Bilateral Renal artery stenosis
Reading File
Finding Sources
Searching PubMed
"bilateral renal artery stenosis" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content to produce a thorough answer. Here is the full review:
Bilateral Renal Artery Stenosis (BRAS)
Definition
Renal artery stenosis (RAS) is narrowing of one or both renal arteries, reducing blood flow to the kidney. When both arteries are affected — or when stenosis affects a solitary functioning kidney — it constitutes bilateral renal artery stenosis and carries distinct pathophysiology and management implications compared to unilateral disease.
Causes
| Cause | Frequency | Characteristics |
|---|---|---|
| Atherosclerosis | ~90% | Ostial/proximal location; older patients; male predominance; widespread vascular disease |
| Fibromuscular dysplasia (FMD) | ~10% | Mid-to-distal vessel; "string of beads"; women aged 20–60; bilateral in 25–35% |
| Rare causes | <1% | Aortic dissection, arteritis (Takayasu), emboli, extrinsic compression |
Risk factors for atherosclerotic BRAS mirror general atherosclerosis: hypertension, diabetes, hyperlipidemia, smoking, and advanced age. Most patients have concurrent coronary, cerebral, or peripheral artery disease.
— Goldman-Cecil Medicine, p. 4146
Pathophysiology
The key distinction of bilateral disease lies in how the renin-angiotensin-aldosterone system (RAAS) is activated and suppressed:
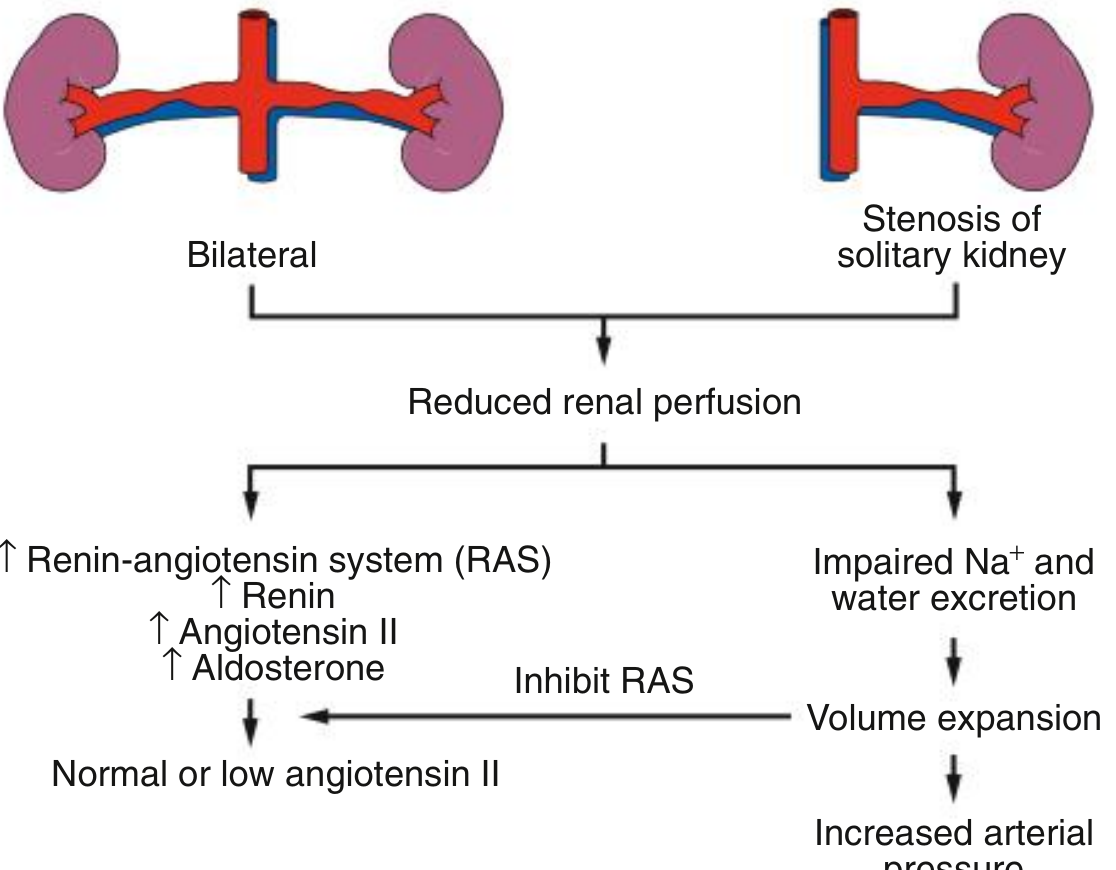
Diagram: In bilateral RAS, reduced perfusion activates RAAS (↑ renin → ↑ angiotensin II → ↑ aldosterone). However, impaired Na⁺ and water excretion from both kidneys causes volume expansion, which then feeds back to suppress renin — resulting in normal or low angiotensin II levels. Hypertension is therefore primarily volume-dependent, not renin-dependent. — Comprehensive Clinical Nephrology, 7th ed.
