Occular examination in clinical posting
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive content from authoritative sources. Let me compile the full, well-structured answer.
Ocular Examination in Clinical Posting
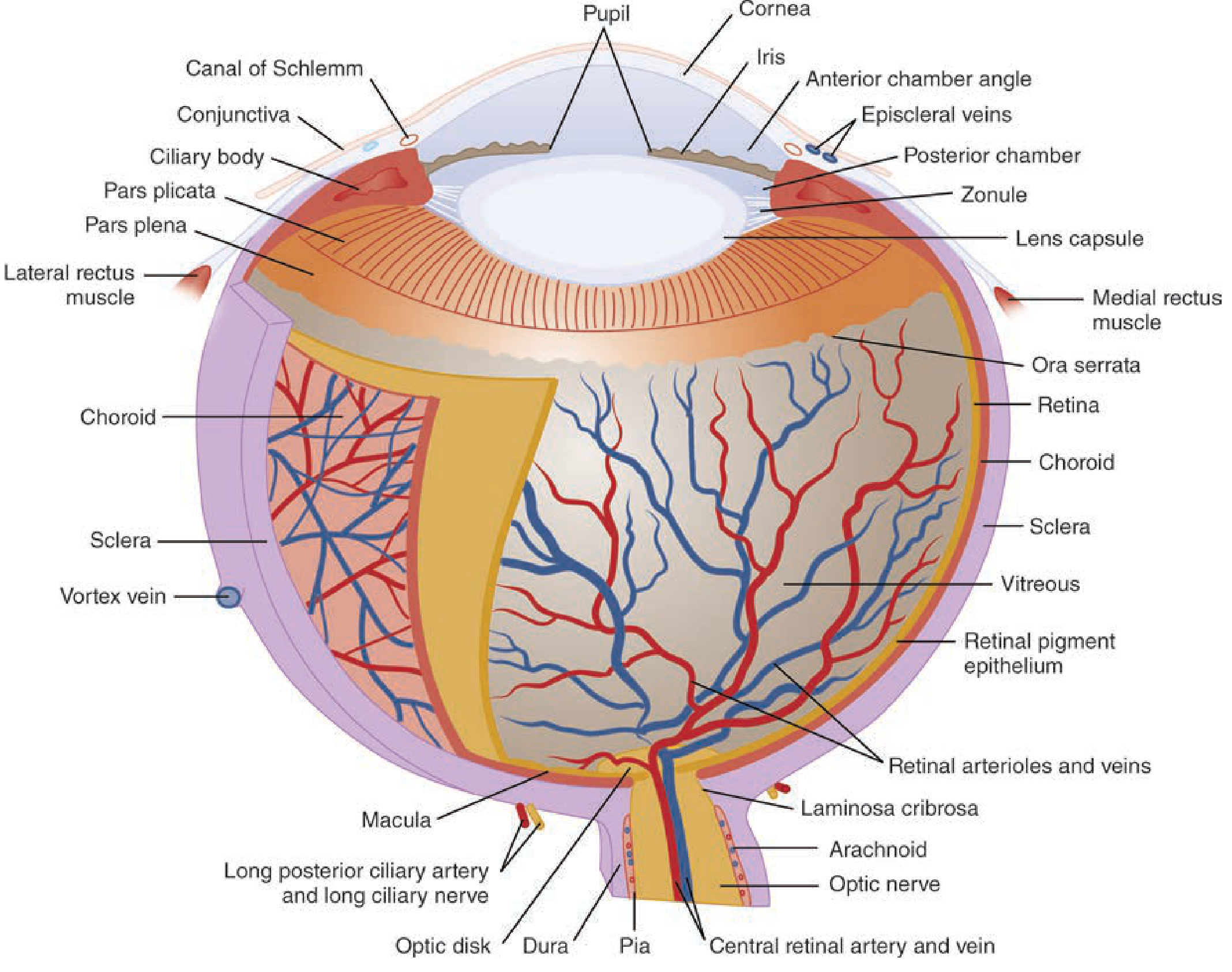
Anatomy Overview
Before beginning the exam, familiarity with ocular anatomy is essential.
