Give me complete detailed notes on cemetogenesis
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Searching the Web
cementogenesis steps cementoblast differentiation Hertwig epithelial root sheath acellular cellular cementum
Searching PubMed
cementogenesis cementoblast differentiation
Reading Web Page
https://pocketdentistry.com/10-early-tooth-development-root-…
Loading Image
I now have comprehensive information from multiple authoritative sources. Here are the complete detailed notes on cementogenesis:
Cementogenesis - Complete Detailed Notes
1. Definition
Cementogenesis is the process by which cementum - a mineralized, avascular, bone-like connective tissue - is formed on the root surface of the tooth. It begins at the cementoenamel junction (CEJ) and progresses apically as the root grows. Cementum anchors the collagen fibers of the periodontal ligament (PDL) to the tooth root, physically attaching the tooth to alveolar bone.
2. Developmental Prerequisites: Role of Hertwig's Epithelial Root Sheath (HERS)
Before cementogenesis can occur, root formation must be initiated by the Hertwig Epithelial Root Sheath (HERS):
- Once crown formation is complete, the inner and outer enamel epithelia proliferate downward as a double-layered sheet of flattened cells - this is HERS.
- HERS maps out the shape and length of the root(s) and is separated from adjacent connective tissues by a basal lamina on both surfaces.
- HERS induces the peripheral mesenchymal cells of the dental papilla to differentiate into odontoblasts, which then lay down root predentine from inside out.
- Once root dentinogenesis begins, the epithelial cells of HERS lose their continuity - they fragment and pull away from the newly formed root dentin surface.
- The fragmented remnants of HERS persist in the PDL as epithelial rests of Malassez (these can later give rise to odontogenic cysts and tumors).
- Once HERS detaches from the root dentin surface, mesenchymal cells of the dental follicle migrate in and differentiate into cementoblasts, initiating cementogenesis.
3. Origin of Cementoblasts
The dental follicle - the fibrous sac surrounding the enamel organ during tooth development - has three layers:
| Layer | Origin | Fate |
|---|---|---|
| Inner investing layer (adjacent to HERS) | Neural crest (ectomesenchyme) | Differentiates into cementoblasts |
| Intermediate layer | Mesoderm | Becomes fibroblasts of PDL |
| Outer layer (adjacent to alveolar bone) | Mesoderm | Contributes to alveolar bone formation |
The inner layer of the dental follicle is the sole source of cementoblasts. Once cementogenesis has begun, cells of the remaining dental follicle become obliquely oriented and become PDL fibroblasts.
4. The Process of Cementogenesis
Cementogenesis proceeds in an apical direction, beginning at the cervical margin (CEJ) and extending toward the root apex. It occurs rhythmically - periods of active deposition alternate with periods of quiescence, producing visible incremental lines within the tissue.
Step-by-Step Sequence:
- HERS detachment: HERS cells detach from the root dentin surface after the initial layer of root predentine is deposited by odontoblasts.
- Cementoblast differentiation: Inner layer dental follicle cells migrate to the root surface and differentiate into cementoblasts - large cuboidal cells closely resembling osteoblasts.
- Cementoid secretion: Cementoblasts secrete an unmineralized organic matrix called cementoid (precementum), which consists largely of collagen fibrils.
- Mineralization: Cementoid undergoes progressive mineralization (calcification), incorporating hydroxyapatite crystals into the organic matrix.
- Cellular entrapment (in cellular cementum): Some cementoblasts get surrounded and entrapped by the mineralizing matrix - these become cementocytes, residing in lacunae, with their processes extending into canaliculi (much like osteocytes in bone).
