Describe in detail opportunistic infections in HIV.
Reading File
Finding Sources
Searching PubMed
"opportunistic infections" AND "HIV" AND "AIDS"
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed to write a comprehensive, detailed response. Here it is:
Opportunistic Infections in HIV/AIDS
Overview and Pathophysiology
Opportunistic infections (OIs) are the hallmark of advanced HIV disease. HIV selectively destroys CD4+ T lymphocytes (T-helper cells), which are central to coordinating both cellular and humoral immunity. As the CD4+ count declines, pathogens that are normally held in check by intact immunity - latent organisms already harbored in the body, or environmental microbes of low virulence - gain the opportunity to cause life-threatening disease. AIDS is defined as either a CD4+ count below 200 cells/µL or the presence of one or more AIDS-defining OIs, regardless of CD4 count.
- Adams and Victor's Principles of Neurology, 12th Ed., p. 765
The progressive depletion of CD4+ T cells also disrupts B-cell function. HIV-infected patients often have polyclonal hypergammaglobulinemia yet fail to mount protective antibody responses to encapsulated bacteria (e.g., Streptococcus pneumoniae), making them vulnerable to a broader range of pathogens than classic T-cell deficiency alone would predict.
- Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed.
CD4 Count Thresholds and OI Risk
The specific pathogens causing OIs are broadly stratified by CD4+ count. This is one of the most clinically useful frameworks:
| CD4+ T Cell Count | Predominant Opportunistic Infections |
|---|---|
| < 500/µL | Recurrent bacterial infections (S. pneumoniae, H. influenzae), TB reactivation, VZV |
| 200-350/µL | Pneumococcal pneumonia, TB (increased severity), oral candidiasis begins |
| < 200/µL | Pneumocystis jirovecii pneumonia (PJP), esophageal candidiasis |
| < 100/µL | Toxoplasma gondii encephalitis, Cryptococcus neoformans meningitis, disseminated histoplasmosis, coccidioidal meningitis |
| < 50/µL | CMV retinitis, disseminated Mycobacterium avium complex (MAC), primary CNS lymphoma |
- Symptom to Diagnosis, 4th Ed., p. 88
The following figure from Harrison's illustrates the dramatic decline in OI incidence after the introduction of highly active antiretroviral therapy (HAART) in 1996-1997:
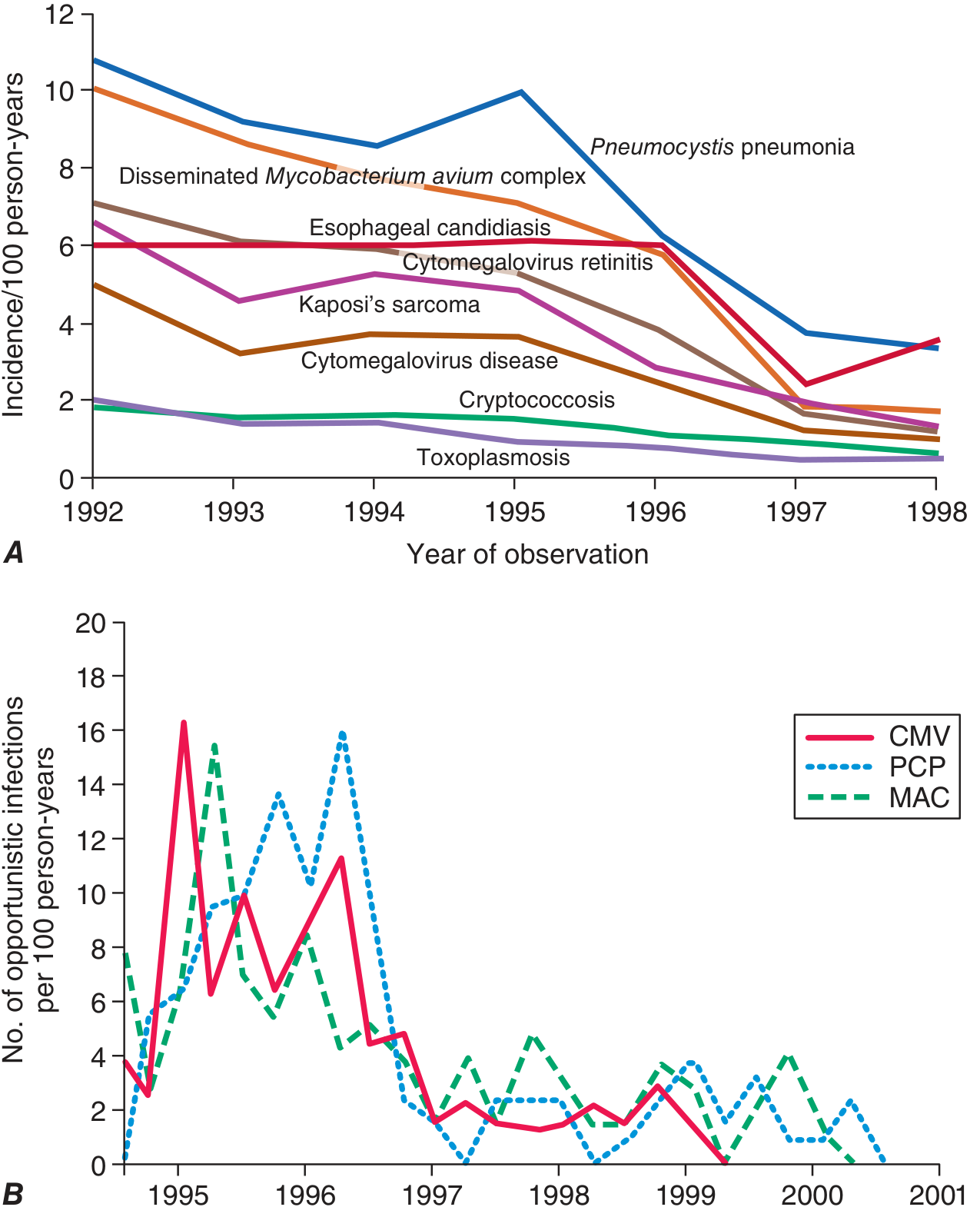