Order of Examination
The standard ocular examination proceeds in a fixed sequence. This order is not arbitrary - each step informs the next, and more invasive steps (like tonometry) come last.
"Full examination should include the following, generally in the order listed: visual acuity, confrontational visual fields, extraocular movements, pupillary reactions, lids and adnexa, conjunctiva and sclerae, cornea, anterior chamber, iris, lenses, vitreous, intraocular pressure, and fundoscopic examination."
- Tintinalli's Emergency Medicine
Exception: For chemical ocular burns, irrigation takes absolute priority before any assessment of visual acuity.
1. History
Before the physical exam, a structured history is taken:
- Symptom category: Vision loss, change in appearance, eye pain/discomfort, or trauma
- Onset: Sudden vs. gradual; duration; circumstances
- Character of discomfort: Aching/throbbing (pain), itching (allergy), foreign body sensation (corneal abrasion/ulcer)
- Specific symptoms: "Flashing lights" and a "curtain/veil" suggest retinal detachment; "floaters" suggest vitreous pathology
- Trauma mechanism: Hammering, grinding, or high-speed machinery can cause globe penetration
- PMH: Diabetes, hypertension, previous eye surgery, contact lens use (especially extended wear - associated with bacterial corneal ulcers), current medications
2. Visual Acuity
Visual acuity is the vital sign of the eye - it is always tested first, even before shining a light (bright light can temporarily reduce acuity).
Methods:
| Situation | Tool | Distance |
|---|---|---|
| Standard | Snellen chart | 20 ft (6 m) |
| Near | Rosenbaum chart | 14 inches (36 cm) |
| Children (pre-literacy) | Allen chart (pictures) | Variable |
- Test each eye separately with the opposite eye covered
- Use corrective lenses/contacts if available
- If lenses unavailable: use pinhole testing - the pinhole allows only parallel rays to fall on the macula, correcting most refractive errors
- Record as 20/x (e.g., 20/40-2 means 2 letters missed on the 20/40 line)
If chart reading is not possible, record qualitatively:
- CF - Counting fingers
- HM - Hand motion
- LP - Light perception
- NLP - No light perception
3. Visual Field Testing (Confrontation)
- Patient covers one eye; examiner covers their own opposite eye
- Examiner holds fingers in four quadrants and asks the patient to indicate when they see movement
- Confrontation is the bedside method - it is unreliable for subtle defects but can detect gross field loss
