What are the basic methods of IHC?
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from Junqueira's Basic Histology. Here is a complete answer:
Basic Methods of Immunohistochemistry (IHC)
Immunohistochemistry exploits the highly specific antigen–antibody interaction to identify and localize proteins within tissue sections, viewable under light or electron microscopy. Every IHC technique requires a prior antibody raised against the target protein (antigen).
1. Antibody Types Used
| Type | How produced | Characteristics |
|---|---|---|
| Polyclonal | Protein antigen injected into animal; collected from plasma | Mixture of antibodies binding multiple epitopes of the target |
| Monoclonal | Activated lymphocytes fused with tumor cells → hybridoma clones | Single-epitope specificity; less non-specific background binding |
2. The Two Core Methods
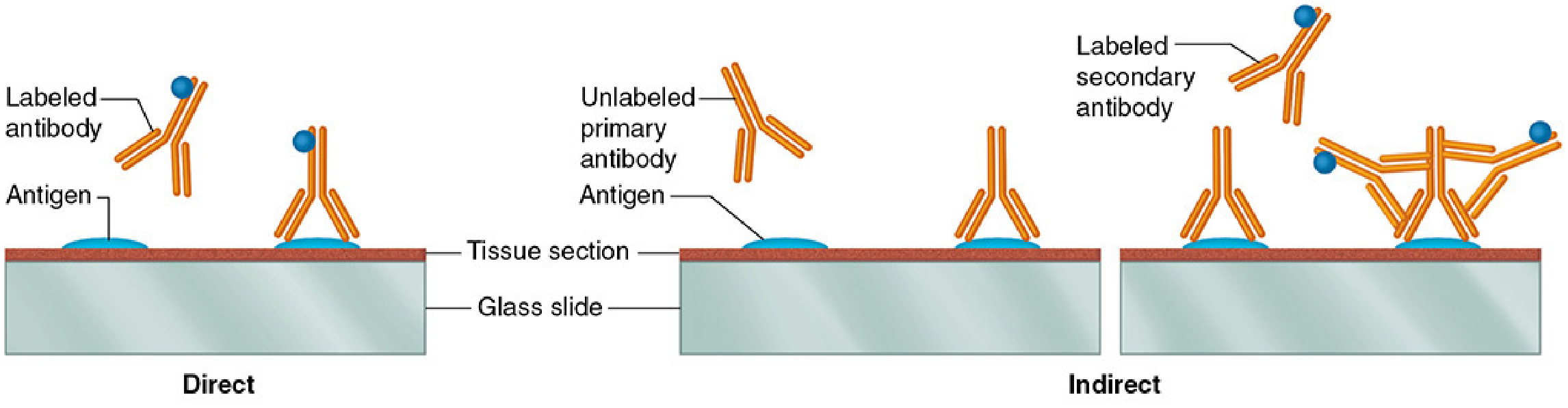
Direct Method
- A labeled primary antibody (specific for the target antigen) is applied directly to the tissue section.
- The label — a fluorescent compound, peroxidase, alkaline phosphatase, or electron-dense gold particles — is conjugated to this single antibody.
- Simple, fast, but less sensitive because only one label molecule is delivered per antigen site.
Indirect Method (more widely used)
- Step 1: An unlabeled primary antibody (specific for the target antigen) is applied to the tissue section and binds its antigen.
- Step 2: A labeled secondary antibody (raised against the immunoglobulin of the primary antibody's host species, and conjugated to a reporter) is applied and binds the primary antibody.
- Because multiple secondary antibody molecules can bind each primary antibody, the signal is amplified — making this method more sensitive than the direct approach.
- The same labeled secondary antibody can be reused with many different primary antibodies (as long as all primaries are from the same host species), making the system economical.
