Hiii,.I've just started surgery posting today
- Always know your patients before rounds — vitals, overnight events, pending investigations, drain outputs
- Carry a small notebook or use your phone for patient lists
- Learn to present concisely: "Mr. X, Day 2 post-op lap chole, afebrile, vitals stable, tolerating diet, drains nil, plan for discharge"
- Arrive early, scrub properly (watch a scrub technique video if you haven't)
- Stand where you don't block the light, and don't touch anything blue (sterile field)
- If you're unsure whether something is sterile — assume it's not
- Ask questions between cases, not during critical steps
- Surgical knot tying (start practicing!)
- Basic instruments: scalpel, Kocher, Allis, retractors, needle holders
- Surgical site infection (SSI) prevention principles
- Pre-op, intra-op, and post-op roles
- Be enthusiastic and proactive — volunteer to help with dressings, sutures, IV lines
- Residents remember students who show up early and stay engaged
- It's okay not to know — it's not okay not to try
Hemorrhage and shock 101 please
Hemorrhage & Shock — Surgery 101
What Is Shock?
Types of Shock (The Big 4)
| Type | Mechanism | Classic Example | Key Feature |
|---|---|---|---|
| Hypovolemic | ↓ intravascular volume | Trauma, GI bleed, burns | Cold, clammy, tachycardic |
| Distributive | ↓ SVR / vasodilation | Sepsis, anaphylaxis, neurogenic | Warm skin (early sepsis) |
| Cardiogenic | Pump failure | MI, myocarditis | Pulmonary edema |
| Obstructive | Outflow obstruction | Tension pneumo, tamponade, PE | Raised JVP |
In surgery, hypovolemic (hemorrhagic) shock is what you'll encounter most — especially in trauma and post-op patients.
Hemorrhagic Shock: The Physiology
- Arteriolar vasoconstriction → ↑ Total Peripheral Resistance
- Venous constriction → maintains venous return
- Tachycardia → HR can rise to 160–180 bpm
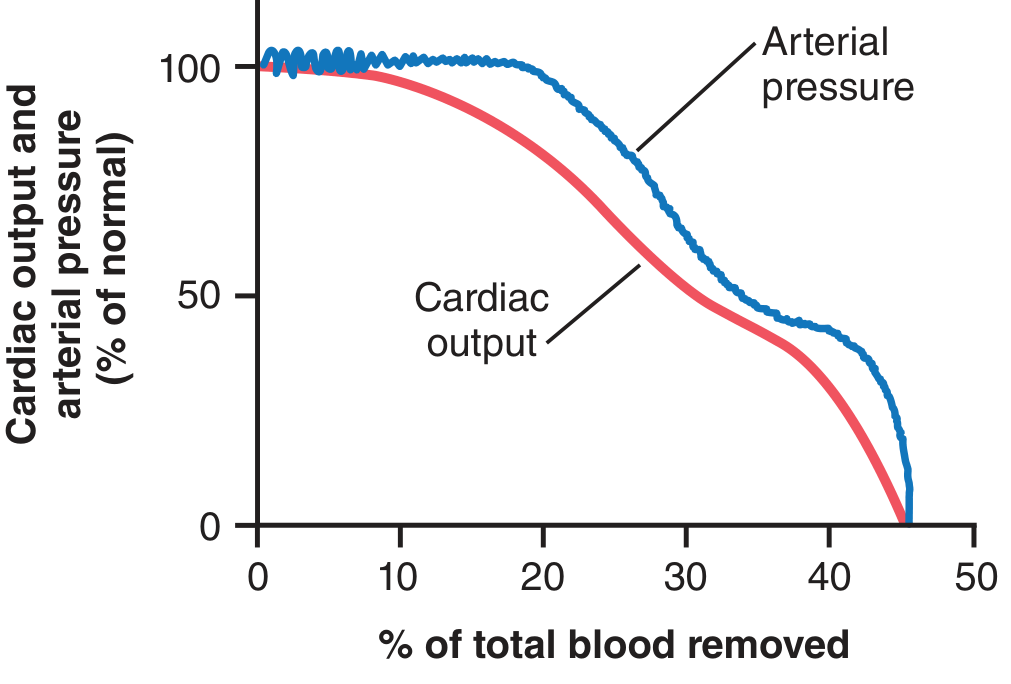
ATLS Classification of Hemorrhagic Shock
| Class | Blood Loss | HR | BP | Urine Output | Mental Status | Treatment |
|---|---|---|---|---|---|---|
| I | <15% (<750 mL) | <100 | Normal | >30 mL/h | Normal | IV fluids |
| II | 15–30% (750–1500 mL) | >100 | ↓ | 20–30 mL/h | Anxious | IV fluids |
| III | 30–40% (1500–2000 mL) | >120 | ↓↓ | 5–15 mL/h | Confused | Fluids + blood |
| IV | >40% (>2000 mL) | >140 | ↓↓↓ | Negligible | Lethargic/unconscious | Fluids + blood (emergency) |
3 Stages of Shock (Harrison's)
-
Compensated (preshock): Body compensates — HR rises, SVR rises, BP maintained. Mild lactate elevation. Organs still okay. Reversible if caught here.