- Scotoma = retinal problem
- Glaucoma - may cause crescent-shaped scotomata, binasal field loss, or loss of all peripheral vision
- Hemi/quadrantanopia = neural pathway problem (optic tract, cortex)
4. External Examination
Inspect both eyes simultaneously for gross abnormalities - compare sides.
Lids and Adnexa:
- Ptosis (CN III palsy, Horner syndrome, myasthenia)
- Periorbital edema, erythema (cellulitis, allergy)
- Lagophthalmos (inability to close the lid - risk of exposure keratopathy)
- Crepitus = subcutaneous emphysema (suggests blow-out fracture of the medial orbital wall/ethmoid)
- Evert the upper eyelid to check for foreign bodies
Globe Position:
- Exophthalmos (proptosis): Forward displacement - causes include thyroid eye disease, orbital cellulitis, tumors, retrobulbar hemorrhage
- Enophthalmos: Posterior displacement - may follow blow-out fracture
- Orbital compartment syndrome - most dangerous cause of exophthalmos; stretches optic nerve + retinal artery; may cause RAPD and limited eye movement
Conjunctiva and Sclera:
- Injection (redness), chemosis (subconjunctival oedema), discharge
- Follicles = allergic or viral conjunctivitis
- Hypopyon (pus in anterior chamber), hyphema (blood in anterior chamber)
- Subconjunctival hemorrhage
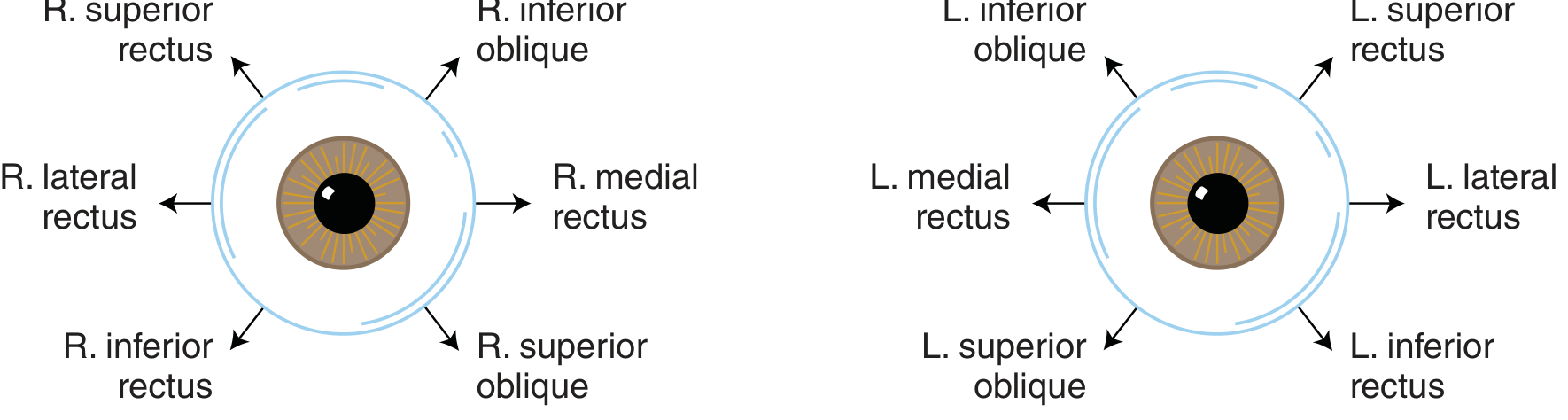
5. Extraocular Movements (EOM)
- Ask patient to follow your finger in an "H" pattern (tests all 6 EOMs)
- Note any limitation of movement or diplopia
| Muscle | Nerve | Action |
|---|---|---|
| Medial rectus | CN III | Adduction |
| Superior rectus | CN III | Elevation in abduction |
| Inferior rectus | CN III | Depression in abduction |
| Inferior oblique | CN III | Elevation in adduction |
| Superior oblique | CN IV | Depression in adduction |
| Lateral rectus | CN VI | Abduction |
- CN VI palsy - inability to abduct (lateral gaze palsy) - most common isolated cranial nerve palsy in diabetes/hypertension
- CN III palsy - ptosis, "down and out" eye, dilated pupil (if compressive, e.g., PComA aneurysm)
6. Pupillary Examination
Examine in both dim and bright light.
Normal findings:
- Equal size (isocoria), round, regular
- Direct and consensual light reflex present
- Accommodation reflex present (miosis when looking at a near object)
Anisocoria:
- Physiological - slight difference (<1 mm), equal in light and dark
- Horner syndrome - miosis + ptosis + anhidrosis (ipsilateral)
- CN III palsy - dilated, unreactive pupil (surgical cause = PComA aneurysm)
- Pharmacological - atropine drops, etc.
