Diagnosis of pulmonary hypertension for md exam answer 10 marks
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pulmonary hypertension"[MeSH Terms] AND diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough 10-mark MD exam answer. Here it is:
Diagnosis of Pulmonary Hypertension
Definition
Pulmonary hypertension (PH) is defined as a mean pulmonary artery pressure (mPAP) >20 mm Hg at rest, measured by right heart catheterization (RHC). The older threshold of ≥25 mm Hg has been revised downward following updated ESC/ERS guidelines. Pulmonary arterial hypertension (PAH) specifically refers to pre-capillary PH with a pulmonary vascular resistance (PVR) ≥3 Wood units and pulmonary artery wedge pressure (PAWP) ≤15 mm Hg, not explained by other causes.
(Fuster and Hurst's The Heart, 15th ed.; Goldman-Cecil Medicine)
WHO Classification (5 Groups)
Understanding the group is essential because diagnosis drives therapy:
| Group | Mechanism | Examples |
|---|---|---|
| 1 | Pulmonary arterial hypertension (pre-capillary) | Idiopathic, heritable, drug-induced, connective tissue disease, HIV, congenital heart disease |
| 2 | Left heart disease (post-capillary) | HFpEF, HFrEF, valvular disease |
| 3 | Lung disease / hypoxia | COPD, ILD, sleep apnea, obesity-hypoventilation |
| 4 | Chronic thromboembolic PH (CTEPH) | Unresolved pulmonary emboli |
| 5 | Unclear / multifactorial | Hematologic, metabolic, sarcoidosis |
Clinical Presentation (History & Symptoms)
The most common presenting symptom is progressive exertional dyspnea. Other features include:
- Fatigue and exercise intolerance
- Exertional chest pain (RV ischemia)
- Exertional syncope or near-syncope (reduced cardiac output)
- Palpitations
- Symptoms of right heart failure in advanced disease: leg edema, right upper quadrant pain (hepatic congestion), ascites
An important diagnostic clue is long-standing dyspnea unresponsive to treatment for more common conditions (asthma, COPD) - many patients see multiple clinicians before PH is considered. (Fishman's Pulmonary Diseases and Disorders)
Risk factor history should include:
- Connective tissue disease symptoms (Raynaud's, dysphagia, skin changes, joint disease)
- Sleep apnea (witnessed apnoeas, daytime hypersomnolence)
- Prior DVT/PE (for CTEPH)
- HIV, liver disease, anorectic drug use
- Family history of PH
Physical Examination Findings
In early/mild PH, examination may be normal. With progression:
Signs of pulmonary hypertension:
- Loud, palpable P2 (pulmonary component of S2)
- Right ventricular heave (parasternal lift)
- Pulmonary ejection click
- Systolic ejection murmur over pulmonary area
Signs of RV failure:
- Elevated JVP with prominent a-wave
- Tricuspid regurgitation murmur: holosystolic at lower left sternal border, increasing with inspiration (Carvallo's sign)
- Right ventricular S3 gallop (accentuated by inspiration)
- Hepatomegaly with expansile pulsations, right upper quadrant tenderness
- Peripheral edema
- Central cyanosis and peripheral cyanosis in advanced disease
Signs suggesting aetiology:
- Telangiectasias, sclerodactyly, digital ulcers - connective tissue disease
- Clubbing - congenital heart disease, certain ILD, PVOD
- Barrel chest, hyperresonance - COPD
- Large neck, macroglossia - obstructive sleep apnoea
Diagnostic Investigations
Diagnosis requires a systematic step-wise approach from non-invasive screening to definitive invasive confirmation.
