Make a detailed note on Vancomycin-resistant enterococci (VRE) infection or colonisation on ICU. Make sure to use current guidelines & referrences
Reading File
Finding Sources
Searching PubMed
"vancomycin-resistant enterococci" AND "intensive care unit"
Searching the Web
VRE vancomycin-resistant enterococci ICU guidelines 2024 2025 management infection control
Finding Sources
Finding Sources
Searching PubMed
"vancomycin-resistant enterococci" AND treatment
Searching PubMed
"VRE" AND "infection control" AND screening
Reading File
Finding Sources
Reading Article
Reading Article
Reading File
Reading File
Finding Sources
Reading Article
Reading Article
Reading File
Reading Web Page
VRE ICU screening isolation contact precautions management
Finding Sources
Reading File
Reading File
Finding Sources
I now have comprehensive data. Let me compile the detailed clinical note.
Vancomycin-Resistant Enterococci (VRE): Infection and Colonisation in the ICU
1. Background and Microbiology
Enterococci are Gram-positive, facultatively anaerobic cocci that belong to the normal flora of the human gastrointestinal tract. The two clinically dominant species are Enterococcus faecalis and Enterococcus faecium, the latter being far more problematic in the ICU due to its propensity to acquire resistance.
VRE were first reported in 1988. By 1995 VRE had become endemic in US hospitals. In Europe, the VRE prevalence in E. faecium reached 17.3% (population-weighted mean) by 2018 and is rising, driven partly by the emergence of a hospital-adapted clonal lineage.
Resistance Mechanisms
Vancomycin normally inhibits cell wall synthesis by binding to the D-Ala-D-Ala terminus of peptidoglycan precursors. VRE acquires resistance via van gene clusters carried on mobile genetic elements (plasmids and transposons), allowing plasmid-mediated inter-patient transmission:
| Gene | Resistance level | MIC to vancomycin | MIC to teicoplanin | Common species | Epidemiologic concern |
|---|---|---|---|---|---|
| vanA | High | ≥64 mg/L | ≥16 mg/L | E. faecium, E. faecalis | High (plasmid, transmissible); predominates in USA |
| vanB | Variable (moderate-high) | 4-1024 mg/L | Susceptible | E. faecium, E. faecalis | High (plasmid, transmissible); predominates in Europe |
| vanC | Intrinsic, low-level | 2-32 mg/L | Susceptible | E. gallinarum, E. casseliflavus | Low (chromosomal, non-transmissible) |
Both vanA and vanB are encoded on plasmids, making horizontal gene transfer a critical infection-control concern.
- Tietz Textbook of Laboratory Medicine, 7th Ed.
- Henry's Clinical Diagnosis and Management by Laboratory Methods
2. Epidemiology in the ICU
VRE are a leading cause of healthcare-associated infections (HAI), particularly in high antibiotic-use settings. ICUs carry a disproportionate burden:
- MDRO gut acquisition in ICU patients: pooled incidence 5% (range 1-43%), with an incidence rate of 12.2 per 1000 patient-days (95% CI 8.1-18.6). Colonisation increases quasi-linearly at ~1.41% per day through 30 days of ICU stay. (Heath et al., Critical Care, 2024 - PMID 38943133)
- Among VRE gut carriers, the pooled 30-day cumulative incidence of infection is 8% (95% CI 5-13). (Willems et al., Lancet Infect Dis, 2023 - PMID 36731484)
- VRE bloodstream infection (BSI) is associated with 46% higher mortality compared to vancomycin-susceptible E. faecium BSI (RR 1.46, 95% CI 1.17-1.82). (Eichel et al., J Hosp Infect, 2023 - PMID 37734679)
- VRE bacteraemia carries an in-hospital mortality of ≥20%, approximately twice that of VSE bacteraemia. (Goldman-Cecil Medicine, 2-Vol Set)
- The proportion of VRE among hospitalised patients can be as high as 30% in some settings. (Red Book 2021)
3. Risk Factors for VRE Colonisation and Infection in the ICU
Patient-level Risk Factors
- Prolonged ICU / hospital stay (colonisation pressure rises ~1.4% per day)
- Prior broad-spectrum antibiotic exposure - especially multi-drug regimens with antianaerobic activity: clindamycin, metronidazole, piperacillin-tazobactam
- Hematological malignancy / bone marrow transplant / HSCT
- Solid organ transplantation (especially liver transplant)
