Terminal respiratory units Full details for md exam answer 10 marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive material. Let me compile the full 10-mark MD exam answer.
Terminal Respiratory Units (TRU) - Full MD Exam Answer
Definition
The terminal respiratory unit (TRU), also called the acinus or primary lobule, is defined as the aggregation of all airways and alveolar structures arising from a single terminal bronchiole - specifically, the respiratory bronchioles, alveolar ducts, alveolar sacs, and their accompanying alveoli, together with their associated blood vessels and lymphatics.
The functional definition is equally important: because gas-phase diffusion within the TRU is so rapid, the partial pressures of O2 and CO2 are effectively uniform throughout the entire unit at any given moment. This distinguishes the TRU from the conducting airways where convective flow creates concentration gradients.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 36 (Key Points)
Structural Components and Airway Generations (Weibel's Model)
The human lung has approximately 23 generations of airways. The TRU encompasses generations 17-23:
| Zone | Airway | Generations | Function |
|---|---|---|---|
| Conducting | Trachea → bronchi → bronchioles → terminal bronchioles | 0-16 | Conduction only (dead space) |
| Transitional | Respiratory bronchioles (RBL) | 17-19 | Partial gas exchange (alveoli bud from walls) |
| Respiratory | Alveolar ducts (AD) | 20-22 | Full gas exchange |
| Respiratory | Alveolar sacs (AS) | 23 | Full gas exchange |
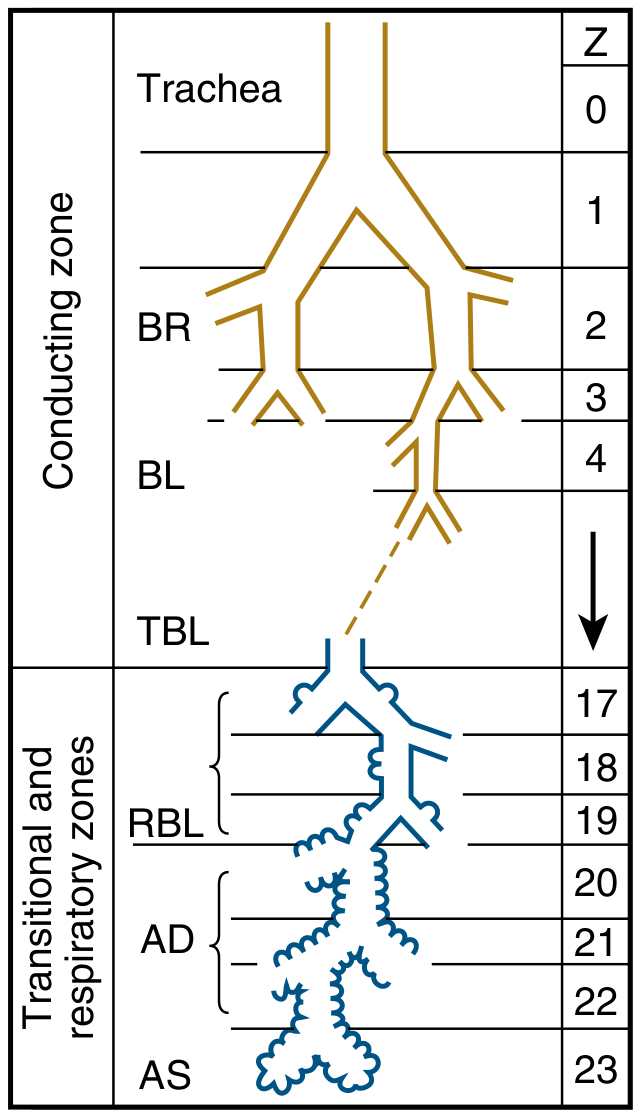
Weibel's model A: conducting zone (gold) vs. transitional and respiratory zones (blue). The TRU begins at generation 17.
