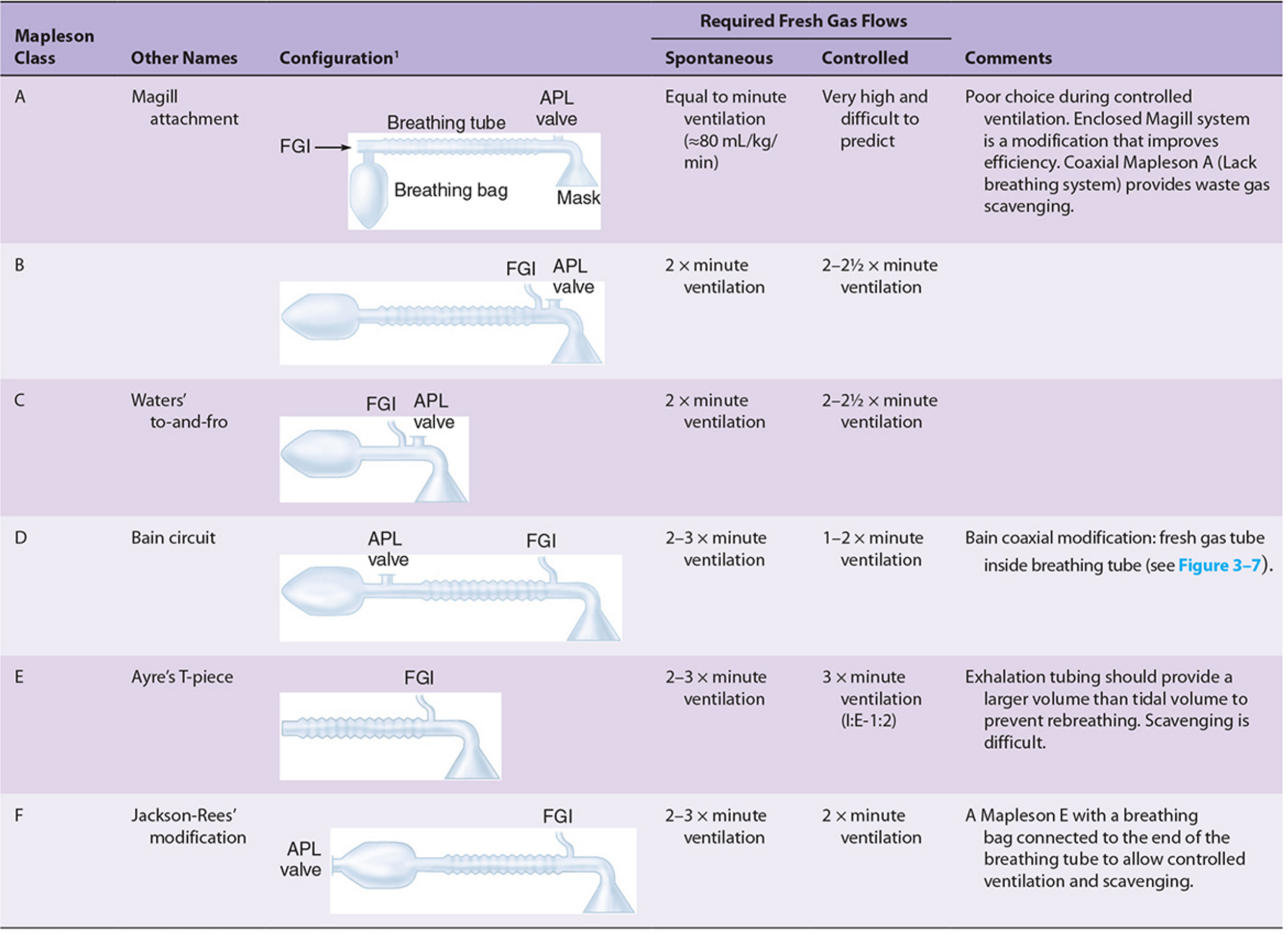
A Mapleson circuit is a semi-open anesthetic breathing system - meaning it has no CO2 absorber. Instead, it flushes out exhaled CO2 by using fresh gas flow (FGF) to push it out through a pop-off valve. There are 6 types (A through F), all sharing the same basic parts arranged differently:
| Part | What it does |
|---|---|
| FGF inlet | Continuously supplies fresh anesthetic gas from the machine |
| Corrugated tubing | Large-diameter tube that holds gas and acts as a reservoir |
| Reservoir bag | Stores extra gas for inspiration; shows breathing effort visually |
| APL valve (pop-off valve) | Lets waste/expired gas escape; prevents pressure buildup |
| Face mask / ETT | Patient connection point |
The key difference between each circuit = where these parts are placed relative to each other.
Quick Overview of All 6 Circuits
Before focusing on D, E, and F - here's the big picture:
- A (Magill) - Best for spontaneous breathing in adults. Least efficient for controlled ventilation.
- B & C - Rarely used today. Inefficient in both modes.
- D, E, F - The "T-piece group." Most commonly used today. Best for controlled ventilation.