- Chronic renal insufficiency / dialysis
- HIV infection
- Neutropenia / immunosuppression
- Pre-existing urethral catheters or intravascular lines
- Recent surgery (especially abdominal/hepatobiliary)
- Prior VRE colonisation or infection
- Age ≥60 years
- Uncontained body fluids, need for toileting assistance (IPAC Canada, 2025)
Environmental / ICU-Level Risk Factors
- High colonisation pressure in the unit (prevalence of colonised patients is the strongest independent predictor of new acquisition)
- Inadequate hand hygiene compliance
- Shared or inadequately cleaned equipment
- Prolonged environmental survival - VRE can persist on dry surfaces for weeks to months
4. Clinical Presentations
Nearly all Enterococcal infections are preceded by asymptomatic gastrointestinal colonisation. Only 1 in 10 colonised patients develops symptomatic infection. In the ICU, the main clinical syndromes are:
| Syndrome | Key Features |
|---|---|
| Bacteraemia | Most serious; often polymicrobial; may present as septic shock; sources: urinary tract, hepatobiliary, IVAD. Mortality ≥20% |
| Urinary tract infection | Most common; often catheter-associated; may be asymptomatic. Less likely to cause bacteraemia |
| Intra-abdominal / biliary infection | Polymicrobial; post-operative; liver transplant-associated; hepatic abscess. High mortality |
| Endocarditis | E. faecalis predominates; left-sided; subacute presentation; requires synergistic therapy |
| Skin / soft tissue / wound | Usually mixed; post-surgical site infections; diabetic foot; decubitus ulcers |
| Meningitis (rare) | Mostly post-neurosurgical; linezolid considered (Goldman-Cecil) |
5. Diagnosis
Microbiological
- Blood cultures (2 sets minimum): isolate from sterile site confirms true bacteraemia vs. contamination (clinical judgement required for single-positive bottles from catheter hubs)
- Urine culture: catheter-associated vs. symptomatic UTI distinction is important
- Wound / tissue / fluid cultures: sterile site cultures guide directed therapy
- Rectal swab / PCR screening: rapid detection of vanA/vanB genes; selective agar available; PCR is faster and more sensitive for active surveillance
- Species identification: MALDI-TOF increasingly used. E. faecium and E. faecalis must be reliably differentiated
- Susceptibility testing: ampicillin MIC, vancomycin MIC (to distinguish vanA/B/C), linezolid, daptomycin, tigecycline
- High-level aminoglycoside resistance (HLAR) testing mandatory before planning synergistic therapy
Molecular / Rapid Diagnostics
- PCR-based assays (BD GeneOhm VanR) detect vanA and vanB from rectal swabs and blood specimens
- Rapid ID from positive blood cultures (MALDI-TOF, multiplex PCR panels) can reduce time-to-effective therapy
- Red Book 2021; Henry's Clinical Diagnosis; Tietz Textbook of Laboratory Medicine
6. Treatment
Because of the complexity of enterococcal infections, infectious disease consultation is recommended for all severe VRE infections. (Goldman-Cecil Medicine)
6a. Antibiotic Treatment by Site
VRE Bacteraemia
| Agent | Dose | Notes |
|---|---|---|
| Linezolid | 600 mg IV/PO q12h | Drug of choice for non-bacteraemia infections; bacteriostatic; good outcomes in bacteraemia, though not FDA-approved for this indication. Risk of myelosuppression (esp. thrombocytopenia with >2 weeks use) |
| Daptomycin | 6-10 mg/kg IV q24h (higher doses 10-12 mg/kg often used in VRE BSI) | Bactericidal; not FDA-approved for VRE; good outcomes in BSI and soft tissue. Monitor CPK |
| Tigecycline | 50-100 mg IV q12h | FDA-approved for complicated SSTI and IAI caused by VSE E. faecalis only; black-box warning for increased mortality limits use in BSI |
| Tedizolid | 200 mg PO/IV q24h | Newest oxazolidinone; covers some linezolid-resistant strains; approved for SSTI only |
| Quinupristin-dalfopristin | 7.5 mg/kg IV q8h | Active against E. faecium only (not E. faecalis); second-line |
Note on linezolid in bacteraemia: Linezolid resistance is increasingly being reported, including in patients receiving prolonged treatment. Monitor susceptibility.