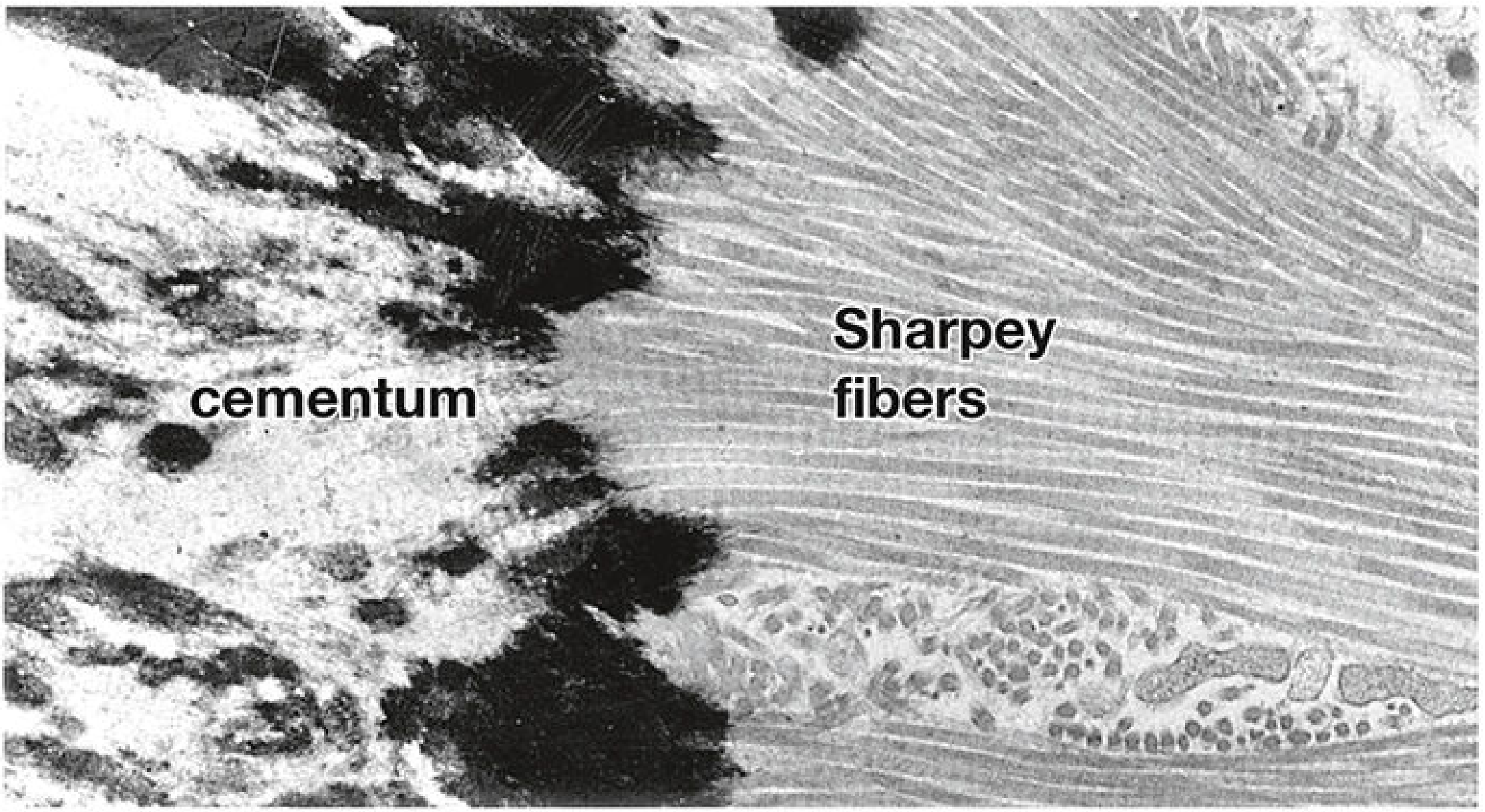
- Periodontal ligament integration: As cementogenesis proceeds, collagen fibers from the PDL become embedded in the mineralizing cementum surface - these are Sharpey fibers (extrinsic fibers), serving as the structural anchors of the tooth.
5. Types of Cementum Formed
Cementum is laid down in two primary forms (acellular and cellular) and five recognized subtypes:
A. Acellular (Primary) Cementum
- Formed first, slowly, at the cervical third of the root.
- No cementocytes are incorporated - cementoblasts remain on the outer surface.
- Deposited very slowly; incremental lines are closely spaced.
- Almost exclusively composed of Sharpey fibers (extrinsic PDL fibers embedded in the matrix).
- This subtype is called Acellular Extrinsic Fiber Cementum (AEFC) - the most important for tooth attachment.
B. Cellular (Secondary) Cementum
- Formed later, more rapidly, at the apical half to two-thirds of the root.
- Formed when cementoblasts are entrapped in the matrix and become cementocytes.
- Incremental lines are more widely spaced (faster deposition).
- Composed of cementocytes, Sharpey fibers (extrinsic), and intrinsic collagen bundles arranged randomly.
- This is Cellular Mixed Stratified Cementum (CMSC) - present at the apical portion.
