Plantar reflex and other alternate methods and its components
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Searching the Web
plantar reflex alternate methods Babinski Chaddock Oppenheim Gordon Schaefer Bing components
Finding Sources
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK519555
Here is a complete, well-structured account of the plantar reflex, its components, and all alternate methods of elicitation.
Plantar Reflex (Babinski Sign) - Complete Overview
What Is the Plantar Reflex?
The plantar reflex is a cutaneous (superficial) reflex that tests the integrity of the corticospinal (pyramidal) tract. It is one of the most important signs in clinical neurology.
- How elicited (Babinski's method): A blunt object (tongue blade, key edge, reflex hammer handle) is drawn along the lateral sole of the foot, starting from the heel, moving toward the base of the 5th toe, then arcing medially toward the base of the big toe - in a "J" or "lateral-then-medial" path. Toes should not be touched directly.
- Normal response (adults): Plantar flexion (downward movement) of all toes.
- Abnormal response (Babinski sign / extensor plantar response): Dorsiflexion (upward extension) of the great toe + fanning (abduction) of the other toes. This is a positive Babinski sign and indicates upper motor neuron (UMN) pathology.
Components of the Babinski Sign (Positive Plantar Response)
The positive plantar reflex has two key components:
| Component | Description |
|---|---|
| Extension of the great toe | Dorsiflexion (upward movement) of the hallux - the cardinal sign |
| Fanning of the other toes | Spreading/abduction of the 2nd-5th toes (not always present) |
A third component sometimes seen in severe UMN lesions is the "triple flexion response" - dorsiflexion of the toes + dorsiflexion of the foot + flexion at the knee and hip. This is a spinal flexor reflex with the same significance as the Babinski sign.
Note: The fanning of toes may be absent in some cases of clear UMN disease. Dorsiflexion of the hallux is the most reliable component. - Adams and Victor's Principles of Neurology, 12th Ed.
Significance
- Positive Babinski (extensor response) in adults = damage to the corticospinal system (UMN lesion)
- Location: anywhere from the motor cortex down through the internal capsule, brainstem, or spinal cord, above the S1 level
- In neonates and infants up to ~18 months, an extensor response is normal (incomplete myelination)
- The sign may be absent in the presence of marked atrophy of the toe extensor muscles even with UMN disease - Bradley and Daroff's Neurology in Clinical Practice
Why Alternate Methods Are Needed
Sometimes the standard plantar stroke cannot be used or gives unreliable results due to:
- Excessive withdrawal response to plantar stimulation (ticklishness, pain sensitivity)
- Lesions/wounds on the lateral plantar surface of the foot
- Uncooperative or confused patients
- Desire to confirm an equivocal response
All alternate methods produce the same positive response - dorsiflexion of the hallux and/or fanning of the toes - and carry the same clinical significance as the Babinski sign.
Alternate Methods for Eliciting the Extensor Plantar Response
1. Chaddock's Sign (1911)
- Stimulus: Stroke the skin in a circular arc around and below the lateral malleolus (external malleolar region)
- Direction: From below the lateral malleolus along the dorsolateral foot
- Advantage: Minimizes withdrawal response since the plantar surface is not touched. Useful when plantar skin is injured or the patient is hypersensitive
- Sensitivity: ~95.7% in UMN lesions - nearly as sensitive as Babinski's method. May appear before Babinski and disappear later; can be positive bilaterally even with a unilateral lesion
- StatPearls - Chaddock Reflex, NCBI
2. Oppenheim's Sign (1902)
- Stimulus: Firm downward pressure with the thumb and index finger along the anterior (medial) surface of the tibia, from just below the knee to the ankle