VRE Endocarditis
- Optimal therapy for VRE endocarditis resistant to ampicillin is not established
- Options include linezolid (not FDA-approved for endocarditis) and daptomycin (not FDA-approved for enterococcal infections) if susceptible
- Combination therapy (e.g., daptomycin + ampicillin, or daptomycin + linezolid) considered for refractory cases
- Goldman-Cecil Medicine
VRE Urinary Tract Infection
- Nitrofurantoin: most VRE strains remain susceptible even with vancomycin resistance (not for upper UTI / bacteraemia risk)
- Fosfomycin: effective for susceptible E. faecalis UTI
- Linezolid: reserved for symptomatic infections not responding to first-line agents
- Goldman-Cecil Medicine; Katzung Pharmacology
VRE Intra-abdominal / Health-care Associated Infection
- For patients at high risk or known VRE colonisation: daptomycin or linezolid as empiric therapy
- Fischer's Mastery of Surgery, 8th Ed
6b. Agents Not to Use for VRE
| Agent | Reason |
|---|---|
| Vancomycin | By definition - VRE is resistant |
| Teicoplanin | Inactive against vanA (high-level resistance) |
| Cephalosporins | Intrinsic resistance |
| Clindamycin | Intrinsic resistance |
| TMP-SMX | Clinical failures despite in vitro susceptibility (enterococci scavenge exogenous folate) |
| Tobramycin / kanamycin | No synergistic activity against enterococci |
| Quinupristin-dalfopristin | Inactive against E. faecalis; only for E. faecium |
6c. Toxicity Monitoring for Key Agents
| Agent | Key Toxicities | Monitoring |
|---|---|---|
| Linezolid | Thrombocytopenia, peripheral neuropathy, optic neuropathy, lactic acidosis, serotonin syndrome (with SSRIs/fentanyl/meperidine) | Weekly CBC; avoid with serotonergic agents |
| Tedizolid | Similar to linezolid (possibly less severe); interacts with serotonergic agents | CBC; caution with MAOIs |
| Daptomycin | Myopathy, rhabdomyolysis, eosinophilic pneumonia | Serial CPK; hold statins; avoid if CrCl <30 without dose adjustment |
| Tigecycline | Nausea/vomiting, elevated LFTs, increased mortality in BSI | Not recommended for BSI |
7. Infection Prevention and Control in the ICU
This is the cornerstone of VRE management. The key elements form a "bundle":
7a. Hand Hygiene
- Alcohol-based hand rub and soap-and-water compliance is the single most effective measure
- Note: Alcohol-based products are generally effective against VRE (non-spore former)
7b. Contact Precautions
- Standard of care for known or suspected VRE patients: private room, dedicated equipment (stethoscopes, BP cuffs), gloves and gown on entry
- IPAC Canada's 2025 Position Statement recognises that in endemic (non-outbreak) settings, several studies show no significant increase in VRE infection rates when routine isolation is discontinued (RR 0.93; 95% CI 0.68-1.26; p=0.62 for HA-VRE; RR 0.68; 95% CI 0.44-1.07 for HA-VRE BSI - Pan et al., AJIC, 2024 - PMID 39111343)
- However: Any reduction in precautions must be:
- Guided by regional/provincial requirements and local epidemiology
- Risk-based (facility VRE burden, patient vulnerability)
- Accompanied by close HAI monitoring with readiness to reinstate full precautions