Diagnostic Algorithm
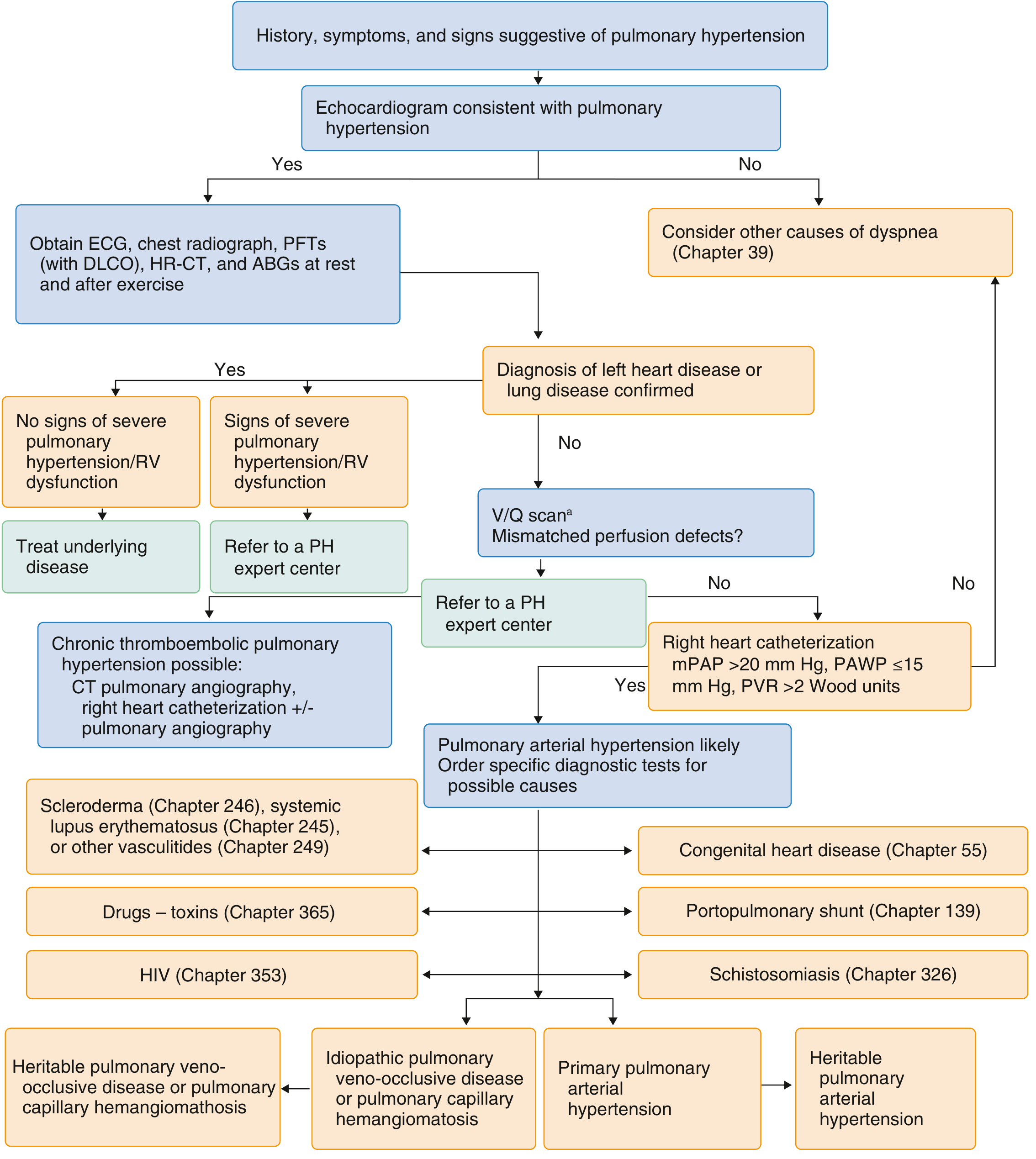
1. Electrocardiogram (ECG)
Findings suggestive of PH:
- Right axis deviation
- Right atrial enlargement (P pulmonale: tall, peaked P waves >2.5 mm in lead II)
- Right ventricular hypertrophy: R:S >1 in V1, S1Q3T3 pattern
- ST depression/T-wave inversion in right precordial leads (V1-V4) - RV strain
- Arrhythmias are uncommon until late disease
ECG is neither sensitive nor specific; a normal ECG does not exclude PH.
2. Chest Radiograph
- Early disease: May be normal
- Progressive disease:
- Prominent central pulmonary arteries with peripheral pruning (oligaemia)
- Enlargement of main pulmonary artery and hilar arteries
- Right heart enlargement: right atrial enlargement (loss of cardiac waist), RV enlargement
- Loss of retrosternal space on lateral view
- May also reveal underlying lung disease (hyperinflation in COPD, diffuse infiltrates in ILD) or evidence of pulmonary oedema (left heart disease)
3. Echocardiography (Key Non-Invasive Test)
Echocardiography is the most important non-invasive screening test for PH.
Estimation of PA pressure:
- Continuous-wave Doppler of tricuspid regurgitation jet: uses modified Bernoulli equation
- RVSP = 4v² + estimated right atrial pressure (v = TR jet velocity in m/s)
- RVSP is assumed equal to PASP when pulmonary valve is normal
- Normal RVSP: 28 ± 5 mm Hg
- TR jet velocity >3.4 m/s suggests high probability of PH
- TR jet velocity 2.9-3.4 m/s suggests intermediate probability
Additional findings:
- RV dilation and hypertrophy
- Flattening/paradoxical motion of interventricular septum ("D-shaped" LV) due to RV pressure overload
- Tricuspid annular plane systolic excursion (TAPSE) reduced (<18 mm) - marker of RV function
- Pericardial effusion (poor prognostic sign)
- Dilated right atrium
- Pulmonary artery dilation (>30 mm)
- IVC dilation and reduced collapse with respiration (elevated RAP)
Echocardiography also identifies left heart disease (Group 2) and congenital heart disease.
Exercise echocardiography may be useful when resting estimates are normal but suspicion is high (e.g., systemic sclerosis with unexplained dyspnea).
