behcet disease with cns involvement
Reading File
Finding Sources
Searching PubMed
"Behcet disease" AND "central nervous system"
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
I have comprehensive information to compile a thorough answer. Let me now present the full synthesis.
Neuro-Behcet Disease (CNS Involvement in Behcet Disease)
Overview
Behcet disease (BD) is a multisystemic autoimmune, vascular inflammatory disorder of unknown origin. It is defined by the classic triad of recurrent oral ulcers, genital ulcers, and uveitis, and preferentially affects populations along the ancient Silk Road (Turkey, Middle East, East Asia). CNS involvement - called neuro-Behcet - is one of the most serious and disabling manifestations of the disease.
- Bradley and Daroff's Neurology, p. 1227
Epidemiology and Risk Factors
-
CNS involvement occurs in approximately 20% of Behcet patients overall
-
In children and adolescents, the incidence of neuro-Behcet ranges from 5% to 15%
-
Males predominate among those with neuro-Behcet, especially in pediatric populations
-
In a large Turkish cohort of 728 patients, 3.6% were pediatric; pediatric patients were more likely to have venous sinus thrombosis (88.5%) than parenchymal brain disease (11%), which contrasts with adults
-
Disease is more common in Turkey and other Middle Eastern countries
-
Neurological involvement is a cause of major morbidity; approximately 50% of patients are moderately to severely disabled after 10 years
-
Bradley and Daroff's Neurology, p. 1228; Grainger & Allison's Diagnostic Radiology, p. 1524
Pathophysiology
Neuro-Behcet results from:
- Small vessel inflammatory disease - causing ischemia of brain and spinal cord
- Vasculitis of both arterial and venous systems - associated with thrombosis and arterial aneurysms
- Chronic meningoencephalitis - the most common pathological pattern of CNS involvement
- Dural sinus thrombosis - particularly cerebral venous sinus thrombosis (CVST)
Behcet disease is recognized as a vasculitis that can precipitate cerebral venous thrombosis, alongside other conditions such as pregnancy, oral contraceptive use, and infection.
- Grainger & Allison's Diagnostic Radiology; Bradley and Daroff's Neurology
Clinical Presentations
Parenchymal Neuro-Behcet (most common form in adults)
| Feature | Details |
|---|---|
| Headache | Most common neurological symptom |
| Focal/multifocal neurological signs | Weakness, sensory deficits |
| Brainstem involvement | Frequently involved - diplopia, dysarthria, ataxia |
| Basal ganglia involvement | Movement disorders |
| Meningoencephalitis / aseptic meningitis | 20% of cases |
| Encephalomyelitis | Widespread white matter disease |
| Seizures | Occur, especially in children |
| Pseudotumor cerebri | Raised ICP without mass lesion |
| Cognitive / behavioral changes | Common |
Psychiatric Manifestations
- Depression, psychosis, dementia - part of the recognized neuro-psychiatric spectrum
Vascular Neuro-Behcet
- Cerebral venous sinus thrombosis (CVST) - more common in pediatric patients
- Intracranial hemorrhage - secondary to ruptured aneurysms (rare)
- Ischemic stroke - from small vessel inflammatory vasculopathy
Spinal Cord
- Myelopathy can occur (cord lesions visible on MRI)
Peripheral Nervous System (rare)
-
Polyneuropathy or mononeuropathy multiplex
-
In neuro-otological presentation: vestibular neuronitis
-
Rare case reports of facial nerve paralysis and vocal cord paralysis
-
Bradley and Daroff's Neurology; Grainger & Allison's Diagnostic Radiology, p. 1524
Diagnosis
Clinical Criteria
