Penial gland tumor clinical features, invesrigation, managemwnt , dd
Reading File
Finding Sources
Finding Sources
Searching PubMed
pineal gland tumor management
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Pineal Gland Tumors - Complete Clinical Review
Classification
Pineal region tumors are grouped into four broad categories:
| Category | Examples | WHO Grade |
|---|---|---|
| Pineal parenchymal | Pineocytoma | I |
| PPTID (pineal parenchymal tumor of intermediate differentiation) | II-III | |
| Pineoblastoma | IV | |
| Germ cell tumors | Germinoma (most common ~50%), embryonal CA, choriocarcinoma, yolk sac tumor, teratoma | Varies |
| Glial tumors | Astrocytoma | Varies |
| Miscellaneous | Papillary tumor of pineal region (PTPR), meningioma, metastasis | Varies |
Epidemiology: Children, adolescents, and young adults are primarily affected; males > females. Germinomas account for ~50% of all pineal region tumors. Pineal tumors after age 30 are uncommon.
Clinical Features
1. Raised Intracranial Pressure (most common presentation)
- Headache (often severe)
- Nausea and vomiting
- Papilloedema
- The tumor compresses the cerebral aqueduct (Sylvius), causing obstructive hydrocephalus
2. Parinaud's Syndrome (dorsal midbrain syndrome) - pathognomonic
Compression of the superior colliculi/pretectal area causes:
- Loss of upward gaze (most characteristic)
- Loss of convergence
- Pupils: large, react to accommodation but NOT to light (light-near dissociation)
- Retractatory nystagmus on attempted upgaze
- Convergence-retraction nystagmus
3. Endocrine Features
- Precocious puberty in males with germinomas (HCG secretion stimulates Leydig cells)
- Diabetes insipidus if hypothalamus involved
- Sleep disturbance (melatonin disruption, though usually mild)
4. Pineal Apoplexy (rare)
- Sudden hemorrhage into the tumor
- Presents with sudden severe headache + depressed consciousness - mimics subarachnoid hemorrhage
- CT/MRI distinguishes it
5. Late/Additional Features
- Cerebellar ataxia (compression of superior cerebellar surface)
- Spastic weakness
- Diplopia (CN VI or III compression)
- Seizures (uncommon)
Histopathology (H&E)
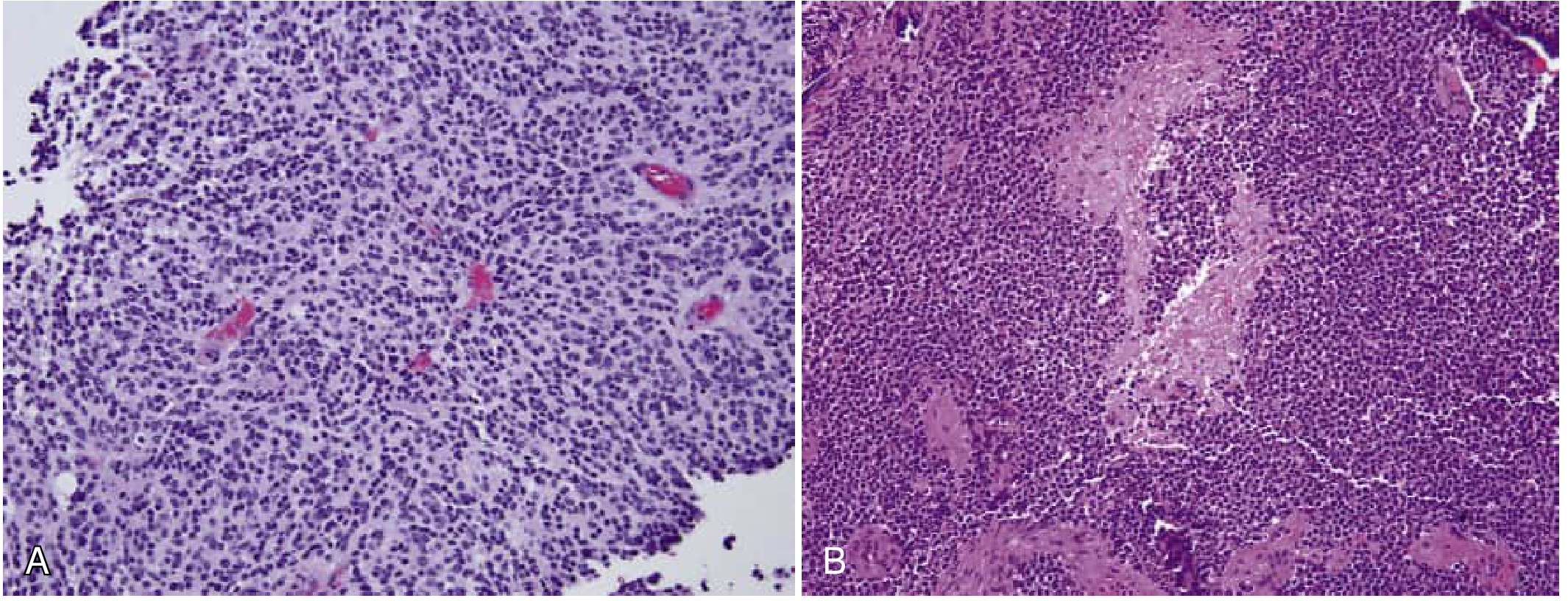
A: PPTID - cellular sheets with minimal pleomorphism. B: Pineoblastoma - dense cellularity with necrosis. (H&E x100)
Key histological features:
- Pineocytoma: Lobular architecture, pineocytomatous rosettes (tumor cells around acellular neuropil center), rare mitoses, synaptophysin+
- PPTID: Sheets of cells, minimal pleomorphism, rosettes absent or rare
- Pineoblastoma: Dense cellularity, nuclear molding, numerous mitoses, necrosis, apoptotic bodies - resembles medulloblastoma; DROSHA mutations common
- Germinoma: Large spherical epithelial cells with reticular connective tissue + many lymphocytes
- PTPR: Papillary architecture with cuboidal/columnar cells on fibrovascular cores; keratin+ and S100+; PTEN mutations, loss of chromosome 10
Investigations
Neuroimaging (primary investigation)
- MRI brain with contrast - investigation of choice
- Shows tumor, compresses tectum and aqueduct
- T2-FLAIR: shows hydrocephalus and transependymal CSF flow
- Sagittal view best for demonstrating tectal compression
- CT head - initial; detects calcification (pineal calcification displaced/enlarged), hemorrhage
Tumour Markers (serum AND CSF)
| Marker | Tumor |
|---|---|
| Beta-hCG (β-hCG) | Germinoma (mild), choriocarcinoma (high) |
| Alpha-fetoprotein (AFP) | Endodermal sinus (yolk sac) tumor, immature teratoma |
| Melatonin (serum/CSF) | Mainly useful for detecting recurrence post-resection |
| Placental alkaline phosphatase (PLAP) | Germinoma |
- Typical germinomas show little elevation of either AFP or β-hCG; significant elevations suggest complex mixed germ cell tumors.