The T-Piece Group: D, E, and F in Detail
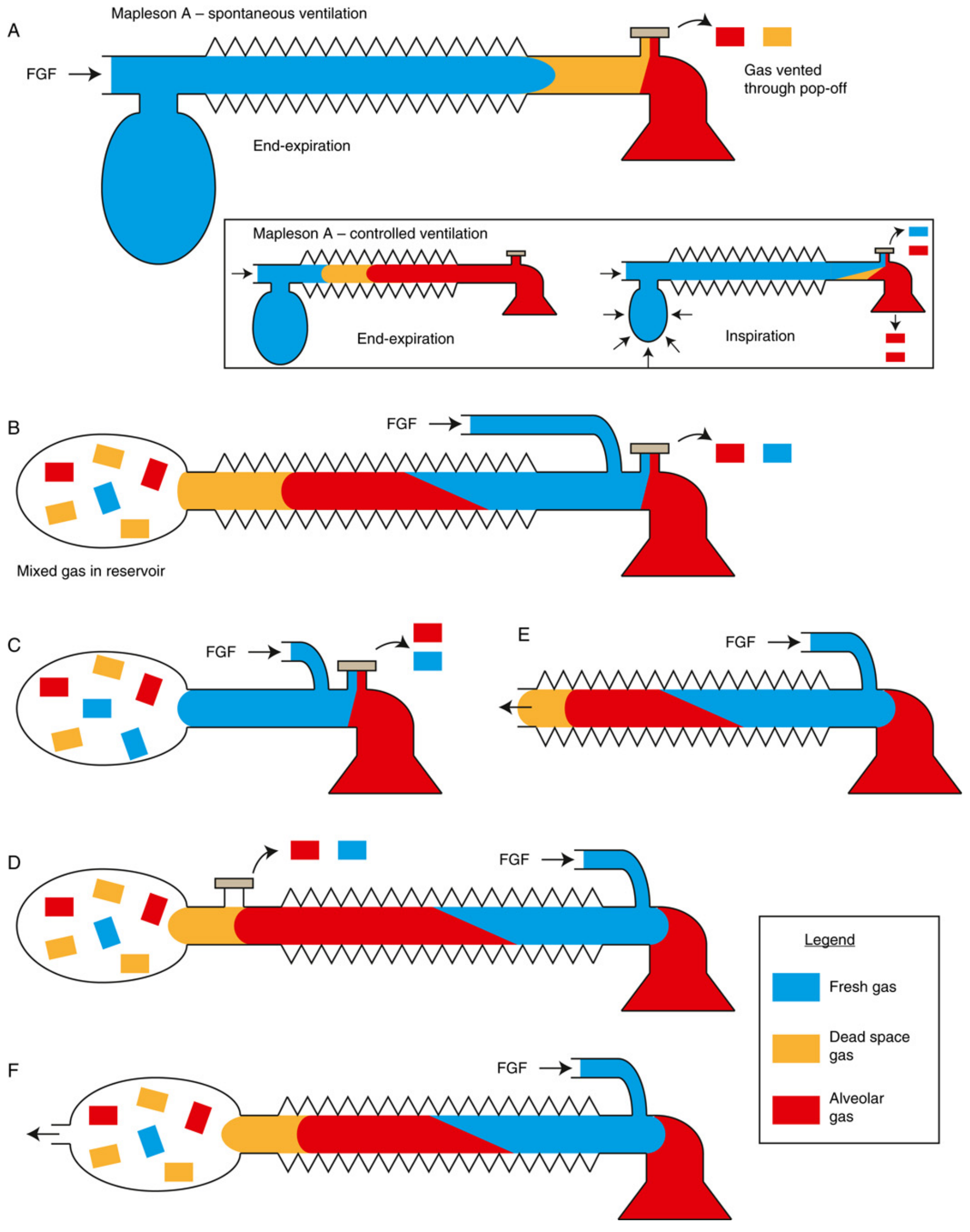
D, E, and F all share the same key feature: FGF enters near the patient end of the circuit (close to the mask/ETT). This is the opposite of Mapleson A, where FGF enters near the reservoir bag.
Mapleson D - "The Bain Circuit"
Layout (patient → APL valve → tubing → FGF inlet → reservoir bag):
Think of it as the exact reverse of Mapleson A.
[Reservoir bag] ← [APL valve] ← [Corrugated tube] ← [FGF inlet] ← [Patient]
How it works:
- Inspiration - Fresh gas from the FGF inlet + gas from the tubing flows to the patient.
- Expiration - Exhaled gas travels back down the tube toward the reservoir bag and APL valve.
- At end-expiration, the tube contains a mix of fresh gas (near patient end) and expired gas (near bag end).
- The APL valve vents expired gas, and fresh gas pushes in to flush it out.
Why FGF near the patient is smart for controlled ventilation:
During positive-pressure ventilation, you control when gas goes in. Having the FGF right at the patient end means fresh gas is always the first thing reaching the lungs - very efficient.