Key pathophysiologic steps:
- ≥70% stenosis + 20–25% peak systolic pressure gradient → reduced perfusion pressure → juxtaglomerular renin release
- RAAS activation → vasoconstriction, Na⁺ and water retention → hypertension
- In bilateral disease: both kidneys retain Na⁺/water → volume expansion → renin suppression (unlike unilateral disease where the contralateral kidney can excrete the excess)
- Persistent reduced GFR → ischemic nephropathy (chronic kidney disease)
- Non-hemodynamic mechanisms: pro-inflammatory/pro-fibrotic pathways, impaired VEGF expression → pathologic microvascular remodeling (may limit GFR recovery even after revascularization)
— Goldman-Cecil Medicine, p. 4157; Brenner and Rector's The Kidney, p. 2119
Clinical Manifestations
BRAS is often clinically silent; it may be detected incidentally on vascular imaging. When symptomatic, the hallmark presentations are:
Classic "Red Flags" for BRAS/Renovascular Disease (Box 47.2)
- Early-onset hypertension (<30 years) or late-onset (>50 years)
- Accelerated or resistant hypertension (inadequately controlled on ≥3 drugs)
- Deterioration of renal function during treated hypertension
- Acute kidney injury precipitated by ACE inhibitor or ARB — hallmark of bilateral disease
- Flash pulmonary edema — recurrent, episodic; most characteristic of bilateral disease
- Progressive renal insufficiency (ischemic nephropathy)
- Refractory congestive heart failure
Syndromes 5–7 (flash pulmonary edema, progressive renal failure, refractory CCF) are most common in patients with bilateral disease. — Brenner and Rector's The Kidney, p. 108
Physical Examination
- Abdominal/flank bruit (present in 46% of renovascular HTN vs. 9% of essential HTN)
- Signs of widespread atherosclerosis
Laboratory Clues
- Rise in creatinine after starting ACEi/ARB (acute drop in GFR due to loss of angiotensin II–dependent efferent arteriolar tone)
- Hypokalemia (secondary hyperaldosteronism)
- Proteinuria
- Normal or low plasma renin activity (in bilateral disease, renin is suppressed by volume expansion)
Diagnosis
Imaging Modalities
| Modality | Sensitivity | Specificity | Notes |
|---|---|---|---|
| Doppler US | Moderate | Moderate | First-line screening; PSV >200 cm/s in main renal artery suggests flow-limiting stenosis; limited by body habitus and bowel gas |
| CT Angiography (CTA) | 64–92% | 92% | Excellent resolution; limited by heavy calcification; radiation + contrast nephrotoxicity |
| MR Angiography (MRA) | 83–100% | 92–97% | Gadolinium-enhanced; avoid in eGFR <30 (nephrogenic systemic fibrosis risk); non-contrast techniques available |
| Conventional arteriography | Gold standard | Gold standard | Invasive; allows simultaneous pressure gradient measurement and intervention |
A peak systolic velocity of 100–200 cm/s in the main renal artery is a common threshold for flow-limiting stenosis on Doppler. — NKF Primer on Kidney Diseases, p. 2661
Additional considerations:
- Small kidney size on imaging suggests longstanding ischemia and predicts poor benefit from revascularization
- BOLD-MRI (cortical hypoxia imaging) possible but not in routine clinical use
- Radionuclide (nuclear) scan: can assess split renal function and detect captopril-provoked GFR asymmetry
Management
1. Medical Therapy (First-Line for Atherosclerotic BRAS)
Medical management is the preferred therapeutic approach for the majority of patients with atherosclerotic BRAS. The CORAL trial confirmed no significant benefit of stenting over optimal medical therapy in most patients.