-
Decompensated (true shock): Compensatory mechanisms overwhelmed. Hypotension, organ dysfunction (↑ creatinine, altered consciousness, oliguria). Still reversible with aggressive treatment.
-
Irreversible shock: Permanent organ damage. Multiorgan failure. Even with treatment, death is likely.
⚠️ The goal is to catch shock at Stage 1 or 2 — never let it reach Stage 3.
Progressive Deterioration in Untreated Shock
- ↓ perfusion → ischemic tissues → release of histamine, serotonin, cytokines
- Capillary permeability ↑ → fluid leaks into interstitium → further ↓ volume
- Lactic/carbonic acid → blood "sludging" in microvasculature → microthrombi
- CNS ischemia → vasomotor centre fails → complete cardiovascular collapse
Management: The Surgical Approach
Immediate steps (think ABCDE + hemorrhage control)
- Stop the bleeding — pressure, tourniquet, surgical control. "Stop the bleeding first" is the golden rule.
- Two large-bore IV lines (antecubital, 16G or larger)
- Send bloods: FBC, U&E, coagulation, cross-match, ABG (lactate!)
- Fluid resuscitation:
- Class I–II: Crystalloid (Normal saline or Lactated Ringer's)
- Class III–IV: Blood products. Rule of thumb — start pRBCs once crystalloids exceed 30 mL/kg (~2L)
- Target MAP ≥ 60–65 mmHg
- Monitor urine output (catheterise) — aim >0.5 mL/kg/h
- Warm the patient — hypothermia worsens coagulopathy
The Lethal Triad (avoid at all costs in trauma)
Hypothermia + Acidosis + Coagulopathy — each worsens the others. Breaking this cycle is the core of damage control surgery.
Quick Summary Card
Shock = ↓ O₂ delivery to tissues
Hemorrhagic shock = most common in surgery
Signs: tachycardia > hypotension (BP is a late sign!)
ATLS Class I→IV based on blood loss %
3 stages: Compensated → Decompensated → Irreversible
Treatment: Stop bleeding + Fluids + Blood products + Monitor UO
Avoid: Lethal triad (hypothermia + acidosis + coagulopathy)
General Examination and specific thyroid Examination
thyroid goiter examination neck swelling
Graves disease exophthalmos proptosis hyperthyroidism clinical signs
General Examination + Thyroid Examination
PART 1: General Examination
The 10 Components of General Examination
| Parameter | What to Look For |
|---|---|
| Build & Nutrition | Obese / average / thin / cachectic / wasted |
| Pallor | Conjunctival pallor (pull lower lid) → anaemia |
| Jaundice | Sclerae (yellow tinge) → liver/haemolysis |
| Cyanosis | Central (tongue) or peripheral (fingertips) |
| Clubbing | Grades 1–4; causes: lung, heart, liver, IBD |
| Lymphadenopathy | Cervical, axillary, inguinal nodes |
| Oedema | Pitting (press shin for 5s) vs non-pitting |
| Dehydration | Skin turgor (pinch abdomen), dry tongue, sunken eyes |
| Pulse | Rate, rhythm, volume, character |
| Temperature | Febrile / afebrile |
Surgery tip: Always add vitals (BP, HR, RR, SpO₂, temp) and urine output in surgical patients.
Presenting General Examination
"The patient is conscious, oriented, and cooperative. She is moderately built and nourished. She has no pallor, jaundice, cyanosis, or clubbing. There is no significant lymphadenopathy or pedal oedema."