Fresh gas flow requirements:
- Spontaneous breathing: 2-3x minute ventilation (less efficient than Mapleson A)
- Controlled ventilation: 1-2x minute ventilation (more efficient than Mapleson A)
The Bain modification - a coaxial version where the narrow FGF tube runs inside the corrugated tube. This warms the incoming fresh gas (the expired gas in the outer tube pre-heats the fresh gas) and makes the circuit more compact and portable.
Used for: Adults and children during controlled/assisted ventilation; transport; ICU.
Mapleson E - "Ayre's T-Piece"
The simplest of all Mapleson circuits.
[FGF inlet] → [T-junction at patient] → [Open-ended corrugated tube (expiratory limb)]
What makes it unique:
- No reservoir bag
- No APL valve
- Just a T-piece: one arm to the patient, one arm for FGF in, one open tube for expiration out.
How it works:
- Fresh gas flows in continuously through the FGF arm.
- The patient inhales from the T-junction (FGF + gas in the expiratory limb).
- The patient exhales into the open-ended expiratory limb.
- During the expiratory pause, fresh gas fills the expiratory limb, pushing expired gas out of the open end.
- When the next breath starts, the patient gets clean gas from the limb + FGF.
The expiratory limb must be longer than the tidal volume - because it stores a reservoir of fresh gas for the next breath. If it is too short, the patient will rebreathe expired gas.
Pros:
- Ultra-low resistance (no valves!) - ideal for tiny lungs
- No mechanical dead space
- Lightweight, simple, few parts
Cons:
- No bag = can't assist or control ventilation manually (no way to squeeze a breath in)
- Waste gas scavenging is very difficult (open end)
- Barotrauma risk if used with a ventilator (no pressure relief)
- Needs high FGF: 2-3x minute ventilation (spontaneous), 3x minute ventilation (controlled, I:E = 1:2)
Used for: Pediatric patients under 20 kg, neonates, spontaneously breathing patients being weaned from ventilators.
Mapleson F - "Jackson-Rees Circuit"
Mapleson F = Mapleson E + a bag on the expiratory end.
[FGF inlet] → [T-junction at patient] → [Corrugated tube] → [Open-ended reservoir bag]
In 1950, Gordon Jackson Rees modified the Ayre's T-piece by attaching a double-ended bag (open at both ends, one end has an adjustable tap/valve) to the expiratory limb.
What the bag adds:
- You can now squeeze the bag to manually assist or control ventilation.
- The open tail of the bag acts as the pop-off - you can partially close it with your fingers (or a valve) to build up pressure, then release.
- You can see the bag move with each breath (visual feedback of spontaneous breathing effort).
- Allows CPAP (continuous positive airway pressure) application.
How it works in controlled ventilation:
- Partially occlude the open end of the bag with your thumb/finger.
- Squeeze the bag to deliver a breath.
- Release to allow expiration and gas escape.
FGF requirements:
- Spontaneous: 2-3x minute ventilation
- Controlled: 2x minute ventilation (slightly better than E because the bag provides an additional reservoir)
Pros over E:
- Can do controlled + assisted ventilation
- Visual indicator of breathing
- Can apply CPAP
- Slightly more efficient
Cons:
- Scavenging still awkward
- Requires skilled technique to control the open-ended bag correctly
Used for: Pediatric anesthesia (the go-to circuit for children and neonates in many countries), patient transport, ICU.
Side-by-Side Summary: D vs. E vs. F
| Feature | Mapleson D | Mapleson E | Mapleson F |
|---|---|---|---|
| Also called | Bain circuit | Ayre's T-piece | Jackson-Rees |
| Reservoir bag? | Yes (at far end) | No | Yes (at expiratory end, open-ended) |
| APL valve? | Yes | No | No (open end of bag) |
| FGF position | Near patient | Near patient | Near patient |
| Controlled ventilation? | Yes (APL valve) | Very difficult | Yes (squeeze bag) |
| Best for | Adults/children, controlled | Neonates/small children <20 kg, spontaneous | Neonates/pediatrics, all modes |
| FGF (spontaneous) | 2-3x MV | 2-3x MV | 2-3x MV |
| FGF (controlled) | 1-2x MV | ~3x MV | ~2x MV |
| Resistance | Low | Lowest (no valves) | Low |
| Scavenging | Possible via APL | Difficult | Difficult |
Why D, E, F Are the "T-Piece Group"
All three share:
- FGF inlet positioned close to the patient (near the mask/ETT end)
- The reservoir bag/tubing is on the expiratory side (far from patient)
- This means during inspiration, fresh gas is pushed directly toward the patient first - efficient for controlled ventilation
- They all need ~2-3x minute ventilation FGF to prevent CO2 rebreathing (compared to A which needs only 1x MV for spontaneous breathing)
The FGF close to the patient "fills" the expiratory limb during expiratory pauses with fresh gas, so when the next breath starts, the patient inhales fresh gas - not their own expired air.
Sources: Morgan and Mikhail's Clinical Anesthesiology 7e, p. 83-85; Barash et al. Clinical Anesthesia 9e, p. 2010-2011; Miller's Anesthesia 10e, p. 2351-2353
This is a shared conversation. Sign in to Orris to start your own chat.