3. Signal Detection / Labels
| Label | Detection method | Microscopy |
|---|---|---|
| Fluorescent dyes (e.g., FITC, rhodamine) | Fluorescence microscopy | Light (fluorescence) |
| Peroxidase (HRP) | Histochemical substrate (e.g., DAB → brown precipitate) | Light |
| Alkaline phosphatase | Chromogenic substrate | Light |
| Colloidal gold particles | Electron-dense spots | Transmission EM (TEM) |
4. Signal Amplification Techniques
Beyond the basic indirect method, further amplification strategies exist:
- Biotin–avidin (or streptavidin) technique: The primary or secondary antibody is biotinylated; avidin (which binds biotin with extremely high affinity) conjugated to a reporter is then applied. Because one avidin molecule can bind multiple biotins, signal amplification is substantial.
- Polymer-based systems (e.g., EnVision): Reporter enzymes are coupled to a polymer backbone attached to the secondary antibody — no biotin interference and stronger signal.
5. Tissue Preparation Considerations
- Formalin-fixed, paraffin-embedded (FFPE) sections are standard; antigen retrieval (heat-induced or enzymatic) is often needed to unmask epitopes crosslinked by fixation.
- Frozen sections preserve antigenicity better but have inferior morphology.
Clinical Applications (from Robbins Pathology)
- Classifying undifferentiated tumors — cytokeratins → carcinoma; desmin → muscle origin; CD45 → hematopoietic malignancy; SOX10 → melanoma.
- Identifying metastatic tumor origin — PSA (prostate), thyroglobulin (thyroid).
- Therapeutic targets — HER2 (breast cancer, trastuzumab eligibility), ALK fusion proteins (lung/lymphoma, ALK inhibitor eligibility), ER/PR receptors (antiestrogen therapy).
Sources: Junqueira's Basic Histology, 17e; Robbins, Cotran & Kumar Pathologic Basis of Disease
Fibrous histiocytoma histology.
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
fibrous histiocytoma dermatofibroma histology microscopy
Excellent — I have rich histological detail from multiple authoritative sources. Here is a comprehensive answer:
Fibrous Histiocytoma — Histology
"Fibrous histiocytoma" (FH) encompasses a spectrum from benign (dermatofibroma) to malignant (undifferentiated pleomorphic sarcoma / UPS). Their histology differs markedly.
Benign Fibrous Histiocytoma (Dermatofibroma)
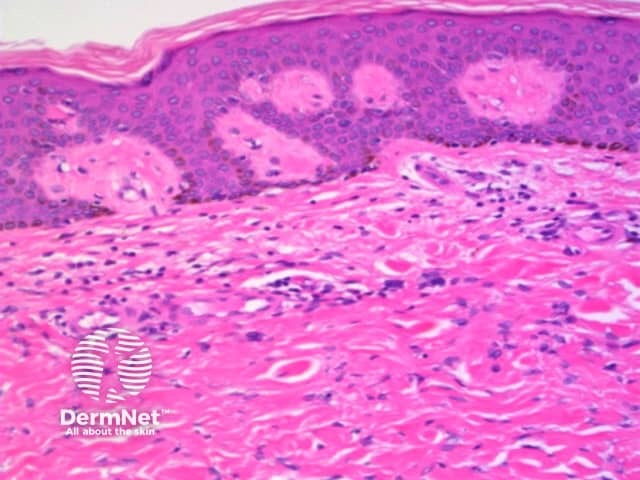
Architecture
- Nonencapsulated, well-defined dermal mass
- Spindle and histiocytic cells arranged in close whorls (storiform / cartwheel pattern)
- Cells entrap individual collagen bundles at the periphery — collagen trapping is characteristic
- May extend into subcutaneous fat
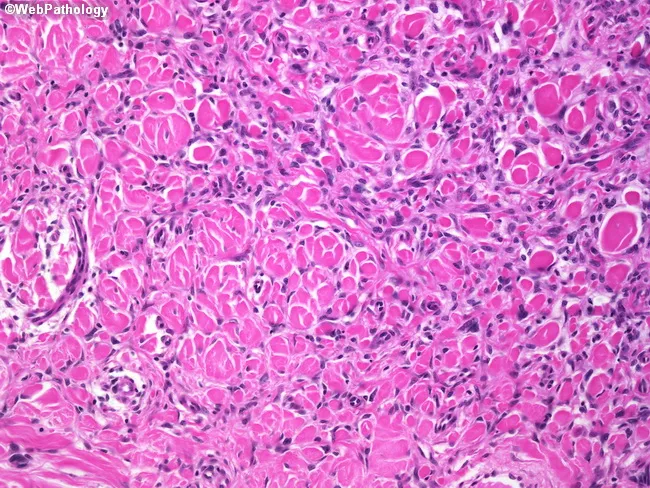
Cytology
- Spindle cells with features of fibroblasts and myofibroblasts (probable primitive mesenchymal origin)
- Bland, elongated nuclei; scant cytoplasm; minimal atypia
- Low mitotic activity
- Occasional foam cells, lipid deposits, and hemosiderin-laden macrophages