PART 2: Thyroid Examination
The Key Rule Before You Start
Ask the patient to swallow while you watch the neck from across the room. A thyroid swelling moves up with swallowing — this distinguishes it from other neck lumps. A thyroglossal cyst moves up with tongue protrusion.
Step-by-Step Thyroid Examination
1. INSPECTION (from front, patient seated)
- Inspect the anterior neck at rest
- Ask patient to swallow (offer a glass of water) — does the swelling move?
- Note:
- Size — localised or diffuse?
- Shape — single nodule / multinodular / diffuse?
- Symmetry — unilateral or bilateral?
- Surface — smooth / irregular / nodular
- Overlying skin — erythema, dilated veins, scar (previous surgery)
- Visible pulsation — seen in vascular goitres (hyperthyroidism)

2. PALPATION (stand behind the patient — the surgical way)
- Site — which lobe? Isthmus?
- Size — approximate cm
- Shape — diffuse or nodular
- Surface — smooth / irregular
- Consistency — soft / firm / hard / rubbery
- Soft → colloid goitre
- Rubbery/firm → Hashimoto's
- Hard/stony → malignancy or Riedel's
- Tenderness — tender in thyroiditis; non-tender in most others
- Mobility — mobile in benign; fixed/tethered → malignancy
- Fixity to skin — pinch skin over the swelling
- Fluctuation — cysts may fluctuate
- Ask patient to swallow again — confirm movement
- Cervical lymph nodes — central compartment (level VI), lateral (levels II–IV) — for malignancy
- Trachea — is it central or deviated? (large goitre can deviate it)
- Berry's sign — absence of carotid pulsation on the side of a malignant thyroid (carotid encasement)
3. PERCUSSION
- Percuss over the upper sternum (manubrium) from top downward
- Dullness on sternal percussion → retrosternal extension of goitre
- This is often missed but is a surgical red flag
4. AUSCULTATION
- Place the bell of the stethoscope over each lobe
- Listen for a bruit (continuous swooshing murmur) → indicates increased vascularity
- Bruit is a hallmark of Graves' disease (active hyperthyroidism)
- Ask the patient to hold their breath during auscultation (to eliminate tracheal breath sounds)
Special Tests in Thyroid Examination
| Test | How | Positive = |
|---|---|---|
| Kocher's test | Press laterally on the goitre | Stridor → tracheal compression |
| Pemberton's sign | Ask patient to raise both arms above head | Facial plethora, JVP rise, cyanosis → retrosternal goitre compressing superior vena cava |
| Berry's sign | Palpate carotid pulse medially | Absent pulsation on one side → malignant infiltration |
Pemberton's sign is one of those dramatic signs you'll love showing on rounds.
General Examination in a Thyroid Patient
In Hyperthyroidism (Graves' disease especially):

| System | Signs |
|---|---|
| Hands | Fine tremor (paper test), warm moist palms, thyroid acropathy (clubbing), onycholysis (Plummer's nails) |
| Pulse | Tachycardia, irregularly irregular (AF) |
| Eyes | Exophthalmos, lid lag (von Graefe's sign), lid retraction (Dalrymple's sign), chemosis, ophthalmoplegia |
| Skin | Pretibial myxedema (non-pitting, over shins), hyperpigmentation |
| Reflexes | Hyperreflexia |
In Hypothyroidism (Hashimoto's, post-surgery):
| System | Signs |
|---|---|
| Hands | Cold dry skin, nail brittleness |
| Face | Puffy, myxedematous face, loss of lateral eyebrow (Queen Anne's sign) |
| Hair | Dry, brittle, thinning; loss of outer third of eyebrows |
| Voice | Hoarse |
| Reflexes | Slow-relaxing reflexes (hung-up reflex) — a classic sign! |
| Pulse | Bradycardia |
How to Present Thyroid Examination
"On inspection, there is a diffuse smooth swelling in the anterior neck involving both lobes of the thyroid, which moves up with deglutition. On palpation from behind, the gland is diffusely enlarged, smooth, non-tender, firm, mobile, not fixed to skin or deep structures. Trachea is central. No cervical lymphadenopathy is palpable. On percussion, there is no retrosternal dullness. On auscultation, a bruit is present over both lobes. General examination reveals fine tremors, warm moist hands, and lid lag — consistent with hyperthyroidism."