- Response: Same extensor toe response
- Sensitivity: ~27-30% - less sensitive than Babinski or Chaddock
- Useful when the foot cannot be accessed
3. Gordon's Sign
- Stimulus: Firm squeezing or pinching of the calf muscle (gastrocnemius)
- Response: Dorsiflexion of the great toe
- Less commonly used; useful as a quick confirmatory test
4. Schaefer's Sign
- Stimulus: Firm squeezing of the Achilles tendon
- Response: Same extensor response
- Sensitivity: ~42.5% in UMN lesions - intermediate sensitivity between Chaddock and Oppenheim
- PMC6073965 - Differentiating Extensor Plantar Response
5. Bing's Sign (1915)
- Stimulus: Multiple pinpricks on the dorsum of the foot (over the dorsal surface)
- Response: Dorsiflexion of the hallux
- Sometimes more effective when the standard stroke fails
6. Cornell's Sign
- Stimulus: Stroking along the dorsum of the foot along the extensor hallucis longus tendon (inner/medial side)
- Response: Extensor response
7. Gonda's Sign
- Stimulus: Forceful downward stretching and sudden snapping/release of the 2nd or 4th toe
- Response: Dorsiflexion of the great toe
- Useful when direct foot stimulation is not possible
8. Stransky's Sign
- Stimulus: Vigorous abduction and sudden release of the little (5th) toe
- Response: Extensor plantar response
9. Moniz's Sign
- Stimulus: Forceful passive plantar flexion of the ankle
- Response: Dorsiflexion of the hallux
10. Strümpell's Sign
- Stimulus: Patient attempts to flex the knee against resistance applied by the examiner
- Response: Involuntary dorsiflexion of the great toe during this effort
11. Throckmorton's Reflex
- Stimulus: Percussion (tapping) over the metatarsophalangeal joint of the big toe
- Response: Dorsiflexion of the hallux
12. Brissaud's Reflex
- Stimulus / Use: In patients with a missing great toe or complete paralysis of toe extension, stroke the plantar surface
- Response: Instead of toe extension, contraction of the tensor fascia lata (hip internal rotation) is observed - this carries the same UMN significance
Summary Table of Alternate Methods
| Sign | Stimulus Site | Method |
|---|---|---|
| Babinski (standard) | Lateral sole | Stroke heel → base of 5th toe → medially |
| Chaddock | Around lateral malleolus | Stroke arc below/around malleolus |
| Oppenheim | Anterior tibia | Downward pressure with thumb+index finger |
| Gordon | Calf muscle | Squeeze/pinch gastrocnemius |
| Schaefer | Achilles tendon | Squeeze tendon firmly |
| Bing | Dorsum of foot | Multiple pinpricks |
| Cornell | Extensor hallucis longus tendon | Stroke along tendon on dorsum |
| Gonda | 2nd or 4th toe | Stretch/snap toe downward |
| Stransky | 5th (little) toe | Abduct and suddenly release |
| Moniz | Ankle | Forceful passive plantar flexion |
| Strümpell | Knee (effort-based) | Patient flexes knee against resistance |
| Throckmorton | 1st MTP joint | Percussion over joint |
| Brissaud | Plantar (amputation) | Observe tensor fascia lata contraction |
Clinical Notes
- Sensitivity comparison: Babinski (~59.7%) > Chaddock (~55.3%) > Schaefer (~42.5%) > Oppenheim (~30%)
- The Babinski and Chaddock methods are complementary - each can be positive when the other is negative; using both increases detection
- An equivocal (mute) plantar response - neither clearly up nor down - should not be called positive; it may reflect withdrawal artifact or early/subtle disease
- In the context of acute UMN injury (e.g., stroke), the Babinski sign can appear within hours and is an early, sensitive marker
- Absent superficial reflexes (abdominal, cremasteric) alongside a positive extensor plantar response provide additional confirmatory evidence of UMN disease - Harrison's Principles of Internal Medicine, 22nd Ed.
Methods of testing ketone bodies
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Here is a complete and well-structured account of all methods for testing ketone bodies, drawn from authoritative laboratory medicine textbooks.
