Recruitment in detail from ent textbooks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have all the material needed for a thorough answer. Here is the complete, detailed response:
Recruitment - A Detailed Account from ENT Textbooks
1. Definition
Recruitment (also called abnormal loudness growth) is the phenomenon in which loudness grows more rapidly than normal at intensity levels just above threshold in an ear with cochlear sensorineural hearing loss. It results in a narrowed dynamic range - the span between the hearing threshold and the loudness discomfort level (LDL) is compressed compared to normal.
In simple terms: a person with recruitment cannot hear soft sounds, but once the sound level rises above their threshold, perceived loudness catches up with - or even overtakes - that of a normal ear very quickly.
"One of the consequences of sensorineural hearing loss is recruitment (abnormal loudness growth). Loudness grows more rapidly than normal at intensity levels just above threshold in an ear with sensorineural hearing loss. This recruitment results in a reduced dynamic range from the threshold level to the discomfort level."
- Shambaugh Surgery of the Ear
2. Normal Dynamic Range - the Baseline
To understand recruitment, the normal dynamic range must be appreciated:
- The normal ear hears from approximately 0 dB HL (threshold) to about 120 dB SPL (pain threshold), giving roughly a 120 dB dynamic range.
- The healthy auditory system achieves this wide range through several mechanisms:
- Compressive behaviour of the basilar membrane (driven by outer hair cells)
- Changes in auditory nerve firing rate
- Spread of excitation along the basilar membrane
- Phase-locking of auditory nerve responses
The equal loudness contours (Fletcher-Munson curves) below illustrate how a normal ear perceives loudness across frequencies:
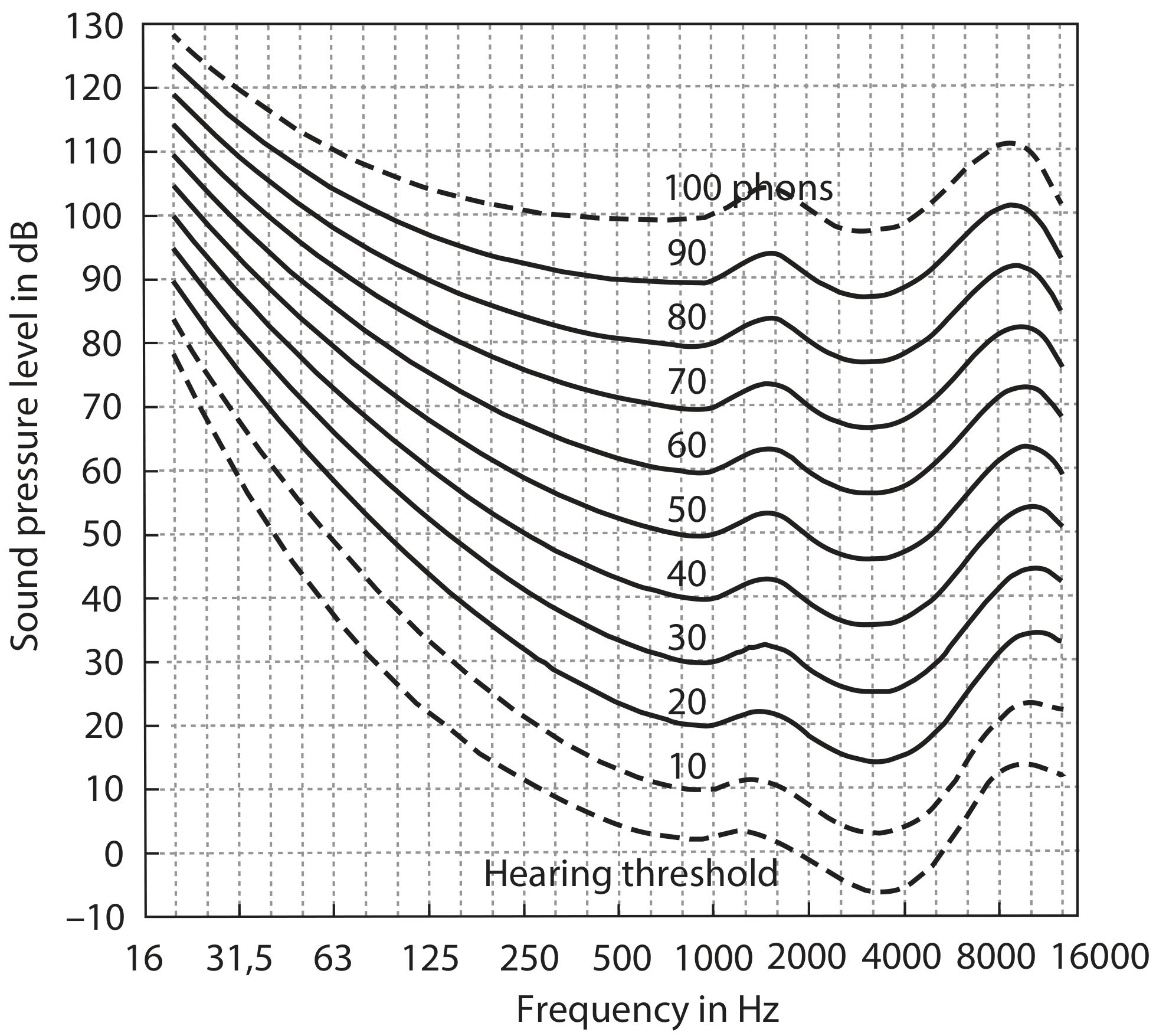
Equal loudness contours. The lower dashed curve = hearing threshold. Contours flatten at high input levels. (Scott-Brown's ORL H&N Surgery, Vol 2)