A: Incidence trends 1992-1998 for major OIs. B: Quarterly rates of CMV, PCP, and MAC 1995-2001, showing marked decline after HAART became available.
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Fig. 208-34
Major Opportunistic Infections - Detailed Coverage
1. Pneumocystis jirovecii Pneumonia (PJP / formerly PCP)
Pathogen: Pneumocystis jirovecii (previously P. carinii), an atypical fungus.
CD4 threshold: Occurs predominantly when CD4+ < 200/µL. Primary prophylaxis is initiated at this level.
Clinical features: Subacute onset of progressive dyspnea, non-productive cough, fever, and hypoxia. The chest X-ray classically shows bilateral interstitial ("ground-glass") infiltrates, though it can be normal early. LDH is typically elevated. BAL demonstrating the organism is diagnostic.
Treatment: Trimethoprim-sulfamethoxazole (TMP-SMX) is the treatment of choice. Alternatives include pentamidine isethionate (IV), trimetrexate + leucovorin ± dapsone, or clindamycin + primaquine. Adjunctive corticosteroids are used when PaO2 < 70 mmHg.
Prophylaxis: TMP-SMX (first-line), dapsone ± pyrimethamine + leucovorin, aerosolized pentamidine, or atovaquone. Prophylaxis can be discontinued once CD4+ count is durably > 200/µL on ART.
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed., Table 48-7
- Goodman & Gilman's Pharmacological Basis of Therapeutics
A 2025 network meta-analysis (PMID 39732393) confirmed that TMP-SMX remains the most effective first-line treatment regimen for PJP in people living with HIV.
2. Toxoplasma gondii Encephalitis
Pathogen: Toxoplasma gondii (an intracellular protozoan), almost always representing reactivation of latent infection.
CD4 threshold: CD4+ < 100/µL (most cases < 50-75/µL).
Clinical features: Focal neurological deficits, headache, fever, altered consciousness, and seizures. Contrast-enhanced MRI shows multiple ring-enhancing lesions, often at the gray-white matter junction and basal ganglia. CSF typically shows elevated protein (50-200 mg/dL), and one-third of patients have lymphocytic pleocytosis. Serology: absence of Toxoplasma IgG makes the diagnosis unlikely and favors CNS lymphoma instead.
Key diagnostic challenge: Cerebral toxoplasmosis must be distinguished from primary CNS lymphoma (also ring-enhancing). Empiric treatment with pyrimethamine + sulfadiazine is initiated first; failure to respond radiographically after 2-3 weeks should prompt stereotactic brain biopsy. CNS lymphoma in HIV is associated with EBV.