Quick Summary Card
Thyroid swelling moves UP with swallowing ← key differentiator
Palpate from BEHIND (surgeon's approach)
Hard + fixed + LN → think malignancy
Bruit → Graves' disease (hyperthyroid)
Pemberton's sign → retrosternal extension
Tremor + tachycardia + exophthalmos → Graves' triad
Slow reflexes + puffy face + bradycardia → Hypothyroid
Inguinal hernia 101
Hernias 101
Thyroid ca 101
papillary thyroid carcinoma histology microscopy Orphan Annie eye nuclei
Thyroid Cancer — Surgery 101
Overview: The Big Picture
Papillary → Follicular → Medullary → Anaplastic
The 4 Types at a Glance
| Feature | Papillary | Follicular | Medullary | Anaplastic |
|---|---|---|---|---|
| Frequency | ~85% | 5–15% | <5% | ~1% |
| Cell of origin | Follicular cell | Follicular cell | C cells (parafollicular) | Follicular cell |
| Spread | Lymphatics | Blood (lungs, bone, liver) | Lymphatics + blood | Local invasion + blood |
| Marker | Thyroglobulin | Thyroglobulin | Calcitonin | None |
| Key mutation | BRAF V600E, RET fusion | RAS, PAX8/PPARG | RET point mutation | TP53 loss |
| Prognosis | Excellent (>95% 10-yr survival) | Good (minimally invasive) to moderate | Intermediate | Uniformly lethal |
| Radioiodine (RAI) sensitive? | Yes | Yes | No | No |
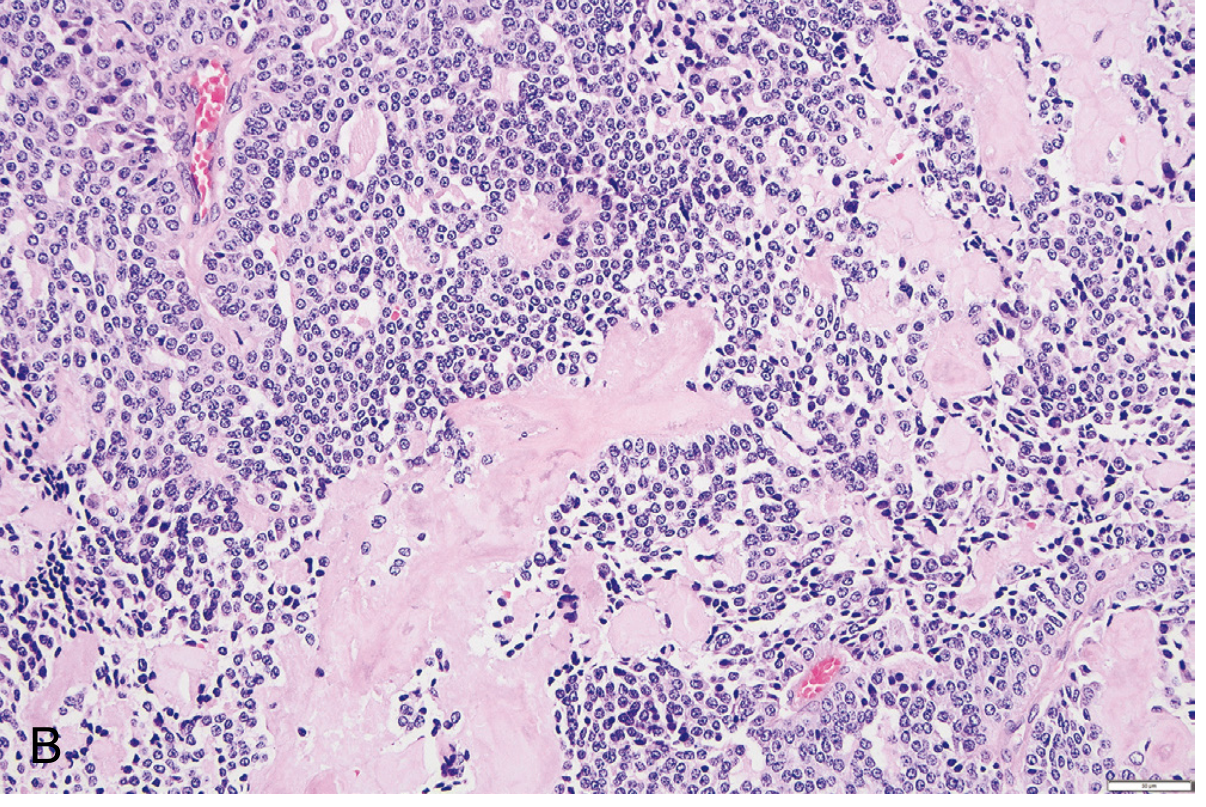
1. Papillary Thyroid Carcinoma (PTC)
Key Histological Features (what the pathologist sees)
- Papillary architecture — finger-like projections with fibrovascular core
- "Orphan Annie eye" nuclei — optically clear, empty-looking nuclei
- Nuclear grooves and pseudo-inclusions
- Psammoma bodies — concentrically calcified concentric rings (almost pathognomonic for PTC)
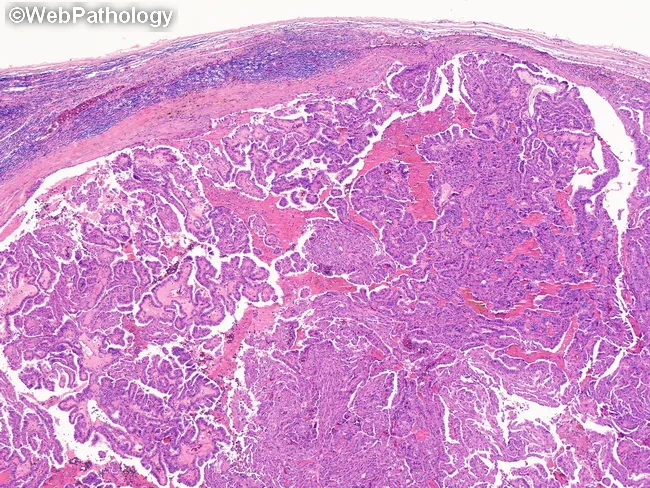
Key point: The nuclear features alone are diagnostic even WITHOUT papillary architecture.
Clinical Features
- Painless neck mass (within thyroid OR as a cervical lymph node metastasis)
- More common in women, peaks 30–50 years
- Can be multifocal within the thyroid