Key dimensions:
-
Each TRU contains approximately 100 alveolar ducts and ~2,000 alveoli
-
The distance from terminal bronchiole to the most distal alveolus is only about 5 mm
-
The respiratory zone makes up most of the lung's gas volume: ~2-3 L
-
Total alveoli in both lungs: ~300 million, with a combined surface area of 50-100 m²
-
Individual alveolar diameter: 75-300 µm (varies with inflation)
-
Murray & Nadel's Textbook of Respiratory Medicine, p. 36-37
Cellular Components of the TRU
The TRU is composed of several specialized cell types, all visible on electron microscopy:
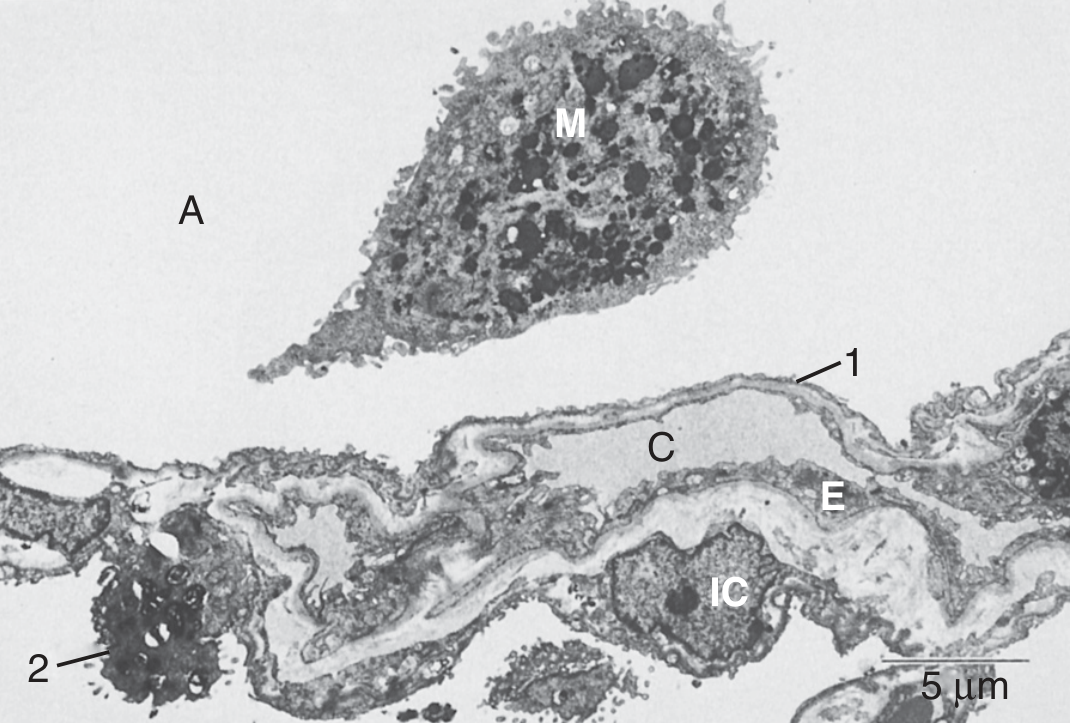
Figure: Cells of the TRU. Alveolar macrophage (M) in air space (A); type 1 (1) and type 2 (2) pneumocytes lining the wall; capillary (C), endothelial cells (E), interstitial cells/fibroblasts (IC). (Murray & Nadel, Fig. 1.27)
1. Alveolar Type 1 Cells (AT1 / Pneumocyte Type I)
- Large, squamous/flat cells with extensive attenuated cytoplasmic processes
- Cover 90-95% of the alveolar surface area, though they are numerically fewer (~8-10% of peripheral lung cells)
- Extremely thin (wall thickness 0.15-0.30 µm at thinnest point) - optimized for gas diffusion
- Express water channels (aquaporins), epithelial sodium channels, and Na+/K+-ATPase - playing a role in pulmonary fluid regulation
- Contain caveolae (non-clathrin-coated vesicles) containing caveolin-1, involved in signal transduction, cholesterol transport, and transcytosis
- Form tight junctions with AT2 cells, creating a relatively impermeable seal between air space and interstitium
- Limited regenerative capacity; vulnerable to injury
2. Alveolar Type 2 Cells (AT2 / Pneumocyte Type II / Granular Pneumocyte)
- Small (~300 µm³), cuboidal cells with stubby apical microvilli
- Numerically more abundant (~15% of peripheral lung cells) but occupy only a small surface area
- Contain lamellar bodies (membrane-bound, osmiophilic inclusions, diameter 0.1-2.5 µm) - the storage organelles for surfactant
- Primary function: synthesis, secretion, and recycling of pulmonary surfactant (phospholipids + surfactant proteins SP-A, SP-B, SP-C, SP-D)
- Surfactant is secreted by exocytosis into the alveolar space, reducing alveolar surface tension and preventing collapse
- Act as facultative stem cells (progenitor cells): can self-renew and differentiate into AT1 cells after injury - critical for alveolar repair
- A subpopulation termed alveolar epithelial progenitors (AEPs), identifiable by the surface marker TM4SF1, rapidly expand after acute lung injury
3. Pulmonary Capillary Endothelial Cells
- Form a near-continuous sheet ("twisted ribbon") between abutting alveoli
- Average capillary internal diameter: ~8 µm
- At the thinnest (fusion) point, the basal laminae of the capillary endothelium and alveolar epithelium fuse, creating the minimal diffusion barrier
- A single pulmonary arteriole supplies all capillaries of one TRU
- The capillary network is a dense, hexagonal anastomosing array
4. Interstitial Cells (Fibroblasts)
- Located in the alveolar wall interstitium between the two basal laminae
- Provide structural support via collagen and elastin synthesis
- Involved in alveolar wall repair
5. Alveolar Macrophages
-
Free-roaming scavenger cells residing in the alveolar air space
-
Remove inhaled particles, microbes, and cellular debris
-
Can be activated to secrete cytokines, modulating inflammation
-
Cleared via the mucociliary escalator or into the interstitium
-
Murray & Nadel's Textbook of Respiratory Medicine, pp. 43-50
The Blood-Gas Barrier
The key structural feature of the TRU enabling gas exchange is the extremely thin blood-gas (air-blood) barrier, consisting of:
- Alveolar lining fluid (surfactant layer)
- AT1 cell cytoplasm
- AT1 cell basal lamina (fused with capillary basal lamina on thin side)