3. Pathophysiology - Why Does Recruitment Occur?
Role of Outer Hair Cells (OHCs)
Recruitment is fundamentally a consequence of outer hair cell (OHC) damage in the cochlea.
The OHCs provide the cochlea's active mechanism - they act as biological amplifiers particularly for low-to-moderate intensity sounds. The basilar membrane's response normally increases in a compressive (non-linear) manner with increasing input level. For example, a 10 dB increase in sound level leads to only a ~2.5 dB increase in basilar membrane displacement. This wide-ranging compression is what grants the ear its huge dynamic range.
When OHCs are damaged (e.g., by noise, ototoxicity, ageing, or Meniere's disease):
- The compressive amplification is lost or reduced
- The basilar membrane's response becomes more linear (steeper)
- Low-intensity sounds are no longer amplified - hence the elevated threshold
- But high-intensity sounds, which do not depend on OHC amplification, still drive the basilar membrane nearly normally
- Loudness therefore "catches up" rapidly with increasing intensity
"Damage to the active mechanism in hearing loss cases leads to a reduction or loss of cochlear compression and thus to a narrower dynamic range."
- Scott-Brown's ORL H&N Surgery, Vol 2
Adams and Victor add a complementary explanation:
"This phenomenon...is thought to depend on the selective destruction of low-intensity elements subserved by the external hair cells of the organ of Corti. The high-intensity elements are preserved, so that loudness is appreciated only at high intensities."
- Adams and Victor's Principles of Neurology, 12th Ed
Inner Hair Cells (IHCs) and Neural Elements
The inner hair cells and their afferent neurons remain relatively intact in pure OHC disease. This is why:
- Threshold is elevated (OHC amplification lost)
- But once the stimulus is loud enough to activate IHCs directly, loudness grows steeply
Meniere's Disease as a Classic Example
Endolymphatic hydrops distorts the organ of Corti, leading to OHC dysfunction. This produces a hallmark low-frequency fluctuating sensorineural hearing loss with prominent recruitment - which is why patients with Meniere's disease classically complain that sounds are either inaudible or painfully loud, with little in between.
"The resulting deafness is...characterized by diplacusis and loudness recruitment."
- Goldman-Cecil Medicine
4. Clinical Features
| Feature | Description |
|---|---|
| Site of lesion | Cochlear (not retrocochlear) |
| Threshold | Elevated |
| Dynamic range | Markedly narrowed |
| Loudness discomfort level | Normal or near-normal (around 90-100 dB in normals) |
| Diplacusis | Often coexists (pitch distortion) |
| Associated conditions | Meniere's, noise-induced SNHL, presbyacusis, ototoxicity |
Key clinical point: In recruiting deafness, the more-affected ear "gains" in loudness rapidly with increasing intensity and may finally equal the better ear. This is the basis for ABLB testing. In non-recruiting (retrocochlear/nerve) deafness, the original inter-ear loudness difference persists at all suprathreshold levels because both high- and low-intensity neural elements are affected.
5. Tests for Recruitment
These tests were historically used for site-of-lesion diagnosis (cochlear vs. retrocochlear). They have largely been superseded by ABR, acoustic reflexes, and MRI, but remain important conceptually and in some clinical situations.
5.1 Alternate Binaural Loudness Balance (ABLB) Test
- Used for: Unilateral or asymmetrical SNHL
- Method: A pure tone of a given frequency is alternated between the two ears. The patient adjusts the level in the poorer ear to match the perceived loudness in the better ear. This is repeated at several suprathreshold levels to build a "Fowler chart" or "ladderogram."
- Interpretation:
- Recruitment present (cochlear): As intensity rises, the loudness of the impaired ear catches up with the normal ear. A loudness balance achieved at equal dB HL levels (rather than equal sensation levels, dB SL) indicates recruitment.
- No recruitment (retrocochlear): The inter-ear loudness difference remains constant at all levels.
- Limitation: Requires unilateral loss; not usable in bilateral hearing loss.
"A loudness balance achieved at equal intensity levels (dB HL), rather than at equal sensation levels (dB SL), indicates recruitment and suggests a cochlear site of damage."