- FNAC (fine needle aspiration cytology) is usually diagnostic preoperatively
Spread & Prognosis
- Spreads via lymphatics → cervical lymph nodes (up to 50% of cases)
- Isolated nodal metastases do NOT worsen prognosis significantly in younger patients
- Rare haematogenous spread (lungs most common)
- 10-year survival >95% — one of the best prognoses of any cancer
2. Follicular Thyroid Carcinoma
Key Histological Features
- Uniform follicular cells resembling normal thyroid
- Diagnosis requires CAPSULAR ± VASCULAR INVASION — cannot be diagnosed on FNAC alone (this is why follicular lesions on FNAC need surgery)
- Distinguished from follicular adenoma only by invasion on histology
Clinical Features
- Presents as a solitary cold nodule
- More common in women, peak age 40–60 years
Spread & Prognosis
- Spreads via blood → lungs, bone, liver (haematogenous)
- Regional LN metastasis is uncommon
- Minimally invasive: <10% mortality at 10 years
- Widely invasive: ~50% mortality at 10 years
Surgeon's pearl: FNAC says "follicular lesion" → operate, because you cannot distinguish adenoma from carcinoma without the surgical specimen.
3. Medullary Thyroid Carcinoma (MTC)
Epidemiology
- 70% sporadic (solitary nodule, adults, peak 40s–50s)
- 30% familial — associated with MEN2A or MEN2B or Familial MTC
- All familial cases carry germline RET mutations
- Familial cases: bilateral, multifocal, younger patients
MEN Associations (must know)
| Syndrome | Components |
|---|---|
| MEN 2A | MTC + Phaeochromocytoma + Hyperparathyroidism |
| MEN 2B | MTC + Phaeochromocytoma + Mucosal neuromas + Marfanoid habitus |
| Familial MTC | MTC only (germline RET, no other MEN features) |
Any patient with MTC should be screened for phaeochromocytoma before surgery — operating on an undiagnosed phaco can kill the patient.
Key Histological Feature
- Polygonal to spindle cells in nests/trabeculae
- Amyloid deposits in stroma (derived from calcitonin polypeptides) — characteristic!