CSF Analysis
- Lumbar puncture (after safe imaging - exclude raised ICP)
- May show tumor cells, lymphocytes, or be entirely normal
- Cytology important for staging (neuraxis seeding)
Histopathology / Biopsy
- Stereotactic biopsy or open surgical biopsy
- Required because each tumor type requires different management
- Endoscopic biopsy via ETV (endoscopic third ventriculostomy) is common in pediatric practice
Management
Step 1 - Treat Hydrocephalus
- External ventricular drain (EVD) - emergency
- Endoscopic Third Ventriculostomy (ETV) - preferred definitive treatment for hydrocephalus; can be combined with biopsy
- VP shunt (if ETV not feasible)
Step 2 - Histological Diagnosis
Surgery is now advised for ALL pineal tumors due to improved microsurgical techniques. Approaches:
- Supracerebellar infratentorial approach - most common
- Occipital transtentorial approach
- Occasionally, if markers are diagnostic (high AFP or β-hCG), empirical treatment may be initiated
Step 3 - Tumor-Specific Treatment
| Tumor | Surgery | Radiotherapy | Chemotherapy |
|---|---|---|---|
| Pineocytoma (WHO I) | Complete resection - often curative | Adjuvant if incomplete | Usually not needed |
| PPTID (WHO II-III) | Maximal safe resection | Focal RT + consider craniospinal | Platinum-based considered |
| Pineoblastoma (WHO IV) | Maximal resection | Craniospinal irradiation | Multiagent chemo (carboplatin, vincristine, etoposide) |
| Germinoma | Biopsy/debulking | Ventricular/focal field RT (highly radiosensitive, excellent prognosis) | Neoadjuvant chemo to reduce RT dose |
| Non-germinomatous GCT | Maximal resection | Whole neuraxis RT | Cisplatin-based chemo (BEP) |
| Glial tumors | Resection | Per grade | Per grade |
| PTPR | Resection | Adjuvant RT if high grade | Under evaluation |
Prognosis:
- Germinoma: >90% 5-year survival with RT
- Pineocytoma: excellent after resection
- Pineoblastoma: poor despite combined therapy
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Pineal cyst | Common incidental finding, benign, no enhancement, stable on follow-up |
| Tectal glioma | Arising from tectum itself, slow-growing, T2-hyperintense on MRI |
| Tentorial meningioma | Older adults, dural tail on MRI, no calcification pattern of pineal |
| Vein of Galen malformation | Neonates/infants, flow voids on MRI, arteriovenous shunting |
| Epidermoid/dermoid cyst | DWI restriction (epidermoid), fat signal (dermoid) |
| Craniopharyngioma | Suprasellar, calcification, bitemporal hemianopia |
| Arachnoid cyst | Follows CSF signal on all sequences, no enhancement |
| Metastasis | Known primary, multiple lesions, ring enhancement |
| Subarachnoid hemorrhage | Pineal apoplexy may mimic; CT distinguishes |
Key Points Summary
- The pineal gland lies in the epithalamus overlying the pretectal area and rostral midbrain, technically outside the brain parenchyma.
- Germinoma is the most common pineal region tumor (~50%); highly radiosensitive with excellent prognosis.
- The classic triad is: raised ICP + Parinaud syndrome + endocrine disturbance.
- Pineal parenchymal tumors express synaptophysin; DROSHA mutations are common in pineoblastoma.
- All pineal tumors should be biopsied/resected when feasible because management differs dramatically by histotype.
- MRI with gadolinium is the cornerstone imaging tool.
Recent Evidence: A 2024 SNO-EANO-EURACAN consensus statement (PMID: 39073785) provides updated management guidelines specifically for pineal parenchymal tumors. A 2026 review "Pineal Tumors and Pineal Region Tumors" (PMID: 42115465) provides the most current surgical and oncological perspective.
Sources: Bradley & Daroff's Neurology in Clinical Practice; Adams & Victor's Principles of Neurology, 12th Ed.; Plum & Posner's Diagnosis and Treatment of Stupor and Coma; Robbins & Cotran Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.