Definitive diagnosis of Behcet disease requires recurrent oral ulcerations (aphthous or herpetiform) plus two of the following:
- Recurrent genital ulcerations
- Ocular lesions (uveitis or retinal vasculitis)
- Skin lesions (erythema nodosum, pseudofolliculitis, papulopustular lesions, acneiform nodules)
- Positive pathergy test (skin hyperreactivity to a needle prick)
CSF Findings
- Mild pleocytosis (lymphocytic)
- Elevated protein concentration
- Normal or mildly elevated opening pressure
MRI Findings (key imaging modality)
MRI is highly sensitive for neuro-Behcet. Typical findings include:
- Inflammatory parenchymal lesions - typically reversible, located in:
- Brainstem (most characteristic)
- Extension to the diencephalon
- Basal ganglia
- Periventricular and subcortical white matter
- Lesions can occasionally resemble MS plaques
- Brainstem atrophy in chronic/advanced cases
- CVST changes on MRV
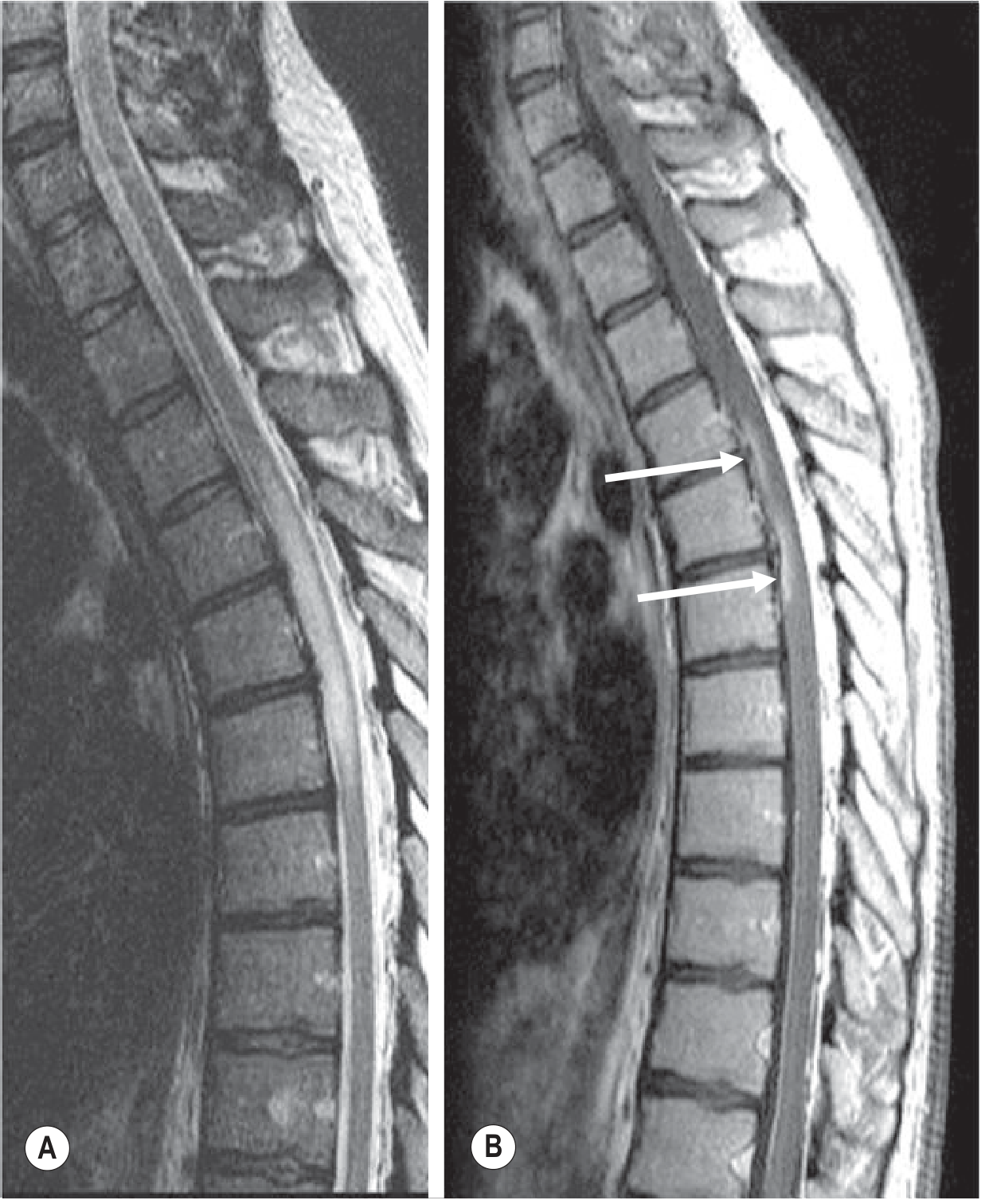
The image below from Grainger & Allison's Diagnostic Radiology shows spinal cord involvement - sagittal MRI (T2 and contrast T1) with a central cord inflammatory lesion:
Differential Diagnosis
Neuro-Behcet must be distinguished from:
-
Multiple sclerosis (lesions can overlap on MRI; look for oral/genital ulcers)
-
Neurosarcoidosis
-
CNS lupus (SLE)
-
Antiphospholipid antibody syndrome
-
CNS lymphoma
-
Cavernous angioma with repeated bleeds
-
Primary angiitis of the CNS (PACNS)
-
Bradley and Daroff's Neurology; Adams and Victor's Principles of Neurology, 12th ed.
Treatment
Acute / Parenchymal Disease
- Corticosteroids are first-line - oral or IV prednisolone until clinical improvement
- High-dose IV methylprednisolone for severe acute attacks
Maintenance / Immunosuppressive Therapy
| Agent | Role |
|---|---|
| Azathioprine | First-choice for severe uveitis and maintenance |
| Methotrexate | Disease-modifying agent |
| Cyclosporine | Used especially for ocular and CNS disease |
| Colchicine | Adjunct for mucocutaneous features |
| Sulfasalazine | Adjunct |
| Interferon-alpha | Used in refractory cases |
| Infliximab (anti-TNF) | Biologic - dramatic results in refractory systemic/CNS disease; supported by EULAR guidelines |
| Other biologics | Adalimumab, tocilizumab in refractory cases |
| Thalidomide | Isolated mucocutaneous disease only |
Cerebral Venous Sinus Thrombosis
-
Anticoagulation is the standard treatment for CVST complicating Behcet disease
-
EULAR guidelines recommend immunosuppression for thrombosis management in addition to anticoagulation
-
Bradley and Daroff's Neurology, p. 1228; Murray & Nadel's Respiratory Medicine; Braunwald's Heart Disease
Key Distinguishing Points for Neuro-Behcet
- Brainstem predominance - unlike most other vasculitides, Behcet has a predilection for the brainstem
- Lesions are often reversible - especially with early immunosuppression, unlike MS which tends to leave permanent damage
- CVST is more common in younger patients - especially pediatric and adolescent males
- Pathergy test positivity supports the diagnosis in the right clinical context
- Eye involvement (uveitis, retinal vasculitis) frequently accompanies CNS disease
Recent Evidence (PubMed 2023-2026)
- A 2023 clinical update review (PMID 37345389) on neuro-Behcet covers diagnostic and treatment updates
- A 2025 review on uncommon non-MS CNS demyelinating disorders (PMID 40591029) includes Behcet as a key differential in demyelinating-like presentations
These reviews are consistent with the textbook content above and do not contradict established management principles.
This is a shared conversation. Sign in to Orris to start your own chat.