Tumour Marker
- Calcitonin — used for diagnosis AND follow-up (if calcitonin rises post-op → recurrence)
- Some also secrete serotonin, ACTH, VIP
Treatment
- Surgery (total thyroidectomy + central neck dissection)
- NOT radioiodine-sensitive
- Targeted therapy (vandetanib, cabozantinib) for metastatic disease
4. Anaplastic (Undifferentiated) Thyroid Carcinoma
Key Points
- Arises de novo or by dedifferentiation of a pre-existing PTC or follicular carcinoma (TP53 loss is the key step)
- Mean age at presentation: 65 years
- Up to 25% have a prior history of well-differentiated thyroid carcinoma
Clinical Presentation
- Rapidly enlarging, bulky, hard neck mass — this is the hallmark
- Symptoms of compression: dysphagia, dysphonia (hoarseness), dyspnea, stridor
- Most are already locally invasive or metastatic (lungs) at presentation
Prognosis
- Death in <1 year in most cases
- NOT radioiodine-sensitive
- Surgery rarely curative — palliative approach with external beam RT ± targeted therapy
Investigations for a Thyroid Nodule (Work-up)
Step 1: TSH (is it hyper/hypo/euthyroid?)
Step 2: Ultrasound (USS) — size, echogenicity, margins, calcifications, LN
Step 3: FNAC (fine needle aspiration cytology) → Bethesda system reporting
Step 4: If follicular lesion on FNAC → surgery (hemithyroidectomy)
Step 5: CT neck/chest if large, substernal, or suspected malignancy
Step 6: Calcitonin if MTC suspected
Step 7: Thyroglobulin post-thyroidectomy for follow-up
The Bethesda System (FNAC reporting for thyroid)
| Bethesda Category | Diagnosis | Malignancy Risk | Action |
|---|---|---|---|
| I | Non-diagnostic | — | Repeat FNAC |
| II | Benign | <3% | Observe |
| III | Atypia of undetermined significance | ~10–30% | Repeat / molecular testing |
| IV | Follicular neoplasm | 25–40% | Hemithyroidectomy |
| V | Suspicious for malignancy | 60–75% | Surgery |
| VI | Malignant | >97% | Surgery |
Treatment Summary
| Type | Surgery | Radioiodine (¹³¹I) | TSH Suppression | Monitoring |
|---|---|---|---|---|
| Papillary | Total thyroidectomy ± neck dissection | Yes (if high risk) | Yes | Thyroglobulin + USS |
| Follicular | Total thyroidectomy | Yes | Yes | Thyroglobulin + USS |
| Medullary | Total thyroid + central neck dissection | No | No | Calcitonin |
| Anaplastic | Palliative surgery/tracheostomy | No | No | CT imaging |
Red Flags on History/Exam Suggesting Malignancy
✗ Hard, firm, fixed, non-tender thyroid nodule
✗ Rapid growth
✗ Hoarseness (recurrent laryngeal nerve invasion)
✗ Dysphagia (oesophageal invasion)
✗ Cervical lymphadenopathy
✗ History of neck radiation
✗ Age extremes (<20 or >60)
✗ Male sex (more likely malignant than in females)
✗ Family history of MTC or MEN
Quick Summary Card
4 types: Papillary (85%) > Follicular > Medullary > Anaplastic
PTC: Orphan Annie nuclei + psammoma bodies, lymphatic spread, excellent prognosis
Follicular: Cannot diagnose by FNAC alone, haematogenous spread
Medullary: C cells, calcitonin marker, amyloid on histo, RET mutation, MEN2
Anaplastic: Rapidly enlarging hard mass, TP53 loss, uniformly lethal
Work-up: USS → FNAC (Bethesda) → Surgery
Radioiodine works: PTC and FTC only
Acute cholecystitis
Urology : Neoplasms of kidney, ureter, & bladder 101
Do surgery operation 101
Surgery in the OT — 101 for Students
PART 1: Pre-operative Phase ("Before the Cut")
Pre-operative Assessment
- Full history: presenting complaint, comorbidities (DM, HTN, cardiac, renal, bleeding disorders), medications, allergies, previous surgeries/anaesthesia
- Drug history is critical: stop anticoagulants (warfarin 5 days before, NOACs 24–48 hrs), stop metformin (24–48 hrs before, risk of lactic acidosis), continue antihypertensives and cardiac drugs
- Family history of anaesthetic problems → ask about malignant hyperthermia
| Investigation | Why |
|---|---|
| FBC | Anaemia, infection, platelets |
| RFT (Urea, Creatinine, Electrolytes) | Renal function, K+ (risk with anaesthesia) |
| LFT | Clotting factors, nutritional status |
| Coagulation (PT/INR, aPTT) | Bleeding risk |
| Blood group & cross-match | Anticipate transfusion |
| ECG | Cardiac baseline (>40 yrs or cardiac hx) |
| CXR | Baseline, detect pulmonary pathology |
| Blood glucose / HbA1c | Diabetics — perioperative glucose control |
| Grade | Description | Example |
|---|---|---|
| ASA I | Healthy | Young fit patient |
| ASA II | Mild systemic disease | Controlled DM, HTN |
| ASA III | Severe systemic disease | Poorly controlled DM, COPD |
| ASA IV | Life-threatening disease | Recent MI, severe heart failure |
| ASA V | Moribund | Ruptured AAA |
| ASA VI | Brain-dead donor | Organ harvest |
Higher ASA = higher anaesthetic and operative risk. Surgeons quote this when consenting patients.