- Resources saved from reduced screening reinvested in hand hygiene, environmental cleaning, and antimicrobial stewardship
7c. Active Surveillance Cultures (ASC)
- Rectal swab PCR or culture at ICU admission for high-risk patients:
- Prior VRE history
- Transfer from long-term care / another hospital
- Hematology/oncology, transplant patients
- Prolonged prior hospitalisation / antibiotic exposure
- Identifies asymptomatic colonised patients who are the primary reservoir for nosocomial transmission
- Surveillance cultures or PCR-based screening recommended; colonised patients placed on contact precautions
- Goldman-Cecil Medicine; IPAC Canada 2025
7d. Environmental Cleaning
- VRE survives on dry surfaces for extended periods - environmental decontamination is particularly important
- Routine terminal cleaning with EPA-registered disinfectants (hypochlorite-based for high-risk areas)
- Pulsed-xenon ultraviolet (PX-UV) decontamination as adjunct to manual cleaning: recent meta-analysis shows significant reduction in HAI burden (Ma et al., J Infect Chemother, 2025 - PMID 40373975)
- Dedicated equipment per patient where possible; shared equipment must be cleaned between patients
7e. Chlorhexidine Gluconate (CHG) Bathing
- Daily bathing with CHG-saturated cloths in ICU patients reduces VRE colonisation and infection
- A randomised trial in 8 adult ICUs + 1 BMT unit showed 23% reduction in combined MRSA and VRE acquisition with daily CHG bathing
- "Colonisation pressure" (prevalence of colonised patients in the unit) is the strongest predictor of new acquisition - CHG bathing as source control directly reduces this
- Goldman-Cecil Medicine (Grade A reference: Frost et al., Crit Care, 2019)
7f. Antimicrobial Stewardship
- Antibiotic selection pressure is a primary driver of VRE emergence
- Minimise use of glycopeptides, broad-spectrum antibiotics with anti-anaerobic activity (clindamycin, metronidazole, pip-tazo), and cephalosporins
- Multidisciplinary, physician-led stewardship programmes are mandated by WHO and ECDC
- Timely de-escalation, short courses, and protocol-driven empiric therapy all reduce VRE colonisation pressure
7g. Device Management
- Timely removal of urinary catheters and intravascular lines - prolonged device use is an independent risk factor for enterococcal BSI
- Catheter care bundles (CAUTI/CLABSI prevention) directly reduce VRE infection risk
8. Cohorting and Outbreak Management
- Cohorting of VRE-colonised or infected patients in dedicated bays/rooms with dedicated nursing staff is recommended during outbreaks
- Consider screening of roommates / contact patients when a new VRE case is identified
- Incident outbreak team notification; enhanced environmental sampling
- Reinstate full contact precautions and active surveillance if incidence rises above baseline
9. Prognosis
| Outcome | VRE | VSE (comparison) |
|---|---|---|
| In-hospital mortality (bacteraemia) | ≥20% | ~10% |
| Relative mortality risk (VRE faecium BSI vs VSE faecium) | RR 1.46 (95% CI 1.17-1.82) | - |
| Length of stay | Prolonged vs matched controls | - |
| Delayed adequate therapy | Associated with worse outcomes | - |