- Capillary endothelial cell cytoplasm
Total thickness of the thin side: ~0.2-0.6 µm (the red blood cell alone contributes a substantial portion of the diffusion pathway given this extreme thinness)
On the thick side of the capillary, the two basal laminae are separated by an interstitial space containing fibroblasts and collagen - this side is important for fluid exchange but not optimized for gas diffusion.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 44; Medical Physiology, p. 876
Gas Transport Within the TRU: Diffusion vs. Convection
A key physiological principle distinguishes the TRU from conducting airways:
-
In conducting airways (generations 0-16): gas movement is by bulk flow (convection)
-
In the TRU: as aggregate cross-sectional area rises steeply, linear velocity falls to near zero. At terminal bronchioles (generation 16), aggregate cross-sectional area is ~180 cm² vs. ~2.5 cm² in the trachea. Gas movement within the TRU is therefore dominated by molecular diffusion
-
This rapid diffusion is why PO2 and PCO2 are uniform throughout the TRU at any moment (the functional definition)
-
Medical Physiology, p. 876; Murray & Nadel's Textbook, p. 219
Surfactant: Role in TRU Stability
Surfactant (produced by AT2 cells) is critical for TRU function:
- Composed primarily of phosphatidylcholine (dipalmitoyl lecithin) plus SP-A, SP-B, SP-C, SP-D
- Reduces alveolar surface tension at the air-liquid interface
- By Laplace's law (P = 2T/r), reduces the tendency of smaller alveoli to collapse
- Prevents alveolar atelectasis at end-expiration
- Also has immunomodulatory functions (SP-A and SP-D are collectins involved in innate immunity)
Deficiency of surfactant is the basis of Neonatal Respiratory Distress Syndrome (NRDS) in premature infants.
Pores of Kohn
Small perforations in the alveolar septa connecting adjacent alveoli. They are:
-
Surrounded by capillaries
-
Allow collateral ventilation between alveoli within the TRU
-
May play a role in preventing atelectasis
-
Medical Physiology, p. 876
Alveolar Dimensions Summary
| Parameter | Value |
|---|---|
| Total alveoli (both lungs) | ~300 million |
| Alveolar surface area | 50-100 m² |
| Alveolar diameter | 75-300 µm |
| Blood-gas barrier thickness (thin side) | 0.15-0.30 µm |
| Capillary diameter | ~8 µm |
| Alveolar ducts per TRU | ~100 |
| Alveoli per TRU | ~2,000 |
| Respiratory zone volume | ~2-3 L |
Clinical Relevance
- NRDS (Hyaline Membrane Disease): AT2 cell immaturity → surfactant deficiency → alveolar collapse → diffuse atelectasis
- ARDS: Injury to AT1 and endothelial cells → breakdown of blood-gas barrier → flooding of TRU with proteinaceous fluid
- Emphysema: Destruction of alveolar walls → loss of TRU surface area → reduced diffusion capacity
- Adenocarcinoma: ~40% of lung cancers arise from components of the TRU (particularly AT2 cells and bronchiolar Clara/Club cells)
- Pulmonary fibrosis: Fibroblast proliferation in TRU interstitium → thickening of blood-gas barrier → diffusion impairment
Summary for Exam
The TRU = terminal bronchiole + respiratory bronchioles (Gen 17-19) + alveolar ducts (20-22) + alveolar sacs (23) + their alveoli and vessels. It is the functional unit of gas exchange where diffusion (not convection) dominates. Its cells are: AT1 (gas exchange, 90-95% surface), AT2 (surfactant, stem cell), endothelium, fibroblasts, macrophages. The blood-gas barrier is ~0.2-0.6 µm. Surfactant prevents collapse. The TRU constitutes most of the lung's volume (~2-3 L) while residing in a space only ~5 mm across.
Sources: Murray & Nadel's Textbook of Respiratory Medicine (9780323655873), pp. 36-50, 219 | Medical Physiology (9780323319737), pp. 875-877
This is a shared conversation. Sign in to Orris to start your own chat.