- KJ Lee's Essential Otolaryngology
5.2 Short Increment Sensitivity Index (SISI)
- Principle: Measures the difference limen for intensity - an indirect measure of recruitment.
- Method: A continuous tone at 20 dB SL is presented, with brief 1 dB increments superimposed. The patient indicates when they detect the increments.
- Interpretation:
- High score (70-100%): Patient detects most 1 dB increments → supports cochlear recruitment
- Low score (0-30%): Fewer increments detected → characteristic of eighth nerve (retrocochlear) lesion
- Rationale: Recruited ears show abnormally steep loudness growth, making small increments perceptible. Nerve-damaged ears lack this steepness.
5.3 Bekesy Audiometry
- Method: Patient traces threshold while a tone automatically sweeps across frequencies, separately for pulsed and continuous tones.
- Interpretation by Bekesy type:
- Type I (pulsed = continuous): Normal
- Type II (continuous drops ~20 dB below pulsed): Cochlear lesion - indicates recruitment and some adaptation
- Type III (continuous drops dramatically in high frequencies): Neural (eighth nerve) lesion
- Type IV (continuous consistently below pulsed): Neural lesion
5.4 Loudness Discomfort Level (LDL) / Uncomfortable Loudness Level (UCL)
- In bilateral cochlear SNHL where ABLB cannot be used, recruitment is assessed by the intensity that causes discomfort.
- Normal: ~100 dB SPL
- In recruiting cochlear loss: LDL may be near-normal (90-100 dB) despite a raised threshold, confirming the narrowed dynamic range.
5.5 Tone Decay Test (TDT) - Differentiating from Retrocochlear
While not a test for recruitment per se, TDT helps differentiate cochlear from retrocochlear:
- Method: Patient listens to a continuous tone slightly above threshold and indicates when it becomes inaudible. Intensity is raised 5 dB if tone fades, until audible for 60 seconds.
- Normal/cochlear: Little or no decay
- Retrocochlear: Decay >25 dB - excessive adaptation (the hallmark of nerve lesions)
6. Recruitment vs. Hyperacusis - Important Distinction
These two conditions are frequently confused:
| Recruitment | Hyperacusis | |
|---|---|---|
| Definition | Abnormal loudness growth associated with raised threshold and narrowed dynamic range | Decreased tolerance to ordinary sounds in an ear with normal or near-normal hearing threshold |
| Hearing threshold | Elevated | Normal or near-normal |
| Mechanism | OHC damage, loss of cochlear compression | Central auditory hypersensitivity, limbic/autonomic involvement |
| LDL | Low but threshold is also high | Very low (sounds intolerable at normal levels) |
| Associated with | Cochlear SNHL (Meniere's, noise exposure) | Tinnitus, PTSD, Williams syndrome, facial nerve injury |
"Loudness recruitment...is a specific experience that is associated with cochlear hearing loss and specifically with dysfunction of the outer hair cells of the organ of Corti."
- Scott-Brown's ORL H&N Surgery, Vol 2
7. Clinical Consequences
Speech Understanding
The narrowed dynamic range impairs speech perception, particularly in noise:
- Soft consonants fall below threshold (inaudible)
- Loud sounds quickly become uncomfortable
- Speech clarity is reduced beyond what the pure audiogram would predict
Hearing Aid Fitting
Recruitment creates the major challenge in hearing aid fitting:
- Simple linear amplification amplifies soft sounds but quickly makes louder sounds uncomfortably loud
- Solution: Modern hearing aids use amplitude compression (non-linear amplification) to:
- Provide more gain for soft sounds
- Progressively reduce gain as input level rises
- Restore a more normal dynamic range
"Loudness recruitment is addressed by the use of amplitude compression in current hearing-aid design."
- Scott-Brown's ORL H&N Surgery, Vol 2
Associated Perceptual Deficits in Cochlear Loss
Recruitment does not occur in isolation. Other perceptual consequences of OHC damage include:
- Loss of frequency selectivity - tuning curves broaden, worsening speech perception in noise
- Loss of temporal fine structure (TFS) processing - affects pitch perception and prosody
- Diplacusis - pitch perceived differently in each ear
8. Summary Table
| Aspect | Detail |
|---|---|
| Definition | Abnormal/rapid loudness growth above threshold |
| Mechanism | OHC damage → loss of cochlear compression → linear BM response |
| Site of lesion | Cochlear (not retrocochlear) |
| Dynamic range | Narrowed (threshold ↑, LDL normal) |
| Key test | ABLB (gold standard for unilateral loss) |
| Other tests | SISI, Bekesy Type II, LDL measurement |
| Classic disease | Meniere's disease |
| Clinical problem | Amplification fitting difficulty |
| Solution | Compression hearing aids |
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2
- Shambaugh Surgery of the Ear
- KJ Lee's Essential Otolaryngology
- Adams and Victor's Principles of Neurology, 12th Ed
- Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.