Methods of Testing Ketone Bodies
The Three Ketone Bodies
The three ketone bodies produced in the liver and their interconversions:
| Ketone Body | Proportion (Normal) | Notes |
|---|---|---|
| Acetoacetate | ~50% | Primary measurable ketone; detected by most tests |
| Beta-hydroxybutyrate (BHB) | ~50% | Not a true ketone chemically; rises to 6:1 ratio vs. acetoacetate in severe DKA |
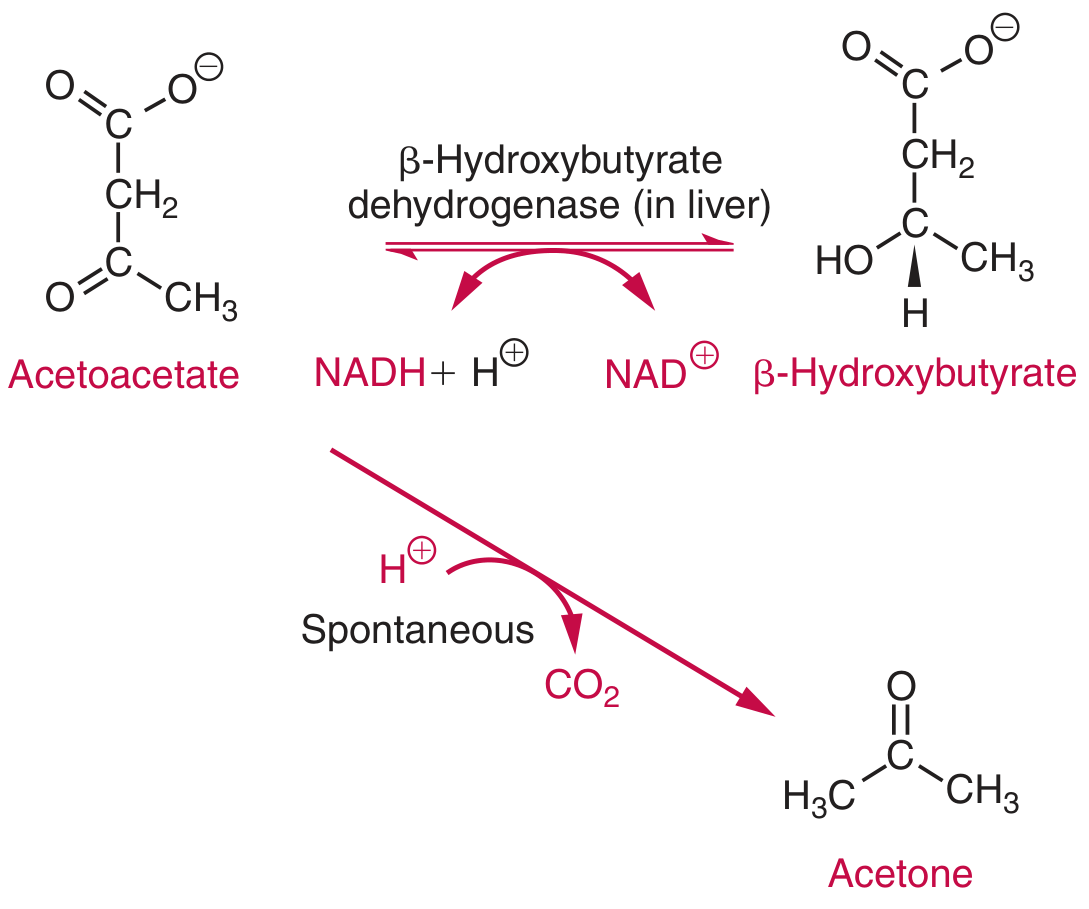
| Acetone | Trace | From spontaneous decarboxylation of acetoacetate; volatile |
Key limitation: No single commonly used test reacts with all three ketone bodies. Most routine methods detect acetoacetate only, or acetoacetate + acetone. Beta-hydroxybutyrate - the predominant ketone in severe DKA - is missed by nitroprusside-based tests. A negative nitroprusside test does NOT rule out ketoacidosis. - Tietz Textbook of Laboratory Medicine, 7th Ed.