Best medical therapy includes:
- Antihypertensives: ACEi or ARB (preferred — also have renoprotective effects, but monitor creatinine carefully); calcium channel blockers as alternatives
- Statins — lipid-lowering; plaque stabilization
- Aspirin 75–100 mg/day (antiplatelet)
- Smoking cessation
- Blood glucose control in diabetics
⚠️ Important caveat with ACEi/ARB in bilateral RAS: Angiotensin II normally maintains GFR by constricting the efferent arteriole in the post-stenotic kidney. Blocking this with ACEi/ARB can precipitate acute kidney injury. Monitor creatinine and potassium closely when initiating — a rise ≤30% is generally acceptable; a larger rise warrants stopping. Despite this concern, ACEi/ARBs remain recommended with careful monitoring.
2. Revascularization (Percutaneous or Surgical)
Indications for revascularization (bilateral disease — more compelling than unilateral):
| Indication | Comment |
|---|---|
| Recurrent flash pulmonary edema | Strongest indication; volume-mediated, refractory to medical therapy |
| Progressive renal failure despite optimal therapy | Attempting to salvage function |
| Severe refractory hypertension | Uncontrolled on ≥3 drugs |
| FMD (any laterality) | Angioplasty alone (no stent usually needed); 35–70% cure/improvement rate |
Techniques:
- Percutaneous transluminal angioplasty (PTA) + stenting — preferred for ostial atherosclerotic lesions (stenting reduces restenosis rate vs. angioplasty alone in atherosclerotic disease)
- Surgical revascularization — aortorenal bypass; reserved for complex anatomy or failed percutaneous approach
- FMD: angioplasty alone (stenting generally not required)
3. Prognosis
- Atherosclerotic BRAS = manifestation of severe systemic vascular disease → markedly increased risk for cardiac and cerebrovascular ischemic events
- Renal function may not significantly recover even after successful revascularization due to microvascular remodeling and fibrosis
- FMD prognosis depends on BP control and severity of disease in other vascular beds
Summary Table: Unilateral vs. Bilateral RAS
| Feature | Unilateral RAS | Bilateral RAS |
|---|---|---|
| Renin/angiotensin | Elevated | Normal or low |
| Mechanism of HTN | Renin-mediated | Volume-mediated |
| Contralateral kidney | Compensates | Cannot compensate |
| ACEi/ARB effect on GFR | Generally safe | Risk of acute GFR drop |
| Flash pulmonary edema | Uncommon | Classic presentation |
| Ischemic nephropathy | Uncommon | Characteristic |
| Captopril renogram | Lateralization | No lateralization |
Sources: Goldman-Cecil Medicine, pp. 4135–4393 | Brenner and Rector's The Kidney, pp. 88–600 | Comprehensive Clinical Nephrology, 7th ed., pp. 2895–2930 | NKF Primer on Kidney Diseases, 8th ed., pp. 2655–2682
This is a shared conversation. Sign in to Orris to start your own chat.