- Multinucleated giant cells (including Touton giant cells) may be present
- Touton giant cells + hemosiderin = pathognomonic of dermatofibroma
Epidermal changes
- Overlying acanthosis (pseudoepitheliomatous hyperplasia) with downward elongation of hyperpigmented rete ridges is typical
- Induction of primitive follicular structures or basal cell carcinoma-like changes may overlie the lesion (true BCC is rare)
Variants
| Variant | Feature |
|---|---|
| Aneurysmal | Pools of extravascular blood and hemosiderin |
| Cellular | Increased cellularity |
| Granular cell | Granular cytoplasm predominates |
| Deep/fascial | Extends into fat or muscle via fibrous septa |
| Pigmented | Histologic overlap with Bednar tumor (pigmented DFSP) |
| Monster cell | Large, strikingly atypical histiocytic cells |
Immunohistochemistry
- Positive: Factor XIIIa, CD10
- Negative: MAC387, S-100, CD34 (CD34 negativity is critical — helps distinguish from DFSP)
Malignant Fibrous Histiocytoma → Undifferentiated Pleomorphic Sarcoma (UPS)
(The term "malignant fibrous histiocytoma" has largely been replaced by UPS in current WHO classification)
Architecture
- Spindle and histiocytic cells arranged in a storiform (cartwheel) pattern — short fascicles of cells and fibrous tissue radiate about a common center around slit-like vessels
- Deep fascial plane location (vs. superficial dermis in benign FH)
- Chronic inflammatory cells may be interspersed
Cytology
- Pleomorphic cellular elements — hallmark feature
- Bizarre, multinucleated giant cells
- Atypical (abnormal) mitotic figures
Histologic subtypes
| Variant | Key feature |
|---|---|
| Storiform-pleomorphic | Classic; most common |
| Myxoid (myxofibrosarcoma) | Prominent myxoid stroma; atypical spindle cells; lower metastatic risk |
| Inflammatory | Dense chronic inflammatory infiltrate |
| Giant cell | Prominent osteoclast-like giant cells |
Immunohistochemistry
- Positive: Vimentin, Factor XIIIa
- No specific lineage markers (by definition "undifferentiated")
- S-100 negative (distinguishes from MPNST/melanoma)
Key Distinguishing Features: Benign vs. Malignant FH
| Feature | Benign FH (Dermatofibroma) | Malignant FH (UPS) |
|---|---|---|
| Location | Superficial dermis | Deep fascia/muscle |
| Borders | Non-encapsulated but circumscribed | Infiltrative |
| Atypia | Minimal | Marked pleomorphism |
| Mitoses | Rare, normal | Frequent, atypical |
| Giant cells | Touton type | Bizarre multinucleated |
| Storiform pattern | Present (mild) | Prominent |
| Vimentin | Variable | Positive |
| CD34 | Negative | Negative |
| Factor XIIIa | Positive | Positive |
| Behavior | Benign, rarely recurs | 35% metastasize; 50% OS |
Sources: Andrews' Diseases of the Skin, 13e; Robbins, Cotran & Kumar Pathologic Basis of Disease; Miller's Review of Orthopaedics, 9e
This is a shared conversation. Sign in to Orris to start your own chat.