Classification of Testing Methods
A. URINE KETONE TESTS
1. Rothera's Test (Nitroprusside / Legal's Test - Classic)
- Principle: Sodium nitroprusside (sodium nitroferricyanide) + ammonia reacts with acetoacetate and acetone in alkaline medium to produce a purple/violet color
- Detects: Acetoacetate (most sensitive) and acetone (less sensitive)
- Does NOT detect: Beta-hydroxybutyrate
- Sensitivity: Acetoacetate ~1-5 mg/dL; Acetone ~10-25 mg/dL
- Procedure:
- To 5 mL urine, add a small amount of ammonium sulfate crystals and a few crystals of sodium nitroprusside
- Dissolve and layer concentrated ammonia on top
- A purple/violet ring at the interface = positive result
- Modern equivalents: The reagent strip (dipstick) and Acetest tablet are both based on this same nitroprusside principle
2. Gerhardt's Test (Ferric Chloride Test)
- Principle: Ferric chloride (FeCl₃) reacts with acetoacetate to form a Bordeaux red/port-wine color
- Detects: Acetoacetate only
- Does NOT detect: Beta-hydroxybutyrate or acetone
- Sensitivity: Low (~25-50 mg/dL) - much less sensitive than nitroprusside tests
- Procedure:
- Add a few drops of 10% ferric chloride solution to urine
- A red/burgundy color = positive (acetoacetate present)
- Limitation: Not specific - also gives a positive reaction with salicylates (aspirin), L-dopa, phenol compounds - Henry's Clinical Diagnosis and Management by Laboratory Methods
- Distinction test: Boiling the urine removes acetoacetate (it breaks down to acetone and CO₂); if the color disappears on boiling and returns when cooled, it confirms acetoacetate
3. Dipstick (Reagent Strip) Test
Two main formulations:
| Strip Type | Reagent | Detects | Sensitivity | Read at |
|---|---|---|---|---|
| Multistix | Sodium nitroprusside + buffer | Acetoacetate only | 5-10 mg/dL | 15 seconds |
| Chemistrip | Sodium nitroprusside + glycine (alkaline medium) | Acetoacetate and acetone | AA: 10 mg/dL, Acetone: 70 mg/dL | 60 seconds |
- Color change: Beige → Violet (positive)
- False positives: Phenylketones, BSP/PSP dyes, L-dopa metabolites, methyldopa, captopril, acetylcysteine, MESNA
- False negatives: Degraded reagents, bacterial breakdown of acetoacetate in stale urine, acetone loss (volatile)
- Reagent strips correlate moderately with plasma acetoacetate and poorly with total blood ketones
4. Acetest (Nitroprusside Tablet Test)
- Reagents in tablet: Sodium nitroprusside + glycine + strongly alkaline buffer + lactose
- Detects: Acetoacetate (5-10 mg/dL) and acetone (20-25 mg/dL); does NOT detect BHB
- Advantage: Can be used on urine, serum, plasma, or whole blood; avoids interference from deeply colored urine
- Procedure:
- Place tablet on white paper
- Add 1 drop of specimen; compare color at 30 seconds (urine), 2 minutes (serum/plasma), 10 minutes (whole blood - remove clot first)
- Color ranges from lavender to deep purple; reported as Negative / Small / Moderate / Large
- Lactose in the tablet enhances color development
5. AimTab (Ketone Tablet)
- Contains: glycine + sodium nitroprusside + disodium phosphate (optimum pH) + lactose
- Same principle as Acetest; disodium phosphate provides optimum reaction pH
- Detects acetoacetate and acetone; BHB does not react
6. Ketostix (Reagent Strip)
- Modification of the nitroprusside test using a reagent strip format
- Positive reaction within 15 seconds with ≥50 mg/L acetoacetate
- Color chart gives semi-quantitative readings: 50, 150, 400, 800, 1600 mg/L
- Acetone also reacts but test is less sensitive to it
B. BLOOD / SERUM KETONE TESTS
7. Enzymatic Assay for Beta-Hydroxybutyrate (Gold Standard for DKA)
- Principle:
- BHB + NAD⁺ → acetoacetate + NADH (catalyzed by beta-hydroxybutyrate dehydrogenase)
- NADH then reduces nitroblue tetrazolium (NBT) via diaphorase → purple compound (read at 505 nm)
- Detects: Beta-hydroxybutyrate specifically and quantitatively
- Specimen: Serum, plasma, or whole blood (fingerstick capillary blood with handheld meters)
- Clinical use: Most accurate method for monitoring DKA treatment (BHB correlates better than acetoacetate with acid-base status changes)
- Devices: Precision Xtra (Abbott), Nova Max Plus (Nova Biomedical), STAT-Site M BHB (EKF Diagnostics)
- Limitation: Meters are less accurate at concentrations >3 mmol/L
8. Indirect BHB Detection (Traditional)
When only nitroprusside-based equipment is available:
- Boil urine to evaporate and remove acetone and acetoacetate (acetoacetate first breaks down to acetone + CO₂)
- Gently oxidize remaining BHB to acetoacetate using H₂O₂, ferric ions, or dichromate
- Detect the newly formed acetoacetate with Gerhardt's test or a nitroprusside method
C. BREATH TESTING
9. Breath Acetone Detection