Treatment: Pyrimethamine (200 mg loading dose, then 50-75 mg/day) + sulfadiazine (4-6 g/day in 4 divided doses) + leucovorin. Alternative: pyrimethamine + clindamycin (for sulfonamide intolerance).
Prophylaxis: TMP-SMX DS once daily (also covers PJP). Secondary prophylaxis continues lifelong unless CD4+ rises durably to > 200/µL on ART.
- Adams and Victor's Principles of Neurology, 12th Ed., p. 767-768
3. Cryptococcus neoformans Meningitis
Pathogen: Cryptococcus neoformans, an encapsulated yeast ubiquitous in soil and pigeon droppings.
CD4 threshold: CD4+ < 100/µL.
Clinical features: Subacute meningitis with headache, fever, malaise, and subtle cognitive changes. Meningismus is often absent. CSF classically shows the organism on India ink preparation; cryptococcal antigen (CrAg) in serum or CSF is the most sensitive test. High CSF opening pressure is common and associated with worse outcomes.
Treatment:
- Induction: Amphotericin B (liposomal or deoxycholate) + flucytosine for at least 2 weeks.
- Consolidation: Fluconazole 400 mg/day for 8 weeks.
- Maintenance (secondary prophylaxis): Fluconazole 200 mg/day indefinitely, or until CD4+ > 100-200/µL for > 3 months on ART with undetectable viral load.
Primary prophylaxis: Not routinely recommended in the United States.
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Table (WHO/CDS.2002 guidelines)
4. Cytomegalovirus (CMV) Disease
Pathogen: CMV (a herpesvirus), almost exclusively reactivation in severely immunocompromised patients.
CD4 threshold: CD4+ < 50/µL for most end-organ disease.
Clinical manifestations:
- Retinitis (most common): Painless, progressive visual loss; fundoscopy shows "pizza pie" or "brushfire" retinal lesions with hemorrhages and exudates. Leading cause of blindness in AIDS patients pre-ART.
- Colitis: Bloody diarrhea, abdominal pain; colonoscopy shows characteristic linear ulcers with submucosal hemorrhage.
- Esophagitis: Odynophagia; large shallow ulcers (vs. the small aphthous ulcers of HSV).
- Pneumonitis: Less common; diffuse bilateral infiltrates.
- Encephalitis: Rare but devastating; subacute cognitive decline, periventricular signal change on MRI.
Treatment: Valganciclovir (oral, preferred for retinitis); IV ganciclovir or foscarnet for severe disease. Ganciclovir intraocular implants were previously used for retinitis.
Secondary prophylaxis: Valganciclovir 900 mg once daily. Can be discontinued if CD4+ > 100/µL for 6 months without active CMV disease.
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed., Table 48-7
5. Mycobacterium tuberculosis (TB)
CD4 threshold: Any level, but severity increases as CD4 falls. Extrapulmonary and disseminated disease are far more common with CD4+ < 200/µL.
Clinical features: TB is the most common OI in HIV globally (particularly in sub-Saharan Africa and Southeast Asia). HIV dramatically expands the TB epidemic. Pulmonary TB is seen in 60-80% of HIV-TB co-infected patients, extrapulmonary in 30-40%. Presentations can be atypical: lower-lobe or diffuse infiltrates, hilar/mediastinal adenopathy, miliary pattern, and extrapulmonary sites (meninges, bone, pericardium, GI tract). Blood cultures are positive in 15% (higher with lower CD4 counts). PPD/IGRA may be falsely negative due to immune suppression.
Treatment: Standard 4-drug therapy (HRZE) for 2 months, then 2-drug continuation (HR) for 4+ months. Rifabutin is often substituted for rifampin due to interactions with antiretroviral drugs. Directly observed therapy is strongly recommended.
ART timing and IRIS: Initiation of ART during TB treatment can provoke immune reconstitution inflammatory syndrome (IRIS) - clinical deterioration as immunity recovers. For most patients, ART should be started 2-8 weeks after beginning TB therapy; for those with CD4+ < 50/µL, start ART as soon as possible (within 2 weeks).
Prophylaxis: 12 weeks of once-weekly isoniazid + rifapentine (3HP regimen) for latent TB in patients with positive TST (≥5 mm) or positive IGRA.
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
6. Mycobacterium avium Complex (MAC)
CD4 threshold: CD4+ < 50/µL (average CD4 at diagnosis is ~10/µL).