4. Pulmonary Function Tests (PFTs) + Arterial Blood Gas
- Help identify and characterise underlying lung disease (Group 3)
- DLCO is reduced in PAH (often disproportionately to lung volumes) and markedly reduced in pulmonary veno-occlusive disease (PVOD)
- Obstruction pattern in COPD; restriction in ILD
- ABG: may show hypoxaemia, elevated A-a gradient; respiratory alkalosis
5. High-Resolution CT (HRCT) of Chest
- Evaluates lung parenchyma for ILD, emphysema, cystic changes
- Pulmonary arteries: dilation of main PA (>29 mm), branching PA enlargement
- May show mosaic attenuation in CTEPH
- PVOD pattern: centrilobular ground-glass nodules, septal lines, mediastinal lymphadenopathy
6. V/Q Scan (Ventilation-Perfusion Scintigraphy)
- Preferred screening test for CTEPH (Group 4)
- CTEPH shows multiple unmatched (mismatched) perfusion defects with normal ventilation
- A normal V/Q scan essentially excludes CTEPH
- CT pulmonary angiography alone may miss CTEPH; V/Q scan is preferred for this purpose
7. CT Pulmonary Angiography (CTPA)
- Used when V/Q scan suggests CTEPH to better delineate thrombus location
- Also helps plan surgical/interventional management of CTEPH
- May identify acute PE, tumour, or other causes
8. Laboratory Tests
Essential workup includes:
- ANA, anti-Scl-70, anti-centromere, anti-ds-DNA, ANCA - connective tissue diseases
- HIV serology
- Liver function tests, hepatitis B & C - portal hypertension
- Thyroid function tests (hypo/hyperthyroidism associated with PAH)
- NT-proBNP/BNP - marker of RV dysfunction; prognostic value; monitoring therapy response
- CBC - polycythaemia, anaemia, thrombocytopaenia (associated causes)
- Coagulation studies, antiphospholipid antibodies (for CTEPH)
- Genetic testing (BMPR2 mutation in heritable PAH) when family history present
9. Right Heart Catheterization (RHC) - Gold Standard
RHC is mandatory to confirm the diagnosis of PH and is required before initiating specific therapy.
Parameters measured:
| Parameter | Normal | Diagnostic Criterion |
|---|---|---|
| mPAP | <20 mm Hg | >20 mm Hg = PH |
| PAWP (or LVEDP) | <12 mm Hg | ≤15 mm Hg = pre-capillary PH |
| PVR | <2 Wood units | ≥3 Wood units = PAH |
| Cardiac output | - | Thermodilution or Fick method |
| Right atrial pressure | - | Elevated = poor prognosis |
PAH diagnosis (Group 1) requires ALL of:
- mPAP >20 mm Hg
- PAWP (or LVEDP) ≤15 mm Hg
- PVR ≥3 Wood units
- Exclusion of left heart disease, lung disease, and CTEPH
Note: PAWP must be measured at end expiration with the transducer levelled at mid-chest. Discordance between PAWP and directly measured LVEDP may occur and left heart catheterization is sometimes needed.
Step-up oximetry during RHC detects left-to-right shunts (congenital heart disease).
10. Acute Vasodilator Testing
Performed during RHC using inhaled nitric oxide (10-20 ppm) or IV adenosine or IV prostacyclin.
Positive response (Vasoresponder) criteria:
- Fall in mPAP ≥10 mm Hg
- Absolute mPAP ≤40 mm Hg
- No fall in cardiac output
About 7% of idiopathic PAH patients are vasoresponders and may respond well to calcium-channel blockers (nifedipine, diltiazem, amlodipine) long-term.
11. Exercise Testing
- 6-minute walk test (6MWT): Assesses functional capacity, prognosis, and treatment response. A distance >440 m correlates with low risk. Serial measurements monitor therapy.
- Cardiopulmonary exercise testing (CPET): Provides detailed haemodynamic and metabolic response data.
- Oximetry at rest and on exercise is important to guide supplemental oxygen.
Summary of Diagnosis Criteria for PAH
| Criterion | Value |
|---|---|
| mPAP | >20 mm Hg |
| PAWP | ≤15 mm Hg |
| PVR | ≥3 Wood units |
| Group 3 excluded | PFTs: no more than mild lung disease |
| Group 4 excluded | V/Q scan: no unmatched defects |
Key Prognostic Markers at Diagnosis
- Functional class (WHO I-IV)
- 6MWT distance
- NT-proBNP level
- Echocardiographic parameters (TAPSE, pericardial effusion)
- RHC: RAP, cardiac output, mPAP
- Evidence of RV failure on imaging or examination
Sources: Fuster and Hurst's The Heart, 15th ed. | Fishman's Pulmonary Diseases and Disorders | Goldman-Cecil Medicine | ESC/ERS 2022 Guidelines for PH
This is a shared conversation. Sign in to Orris to start your own chat.