Swinging Flashlight Test (Marcus-Gunn Pupil / RAPD):
- Shine a bright light rapidly from one eye to the other
- Normal: both pupils constrict equally
- RAPD (Afferent Pupillary Defect): When light moves to the affected eye, the affected pupil dilates (paradoxical dilation)
- Seen in: optic neuritis, central retinal artery occlusion, severe retinal disease
- Important: RAPD is the only pupillary test that can diagnose unilateral optic nerve disease at the bedside
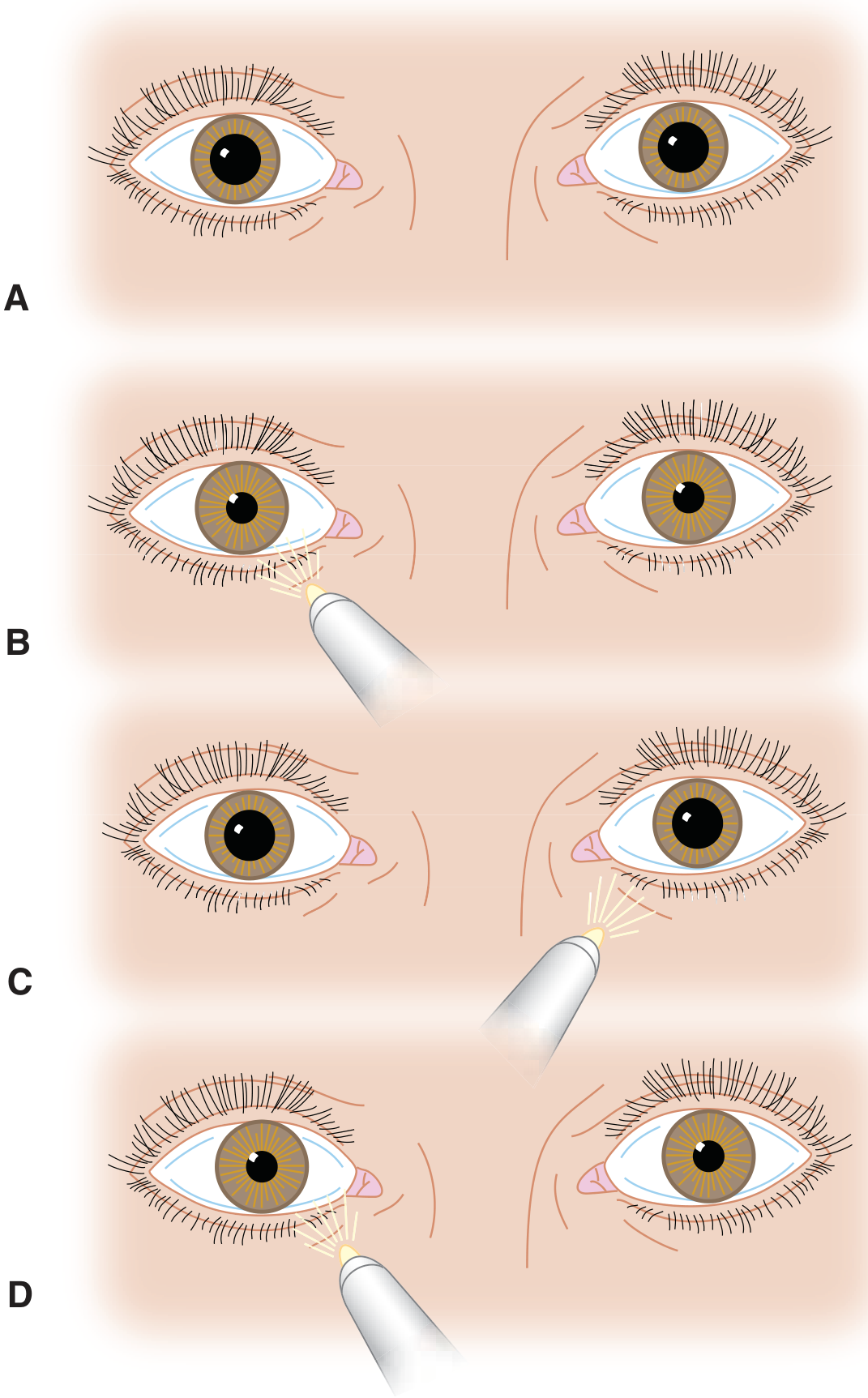
7. Corneal Examination
- Inspect for clarity, ulcers, foreign bodies, abrasions
- Apply topical anaesthetic (proxymetacaine 0.5%) if painful
- Apply fluorescein dye - fluoresces green under cobalt blue light or Wood's lamp
- Corneal abrasion = bright green uptake
- Seidel test - fluorescein streaming = aqueous humor leak through a full-thickness corneal laceration (globe rupture)
- Slit-lamp examination provides magnified view of the cornea, anterior chamber, iris, and lens
8. Anterior Chamber
- Assess depth - shallow chamber = risk of angle-closure glaucoma
- Look for:
- Hyphema - blood in anterior chamber (trauma, bleeding disorders)
- Hypopyon - pus layer in anterior chamber (severe infection/uveitis)
- Flare and cells - seen with slit lamp; indicates uveitis (iritis)
- Penlight oblique illumination can give a rough assessment of depth
9. Lens
- Look for opacities (cataracts) - appear as dark/grey areas in the red reflex or black spots on ophthalmoscopy
- Note clarity and position (lens dislocation after trauma)
10. Intraocular Pressure (IOP) - Tonometry
- Performed near the end (touching the cornea is more irritating)
- Normal IOP: 10-21 mmHg
- Methods:
- Goldmann applanation tonometry - gold standard (requires slit lamp)
- Non-contact (air-puff) tonometry - screening tool
- Tono-Pen - handheld, useful in ED
- Finger palpation - crude bedside method only
- Elevated IOP (>21 mmHg): Acute angle-closure glaucoma, hyphema
- IOP measurement is contraindicated if globe rupture is suspected
11. Fundoscopic Examination
Direct Ophthalmoscopy:
- Dim the room
- Remove your glasses and the patient's glasses
- Approach the patient from 15-20 degrees to the temporal side
- Locate the red reflex first, then advance