Source: Environmental organisms (soil, water) with no person-to-person transmission; portals of entry are GI and respiratory tracts. MAC is common in the United States but rare in Africa, possibly because prior TB exposure reduces susceptibility.
Clinical features: Disseminated disease presenting with fever, drenching night sweats, weight loss, diarrhea, and abdominal pain. Hepatosplenomegaly and lymphadenopathy are common. At least 85% of patients are mycobacteremic. Bone marrow biopsy often shows large numbers of organisms (acid-fast bacilli visible on smear).
Treatment: Two to four drugs, typically: clarithromycin (or azithromycin) + ethambutol ± rifabutin ± ciprofloxacin. Treatment is long-term; discontinuation requires CD4 recovery on ART.
Primary prophylaxis: Azithromycin 1200 mg weekly or clarithromycin 500 mg twice daily when CD4+ < 50/µL. Can be stopped once CD4+ rises to > 100/µL on ART.
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), p. 1545-1546
- Textbook of Family Medicine, 9th Ed.
7. Esophageal and Mucosal Candidiasis
Pathogen: Candida albicans (most common) and other species.
CD4 threshold: Oral/oropharyngeal candidiasis ("thrush") can occur at relatively preserved CD4 counts; esophageal candidiasis, an AIDS-defining illness, typically at CD4+ < 100/µL.
Clinical features:
- Oral candidiasis: White plaques easily scraped from buccal mucosa, erythematous form (angular cheilitis), or pseudomembranous form.
- Esophageal candidiasis: Odynophagia and dysphagia; diagnosis is clinical + response to empiric antifungal therapy. Endoscopy shows white plaques on erythematous mucosa.
Treatment: Fluconazole (oral or IV). Esophageal candidiasis: 14-21 days fluconazole 100-200 mg/day. Refractory cases: itraconazole, voriconazole, or echinocandins.
Prophylaxis: Secondary prophylaxis (fluconazole 100-200 mg/day) for frequent/severe recurrences; primary prophylaxis not routinely recommended.
8. Progressive Multifocal Leukoencephalopathy (PML)
Pathogen: JC virus (John Cunningham polyomavirus), a ubiquitous human pathogen that reactivates in the severely immunocompromised.
CD4 threshold: CD4+ < 100/µL (usually < 50/µL).
Clinical features: Progressive demyelinating disease of the white matter causing focal neurological deficits - hemiparesis, visual field defects, ataxia, aphasia, and cognitive decline. MRI shows non-enhancing white matter lesions in subcortical areas (typically sparing the cortex). There is no ring enhancement and no mass effect (unlike toxoplasmosis). CSF PCR for JC virus is diagnostic.
Treatment: No specific antiviral therapy is effective. ART-mediated immune recovery is the only treatment; prognosis is poor but some patients stabilize with immune reconstitution. ART-associated IRIS can paradoxically worsen PML initially.
- Adams and Victor's Principles of Neurology, 12th Ed., Table 32-2
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed., Table 48-7
9. Histoplasmosis and Coccidioidomycosis
Histoplasma capsulatum causes disseminated disease in HIV patients in endemic areas (Ohio/Mississippi river valleys, Central and South America). Presents with fever, weight loss, hepatosplenomegaly, and skin lesions. Urine antigen is highly sensitive. Treatment: amphotericin B (induction), then itraconazole for consolidation/maintenance. Prophylaxis: itraconazole 200 mg twice daily for CD4+ < 150/µL in endemic areas.
Coccidioides immitis causes disseminated or meningeal coccidioidomycosis in endemic areas (southwestern US, Mexico). Requires fluconazole 400 mg/day for prophylaxis in seropositive patients with CD4+ < 250/µL in endemic regions. Meningeal disease may require lifelong fluconazole.
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), prophylaxis table
10. Herpes Simplex and Varicella-Zoster Virus
HSV: Causes severe, chronic, non-healing mucocutaneous ulcers (oral, genital, perianal), esophagitis, and rarely encephalitis in HIV. Bronchial ulceration is another AIDS-defining manifestation. Treatment: acyclovir, famciclovir, or valacyclovir. Foscarnet for acyclovir-resistant strains. Secondary prophylaxis: valacyclovir 500 mg twice daily (or acyclovir 400 mg twice daily) for frequent/severe recurrences.
VZV: Dermatomal zoster (shingles) is common even at relatively preserved CD4 counts and serves as an early clinical marker of HIV. Disseminated VZV - affecting multiple dermatomes or visceral organs - occurs at lower CD4 counts. Focal vasculitis and encephalitis from VZV are recognized CNS complications of HIV/AIDS. Treatment: acyclovir or valacyclovir; IV acyclovir for severe/disseminated disease.