- Acetone is volatile and excreted in expired air
- The characteristic fruity/acetone breath (ketotic fetor) is a clinical sign of severe ketosis
- Formal breath analyzers exist but are not standard clinical tools; used mainly in research and metabolic monitoring for ketogenic diet adherence
Summary Comparison Table
| Method | Specimen | Detects | Sensitivity | Clinical Use |
|---|---|---|---|---|
| Rothera's test | Urine | Acetoacetate + acetone | AA: 1-5 mg/dL | Classic lab test |
| Gerhardt's (FeCl₃) | Urine | Acetoacetate only | ~25-50 mg/dL | Less used; low sensitivity |
| Dipstick (Multistix) | Urine | Acetoacetate only | 5-10 mg/dL | Rapid bedside |
| Dipstick (Chemistrip) | Urine | AA + acetone | AA: 10 mg/dL | Rapid bedside |
| Acetest tablet | Urine/blood/serum | AA + acetone | AA: 5-10 mg/dL | When colored urine |
| AimTab | Urine/serum | AA + acetone | Similar to above | Semi-quantitative |
| Ketostix strip | Urine | AA + acetone | ≥50 mg/L | Semi-quantitative |
| Enzymatic BHB assay | Blood/serum | BHB specifically | ~0.1 mmol/L | DKA monitoring (best) |
| Indirect BHB | Urine | BHB (after oxidation) | Low | Not routine |
| Breath acetone | Expired air | Acetone | Clinical only | Research/screening |
Key Clinical Points
- Most nitroprusside-based tests miss BHB, which rises to 6:1 ratio vs. acetoacetate in severe DKA. A negative dipstick does NOT exclude DKA
- Gerhardt's test is non-specific - salicylates, L-dopa, and phenols give false positives
- Sample stability: Acetoacetate is degraded by bacteria in stale urine and acetone is volatile - test fresh specimens; refrigerate in closed containers
- ADA recommendation: Patients with Type 1 DM should test ketones when blood glucose consistently >300 mg/dL, during illness/stress, in pregnancy, or with symptoms of DKA
- SGLT2 inhibitor users are at risk for euglycemic DKA - blood BHB testing is preferred as glucose may be near-normal - Tietz Textbook of Laboratory Medicine, 7th Ed.
Components of plantar reflex
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
components of plantar reflex arc receptor afferent efferent muscle Babinski sign anatomy
Here is a detailed breakdown of the components of the plantar reflex, covering both the reflex arc anatomy and the observable response components.
Components of the Plantar Reflex
The plantar reflex has two levels of "components" that are commonly examined:
- Components of the reflex arc (anatomical pathway)
- Components of the observable response (clinical findings)
Part 1: Components of the Reflex Arc
The plantar reflex is a superficial (cutaneous) reflex with a polysynaptic arc involving the following five components:
1. Receptor
- Location: Skin of the sole of the foot - specifically the first sacral (S1) dermatome (the lateral sole and ball of the foot)
- Type: Free nerve endings (nociceptive/tactile receptor endings) responding to stroking/pressure stimulus
2. Afferent (Sensory) Limb
- Nerve: Tibial nerve (a branch of the sciatic nerve)
- Spinal segments: L4, L5, S1, S2
- Carries the sensory signal from the plantar skin up to the spinal cord dorsal horn
3. Integration Centre (Reflex Centre)
- Location: Spinal cord segments L4-L5 to S1-S2
- In the normal adult: the corticospinal tract exerts inhibitory control over the spinal interneuronal pool at these levels, suppressing the primitive extensor (flexor withdrawal) response and allowing the normal flexor toe response
- When the corticospinal tract is damaged: this inhibition is lost, releasing the spinal flexor reflex, producing the extensor (Babinski) response
4. Efferent (Motor) Limb
- Nerve: Tibial nerve (for normal flexor response - flexor hallucis brevis)
- Nerve: Deep peroneal (fibular) nerve (for abnormal extensor response - extensor hallucis longus)
- Two key muscles are involved depending on the response:
| Response | Muscle Activated | Nerve |
|---|---|---|
| Normal (plantar flexion) | Flexor hallucis brevis | Tibial nerve |
| Abnormal (dorsiflexion - Babinski) | Extensor hallucis longus | Deep peroneal nerve |
The muscle that mediates the Babinski sign is the extensor hallucis longus (not the extensor hallucis brevis), and it is invariably accompanied by reflex activity in the tibialis anterior. - van Gijn, The Plantar Reflex (Erasmus University)
5. Effector (Muscle Response)
- The toes and foot muscles produce the visible response (see Part 2 below)
Part 2: Components of the Observable Response
When the plantar reflex is elicited, three possible responses can occur:
A. Normal Response (in adults)
Plantar flexion of all toes - toes curl downward toward the stimulus. This is a "negative Babinski." Mediated by contraction of flexor hallucis brevis.
