M pattern and st depression noted in ? Patient is old and not a known case of htn
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Searching the Web
ECG "M pattern" OR "spade pattern" apical hypertrophic cardiomyopathy ST depression elderly non-hypertensive
Reading File
Reading File
Now I have all the information I need. Let me provide a comprehensive, well-structured answer.
ECG "M Pattern" + ST Depression in an Elderly, Non-Hypertensive Patient
The clinical scenario you describe - M pattern on ECG with ST depression, in an elderly patient without known hypertension - is the classic presentation of Apical Hypertrophic Cardiomyopathy (Apical HCM / Yamaguchi syndrome).
Here is the full breakdown:
What is the "M Pattern" in this context?
The "M pattern" refers to the bifid or notched R wave appearance seen in the mid-precordial leads (V4-V6) in apical HCM. When combined with deep, giant negative T waves in the same leads (V3-V6), the R wave and its flanking components visually create an "M-shaped" morphology on the ECG tracing. This is the hallmark of the apical variant of HCM.
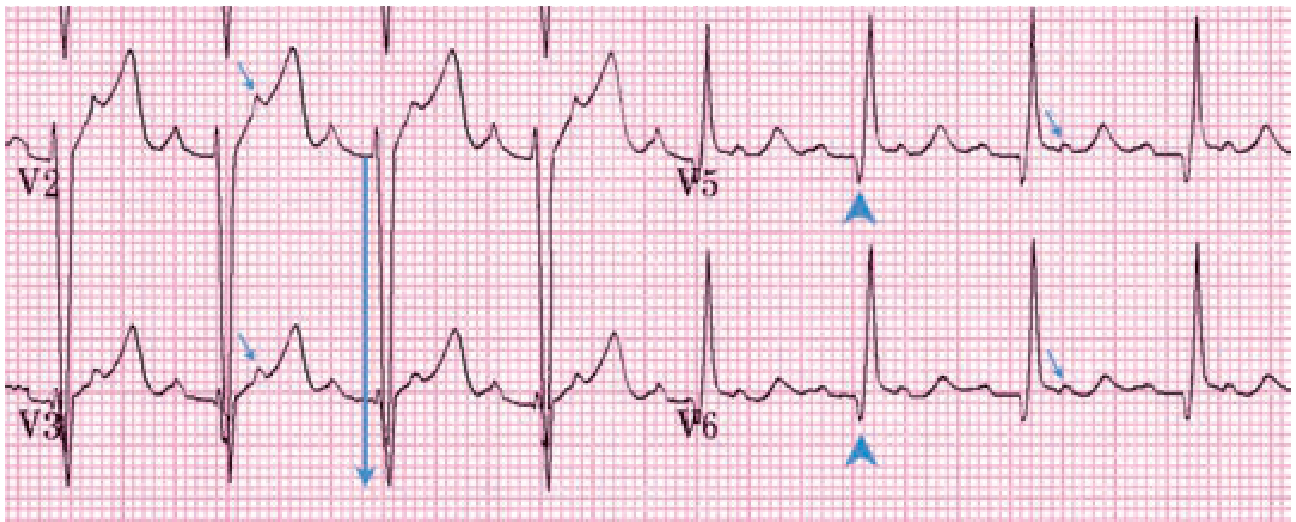
Classic HCM ECG: Large QRS voltage (LVH), septal Q waves in V5-V6 with upright T waves (arrowheads), and additional P waves in ST segments from atrial flutter (arrows) - Tintinalli's Emergency Medicine
Why is the Answer "Apical HCM"?
| Feature | Explains Why |
|---|---|
| M pattern / bifid R wave in V4-V6 | Hypertrophied apical muscle generates abnormal mid-precordial forces |
| ST depression | Part of the "LVH strain pattern" from massive apical hypertrophy; mimics subendocardial ischemia |
| Giant negative T waves (Yamaguchi pattern) | Pathognomonic - negativity ≥1.0 mV in precordial leads V3-V5; reflects distal/apical thickening |
| Elderly patient | Apical HCM has a later mean presenting age (~41-60s) compared to classic HCM; sigmoidal/apical thickening is relatively common in older adults |
| NOT hypertensive | Excludes the most common cause of LVH/ST changes; in a non-hypertensive elderly patient with these ECG findings, apical HCM moves to the top of the differential |
Key ECG Features of Apical HCM
- Giant negative T-wave inversion - maximal in V3-V4, ≥10 mm (1 mV) depth (diagnostic criterion)
- Tall R waves in mid-precordial leads (V4-V5) - increased voltage from LVH
- ST depression in V4-V6 - the "strain pattern"
- The tall R + deep negative T in V4-V5 = the characteristic "M-shaped" appearance in that lead
- No significant left ventricular outflow tract obstruction (unlike classic HCM), so no harsh systolic murmur at rest
Pathophysiology
Apical HCM = hypertrophy confined to the distal left ventricle (apex), below the level of the papillary muscles. Because the obstruction is apical rather than outflow-tract-based:
- No LVOTO gradient
- Left ventriculography shows the classic "ace of spades" / "spade-like" LV cavity in diastole
- Apical obliteration in systole from the massively hypertrophied apex
As Goldman-Cecil Medicine states: "The presence of predominantly distal or apical thickening is associated with giant negative T wave inversion, which is maximal in leads V3 and V4."
Differential Diagnosis to Consider
| Condition | Why It Fits / Why It Doesn't |
|---|---|
| Apical HCM | Best fit: elderly, no HTN, M pattern + ST depression |
| Ischemic ST depression | ST depression yes, but M pattern is not typical; no Q waves expected |
| RBBB | rSR' (M pattern) in V1, NOT V4-V6; ST depression is secondary/right-sided |
| LVH due to HTN | Excluded - no known HTN |
| Cardiac amyloidosis | Can mimic HCM in elderly; but ECG shows low voltage, not high voltage |
| Takotsubo cardiomyopathy | ST changes yes, but apical ballooning, not hypertrophy |
Next Steps
- Echocardiography (first-line) - will show asymmetric apical wall thickening, small LV cavity, apical obliteration in systole
- Cardiac MRI - gold standard for defining extent of hypertrophy and fibrosis; superior to echo for apex visualization
- Troponin + coronary angiography if ACS cannot be excluded clinically (apical HCM can mimic NSTEMI)
- Genetic counseling - autosomal dominant; screen first-degree relatives
Sources:
- Goldman-Cecil Medicine, Diagnostic Testing chapter (HCM)
- Braunwald's Heart Disease, Diagnosis and Morphology (HCM)
- Tintinalli's Emergency Medicine, HCM Diagnosis chapter
- Fuster & Hurst's The Heart, 15th Ed., Cardiac Catheterization (HCM)
- Washington Manual of Medical Therapeutics: "The ECG in apical-variant HCM is characterized by large, inverted T waves across the precordial leads"
M pattern noted in with st depression
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.