11. Bacillary Angiomatosis (Bartonella)
Pathogen: Bartonella henselae and Bartonella quintana. Occurs primarily with CD4+ < 200/µL.
Clinical features: Red-to-violaceous vascular papules, nodules, and plaques that may mimic Kaposi sarcoma, cherry angiomas, or pyogenic granulomas. Dissemination can cause osseous lesions, lymphadenopathy, and visceral disease (hepatic peliosis, splenomegaly).
Diagnosis: Tissue biopsy with Warthin-Starry silver stain shows clusters of organisms.
Treatment: Erythromycin 500 mg four times daily or doxycycline 100 mg twice daily for at least 4 weeks. Lifelong secondary prophylaxis may be needed for recurrent disease.
- Fitzpatrick's Dermatology, Vol. 1-2
12. Oral Hairy Leukoplakia (EBV)
Asymptomatic, corrugated white plaques on the lateral tongue caused by EBV infection of mucosal epithelium in immunosuppressed patients. Lesions cannot be scraped off (distinguishing them from candidiasis). Treatment is not required - ART usually leads to resolution. HIV-related EBV associations also include high-grade B-cell lymphomas (Burkitt lymphoma, diffuse large B-cell lymphoma, primary CNS lymphoma).
- Fitzpatrick's Dermatology, Vol. 1-2, p. 3143
13. Recurrent Bacterial Infections
Streptococcus pneumoniae, Haemophilus influenzae, Staphylococcus aureus, and Salmonella species all cause increased rates of invasive disease in HIV. Recurrent bacteremia with Salmonella species is an AIDS-defining condition. Polyclonal B-cell activation impairs specific antibody responses. Pneumococcal and other bacterial vaccines are recommended for all HIV-positive patients, though their effectiveness is reduced at lower CD4 counts.
Prophylaxis Summary
The table below summarizes primary and secondary prophylaxis recommendations (from the DHHS/WHO guidelines as cited in Harrison's 22nd Ed.):
| Pathogen | Indication | First-Line Prophylaxis |
|---|---|---|
| P. jirovecii | CD4+ < 200/µL | TMP-SMX DS 1 tab/day |
| T. gondii | CD4+ < 100/µL + positive IgG | TMP-SMX DS 1 tab/day |
| M. avium complex | CD4+ < 50/µL | Azithromycin 1200 mg/week |
| M. tuberculosis (latent) | TST ≥5 mm or +IGRA | Isoniazid + rifapentine ×12 weeks |
| Cryptococcus | Secondary only | Fluconazole 200 mg/day |
| Histoplasma | CD4+ < 150/µL in endemic area | Itraconazole 200 mg twice daily |
| Coccidioides | CD4+ < 250/µL + seropositive in endemic area | Fluconazole 400 mg/day |
| Bartonella | Secondary only | Doxycycline 200 mg/day |
| CMV | Secondary only | Valganciclovir 900 mg/day |
| HSV | Frequent/severe recurrences | Valacyclovir 500 mg twice daily |
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
Impact of ART
The introduction of HAART in 1996-1997 transformed OI management. A 20-year-old with HIV on modern ART can now expect to live more than 50 additional years. In countries with ART access, AIDS-related illnesses account for only ~25% of deaths in HIV-infected patients - non-AIDS malignancies, cardiovascular disease, and liver disease now dominate. However, OIs remain major killers in sub-Saharan Africa and other resource-limited settings, where roughly 80% of HIV-infected individuals live.
The key principle in managing all OIs is:
- Treat the acute OI with appropriate pathogen-directed therapy.
- Initiate or optimize ART as soon as it is safe to do so (with attention to IRIS timing).
- Maintain prophylaxis until CD4 counts recover durably.
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025) - McGraw Hill
- Adams and Victor's Principles of Neurology, 12th Ed. - McGraw Hill
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed.
- Fitzpatrick's Dermatology, Vols. 1-2
- Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed.
- Textbook of Family Medicine, 9th Ed.
- Recent PubMed evidence: PMID 39732393 (PJP treatment network meta-analysis, Clin Microbiol Infect 2025), PMID 38583518 (PJP prophylaxis network meta-analysis, Clin Microbiol Infect 2024)
This is a shared conversation. Sign in to Orris to start your own chat.