- Absent red reflex = cataract, vitreous hemorrhage, retinal detachment, or retinoblastoma (in children)
What to assess on fundoscopy:
| Structure | Normal Findings | Abnormal Findings |
|---|---|---|
| Optic disc | Sharp margins, pink, cup:disc ratio <0.5 | Papilledema (blurred margins, elevated disc), optic atrophy (pale disc), glaucoma (increased C:D ratio) |
| Arteries:Veins ratio | 2:3 | Reduced in hypertension, occlusions |
| AV nicking | None | Hypertensive retinopathy |
| Retina | Uniform, no lesions | Hemorrhages (flame = HTN; dot/blot = DM), exudates (hard = DM; soft/cotton wool = ischemia) |
| Macula | Bright foveal reflex | Macular degeneration, cherry-red spot (CRAO) |
Papilledema:
- Bilateral disc oedema due to raised ICP
- Blurred disc margins, diminished cup, venous engorgement, splinter hemorrhages
- Seen in: malignant hypertension, pseudotumor cerebri, intracranial tumors, hydrocephalus
Pharmacological dilation for better fundoscopy:
- 1% tropicamide (Caucasian patients)
- 1% tropicamide + 2.5% phenylephrine (others)
- Warn patient about blurred vision and photophobia for 4-6 hours
- Contraindicated if acute angle-closure glaucoma is suspected
Summary: RAPD vs Efferent Defect
| Feature | RAPD (Afferent) | Efferent defect (CN III) |
|---|---|---|
| Affected pathway | Optic nerve / retina | Oculomotor nerve (pupilloconstrictor) |
| Swinging flashlight | Paradoxical dilation of affected eye | N/A (test not affected) |
| Direct reflex | Reduced | Absent (fixed dilated pupil) |
| Consensual reflex | Intact in the opposite eye | Absent in affected eye |
Quick Reference: Complete Ocular Exam Checklist
- Visual acuity (Snellen chart / Rosenbaum / Allen)
- Visual fields (confrontation)
- External examination (lids, adnexa, globe position)
- Extraocular movements (H-pattern)
- Pupillary reactions (direct, consensual, RAPD/swinging flashlight test)
- Cornea (fluorescein, slit lamp)
- Anterior chamber (depth, hyphema, hypopyon, flare)
- Iris (pupil shape, synechiae)
- Lens (clarity, position)
- Intraocular pressure (tonometry)
- Fundoscopy (disc, macula, vessels, retina)
Sources: Tintinalli's Emergency Medicine (9th ed.), Rosen's Emergency Medicine, Textbook of Family Medicine (9th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.