| 30-day infection risk for gut carriers | 8% (5-13%) | - |
- Goldman-Cecil Medicine; Eichel et al. 2023 (J Hosp Infect); Willems et al. 2023 (Lancet Infect Dis)
10. Special Populations in the ICU
- Solid organ transplant / HSCT patients: highest risk for VRE BSI; mortality very high; screening protocols essential (Nabavi et al., BMC Infect Dis, 2024 - PMID 39438823)
- Hematological malignancy: VRE a dominant pathogen in febrile neutropenia workup; empiric VRE coverage in colonised patients
- Liver transplant: hepatobiliary source most common; polymicrobial BSI; need for ID consultation
- Pre-operative screening: ESCMID/EUCIC 2024 guidelines recommend pre-operative decolonisation strategies for patients colonised with multidrug-resistant Gram-positive bacteria before surgery (Righi et al., Clin Microbiol Infect, 2024 - PMID 39154859)
11. Summary - ICU Practice Bundle
VRE ICU MANAGEMENT BUNDLE
══════════════════════════════════════════════
SCREENING | Rectal swab PCR on admission for high-risk patients
ISOLATION | Contact precautions (private room, gloves, gown)
| Risk-based in endemic settings (IPAC Canada 2025)
DECOLONISATION | Daily CHG bathing in all ICU patients
ENVIRONMENT | Enhanced cleaning + PX-UV adjunct
STEWARDSHIP | Minimise broad-spectrum/anti-anaerobic antibiotics
DEVICES | Early removal of IVAD + urinary catheters
HAND HYGIENE | Alcohol gel + soap-and-water compliance audits
TREATMENT (BSI) | Linezolid 600 mg q12h OR daptomycin 8-10 mg/kg q24h
| ID consultation for all severe VRE infections
MONITORING | Weekly CBC on linezolid; CPK on daptomycin
══════════════════════════════════════════════
Key References
- Eichel VM et al. Epidemiology and outcomes of VRE infections: systematic review and meta-analysis. J Hosp Infect 2023. [PMID 37734679] - VRE faecium BSI mortality RR 1.46 vs VSE
- Willems RPJ et al. Incidence of infection in MDR carriers: systematic review and meta-regression. Lancet Infect Dis 2023. [PMID 36731484] - 8% 30-day infection rate in VRE carriers
- Heath MR et al. Gut colonisation with MDRO in ICU: systematic review and meta-analysis. Crit Care 2024. [PMID 38943133] - 12.2/1000 patient-days acquisition rate in ICU
- Pan H et al. Removal of isolation for VRE: systematic review and meta-analysis. Am J Infect Control 2024. [PMID 39111343] - No increased HAI rate on discontinuing isolation in endemic settings
- Righi E et al. ESCMID/EUCIC guidelines on pre-operative decolonisation for MDR Gram-positive colonised patients. Clin Microbiol Infect 2024. [PMID 39154859]
- Ma L et al. Pulsed-xenon UV and HAI prevention: updated meta-analysis. J Infect Chemother 2025. [PMID 40373975]
- IPAC Canada. Position Statement: VRE Screening and Contact Precautions. September 2025.
- Goldman-Cecil Medicine, International Edition (2-Volume Set). Elsevier.
- Red Book 2021, Committee on Infectious Diseases, AAP.
- Tietz Textbook of Laboratory Medicine, 7th Edition. Elsevier.
- The Washington Manual of Medical Therapeutics. Wolters Kluwer.
- Katzung's Basic and Clinical Pharmacology, 16th Edition. McGraw-Hill.
- Fischer's Mastery of Surgery, 8th Edition.
can you explain Resistance Mechanisms via a infographic ?