Five Recognized Subtypes of Cementum (Schroeder classification):
| Type | Cells | Fibers | Location |
|---|---|---|---|
| 1. Acellular afibrillar cementum | No cementocytes | No collagen fibers | CEJ area (thin, superficial) |
| 2. Acellular extrinsic fiber cementum (AEFC) | No cementocytes | Sharpey fibers only | Cervical root (primary attachment) |
| 3. Cellular mixed fiber cementum (CMFC) | Cementocytes | Sharpey fibers + intrinsic fibers | Apical root/furcations |
| 4. Cellular intrinsic fiber cementum (CIFC) | Cementocytes | Intrinsic fibers only | Gap filling / repair |
| 5. Intermediate cementum | Acellular | Thin sheath | Entire root surface, below above types |
6. Structure and Composition of Mature Cementum
- Mineral content: ~65% mineral (hydroxyapatite), similar to bone - but contains the highest fluoride concentration of any mineralized tissue in the body.
- Organic matrix: ~23% collagen (mainly Type I), ~1% non-collagenous proteins (cementum attachment protein - CAP; cementum protein 1 - CEMP1), ~12% water.
- Avascular: Unlike bone, cementum has no blood vessels - cementocytes receive nutrients via canalicular diffusion from the PDL.
- Lacunae: Contains irregularly distributed lacunae housing cementocytes; canaliculi do not form an interconnecting network (unlike bone).
- Sharpey fibers: Collagen fibers of the PDL that penetrate and become mineralized within the cementum; those within the PDL itself remain unmineralized.
7. Key Regulatory Molecules
Cementoblast differentiation and cementogenesis are regulated by several signaling molecules:
| Molecule | Role |
|---|---|
| BMP-2, BMP-7 | Stimulate cementoblast differentiation from dental follicle cells |
| Enamel matrix derivatives (EMD - amelogenin) | Promote cementogenesis; used clinically to regenerate cementum |
| Runx2 (Cbfa1) | Transcription factor essential for cementoblast/osteoblast differentiation |
| Osterix (Sp7) | Downstream of Runx2; required for mineralized tissue formation |
| CEMP1 (Cementum Protein 1) | Specific marker of cementoblasts; promotes cementoblast phenotype |
| CAP (Cementum Attachment Protein) | Unique cementum protein; mediates cell adhesion to root surface |
| Wnt signaling pathway | Regulates cementum formation, regeneration, and cementocyte function (recent 2026 review) |
| FGF, IGF | Promote cementoblast proliferation |
| Sclerostin | Inhibits cementoblast proliferation and differentiation |
8. Incremental Nature of Cementogenesis
- Cementum is deposited rhythmically in increments throughout life (continuously deposited, unlike enamel which stops after eruption).
- Incremental lines (resting lines) mark periods of reduced activity - they have higher ground substance and mineral content and lower collagen content than adjacent cementum.
- Incremental lines in acellular cementum are closely spaced; those in cellular cementum are wider apart.
- The periodicity may be annual and has forensic utility in estimating age from dental histology.
9. Differences Between Cementum and Bone
| Feature | Cementum | Bone |
|---|---|---|
| Vascularity | Avascular | Vascular |
| Resorption | Resistant to resorption (orthodontic forces resorb bone, not cementum) | Resorbs and remodels continuously |
| Canalicular network | Irregular, non-interconnecting | Interconnecting (Haversian system) |
| Haversian canals | Absent | Present |
| Mineral content | ~65% | ~65% (similar) |
| Fluoride content | Highest of all mineralized tissues | Lower |
| Continuous deposition | Yes (throughout life) | Remodels throughout life |
10. Clinical Relevance
- Hypercementosis: Excessive cementum deposition, often at the apex; seen in Paget disease, local irritation, or tooth overloading.
- Ankylosis: Pathologic fusion of cementum with alveolar bone, eliminating the PDL space - can impede orthodontic movement.
- Rests of Malassez: HERS remnants in PDL can give rise to periapical (radicular) cysts, lateral periodontal cysts, and other odontogenic lesions.
- Periodontal regeneration: Procedures using enamel matrix derivatives (Emdogain) aim to recapitulate cementogenesis for regenerating lost periodontal attachment.
- Root resorption: Cementum normally resists resorption; excessive orthodontic force or trauma can cause apical root resorption when this resistance is overcome.
- Age estimation: The incremental lines and cemental annulations of cementum can be used in forensic dentistry to estimate a person's age.
Sources:
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Ross & Pawlina), Cementum section, p. 1452-1453
- Forensic Anthropology: A Comprehensive Introduction, 2nd Ed., Tooth Anatomy section
- Cummings Otolaryngology, Root Development section
- Pocket Dentistry - Cementogenesis
- Histology of Human Cementum (PMC5390338)
- Li T, et al. (2026). Roles of Wnt signaling pathway in cementum formation. J Zhejiang Univ Sci B [PMID: 41847729]
Electron micrograph of Sharpey fibers extending from PDL into cementum (×13,000):
This is a shared conversation. Sign in to Orris to start your own chat.