B. Abnormal Response - The Babinski Sign (Positive Extensor Plantar Response)
The positive Babinski sign has two cardinal components:
Component 1: Dorsiflexion (Extension) of the Great Toe (Hallux)
- The hallux moves upward (away from the stimulus)
- This is the most important and constant component - mediated by extensor hallucis longus
- May occur even without fanning of the other toes
- Can be absent if the toe extensor muscles are severely atrophied
Component 2: Fanning (Abduction/Spreading) of the Other Toes
- The 2nd-5th toes spread apart (abduct) and extend
- Often accompanies Component 1 but is not always present
- Less reliable as a standalone sign than hallux dorsiflexion
"The main features of the Babinski sign are dorsiflexion of the large toe and fanning of the other toes." - Adams and Victor's Principles of Neurology, 12th Ed.
C. Triple Flexion Response (Severe UMN Lesion)
A third, more extensive component seen in severe or established UMN lesions:
| Component | Movement |
|---|---|
| Toe dorsiflexion | Upward extension of toes |
| Dorsiflexion of the foot | Foot pulled upward at ankle |
| Flexion at knee and hip | Limb withdrawal |
This is a spinal flexor (nociceptive withdrawal) reflex released from corticospinal inhibition. It carries the same UMN significance as the Babinski sign but is more dramatic. - Adams and Victor's Principles of Neurology, 12th Ed.
Variants of the Babinski Sign
| Type | Description |
|---|---|
| True Babinski | Full components - hallux dorsiflexion + toe fanning |
| Minimal | Only tensor fascia lata and hamstrings contract (no visible toe movement - seen in amputees or toe paralysis) |
| Pseudo-Babinski | Due to plantar hyperaesthesia and choreoathetosis; not a true UMN sign |
| Exaggerated | Full extensor or flexor spasm depending on muscle group tone |
Three Possible Responses to Plantar Stimulation
| Response | Appearance | Significance |
|---|---|---|
| Flexor (normal) | Toes curl downward, foot everts | Normal in adults |
| Indifferent (mute/equivocal) | No response | Inconclusive; may be early/subtle UMN disease |
| Extensor (Babinski positive) | Hallux dorsiflexes + toes fan out | UMN lesion (corticospinal tract damage) |
Why the Normal Response Differs by Age
| Age Group | Normal Response | Reason |
|---|---|---|
| Infants (<18 months) | Extensor (Babinski-like) | Corticospinal tract not yet fully myelinated - no inhibitory control |
| Adults | Flexor (plantar flexion) | Mature corticospinal inhibition suppresses the spinal extensor reflex |
"In infants whose corticospinal tracts are not well developed, dorsiflexion of the great toe and fanning of the other toes is the natural response to stimuli applied to the sole of the foot." - Ganong's Review of Medical Physiology, 26th Ed.
Summary
The plantar reflex components in brief:
- Receptor: Free nerve endings, S1 dermatome, sole of foot
- Afferent: Tibial nerve, L4-L5-S1-S2 segments
- Centre: Spinal cord L4-S2 (modulated by corticospinal tract)
- Efferent: Tibial nerve (normal) / Deep peroneal nerve (abnormal)
- Effector muscles: Flexor hallucis brevis (normal) / Extensor hallucis longus + tibialis anterior (abnormal)
- Response components: (1) Hallux dorsiflexion + (2) Toe fanning ± (3) Triple flexion
This is a shared conversation. Sign in to Orris to start your own chat.