Generating Image
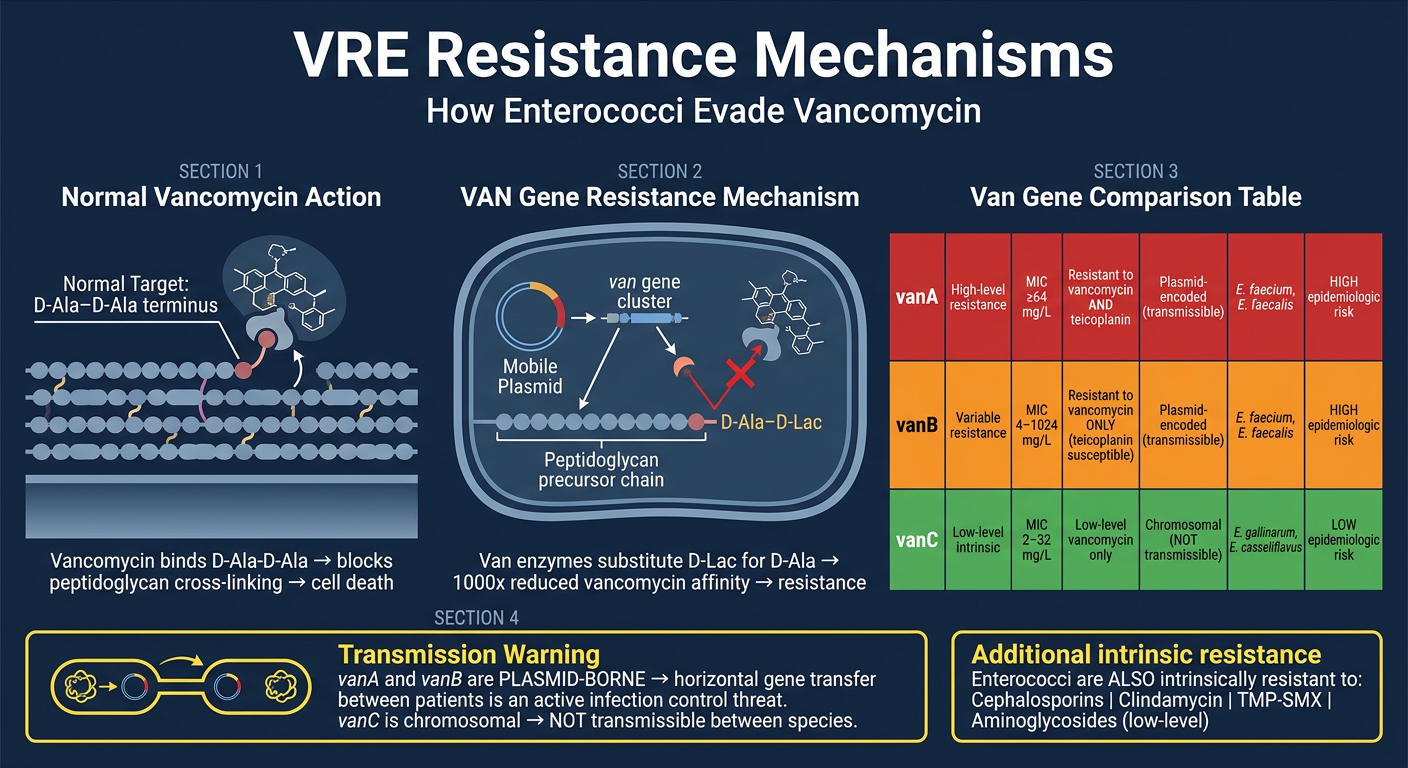
Here's the infographic breaking down the key resistance mechanisms:
The core concept in plain language:
Vancomycin normally works by grabbing onto a specific "handle" on the bacterial cell wall - the D-Ala-D-Ala terminus of peptidoglycan precursors. This blocks cell wall construction and kills the bacterium.
VRE cheats this by using van gene-encoded enzymes to swap out that handle - replacing D-Ala with D-Lactate (D-Lac). Vancomycin no longer fits. The binding affinity drops ~1000-fold, and the drug is rendered ineffective.
The three gene types to know:
- vanA (red): High-level resistance to both vancomycin and teicoplanin. Plasmid-borne, so it spreads between bacteria and between patients. The dominant type in the USA.
- vanB (orange): Variable resistance to vancomycin, but teicoplanin remains active. Also plasmid-borne and transmissible. Predominates in Europe (though vanA is rising there too).
- vanC (green): Low-level, intrinsic resistance in E. gallinarum and E. casseliflavus. Chromosomal - cannot be transferred to other species. Much lower clinical/epidemiological concern.
The plasmid-borne nature of vanA and vanB is what makes VRE such a serious infection control threat in the ICU - resistance genes can jump between organisms during a patient's stay.
can you explain Resistance Mechanisms via a infographic ? Make sure to point out each & every thing from the defination you have mentioned so that i can understand by looking at easily
Generating Image
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.