Consent
- Must be informed, voluntary, and competent
- Surgeon (not nurse/student) must consent the patient
- Explain: procedure, benefits, risks (common AND serious), alternatives, what happens if not done
- Document: specific risks relevant to that operation (e.g., "RLN injury and voice change" for thyroidectomy)
Fasting (NBM — Nil By Mouth)
| What | Time before surgery |
|---|---|
| Clear fluids | 2 hours |
| Breast milk | 4 hours |
| Solids / formula / non-clear fluids | 6 hours |
| Mnemonic: 2-4-6 rule |
Pre-operative Marking
- Surgeon marks the correct site and side with a permanent marker
- Done in the ward, with patient awake and confirming
- Prevents wrong-site surgery (a "never event")
WHO Surgical Safety Checklist
| Pause | When | What's checked |
|---|---|---|
| Sign In | Before anaesthesia | Identity, consent, site marked, allergies, anaesthetic check |
| Time Out | Before skin incision | Team introductions, procedure confirmed, antibiotics given, imaging displayed |
| Sign Out | Before patient leaves OT | Instrument/swab counts correct, specimen labelled, post-op plan |
PART 2: Anaesthesia Basics
Types of Anaesthesia
| Type | What it is | Example |
|---|---|---|
| General (GA) | Patient fully unconscious | Laparotomy, thoracotomy |
| Regional — Spinal | Intrathecal injection → lower body block | LSCS, lower limb surgery |
| Regional — Epidural | Epidural space → continuous block | Labour analgesia, major abdominal |
| Regional — Nerve block | Block a specific nerve | Axillary block for hand surgery |
| Local | Infiltrate operative site | Minor procedures, biopsies |
| Sedation (MAC) | Monitored, patient conscious | Endoscopy, minor procedures |
Induction of GA — RSI (Rapid Sequence Induction)
- Pre-oxygenate
- Cricoid pressure (Sellick's manoeuvre)
- IV induction agent (propofol or thiopentone)
- Fast-acting muscle relaxant (suxamethonium)
- Intubate
- Confirm tube placement (EtCO₂, bilateral air entry)
The Triad of Anaesthesia
Hypnosis (unconscious) + Analgesia (pain-free) + Muscle relaxation (still)
Monitoring During Surgery (Minimum Standard)
- ECG
- SpO₂ (pulse oximetry)
- NIBP / IBP (non-invasive / invasive BP)
- EtCO₂ (end-tidal CO₂ — confirms intubation, detects problems)
- Temperature
- Urine output (catheter)
PART 3: Intra-operative Phase ("In the OT")
Sterile Field — Golden Rules for Students
- Anything blue/draped = sterile → don't touch
- If in doubt — it's not sterile
- Face the sterile field at all times
- Stay away from the scrub nurse's trolley
- Don't reach over the sterile field
- If you contaminate yourself → say so immediately
Surgical Scrub Technique
- Nails first (brush)
- Hands → wrists → forearms → elbows
- Keep hands above elbows at all times (water drains away from hands)
- Air dry, then gown and glove aseptically
Gowning and Gloving
- Open gown technique (scrub nurse assists)
- Closed gloving (hands stay inside gown cuffs until gloves are on) — preferred in scrubbing in for the first time
- Once gowned: keep hands above waist, below shoulders, in front of body — this is the sterile zone
Common Surgical Instruments (Know These!)
| Instrument | Use |
|---|---|
| Scalpel | Skin incision (10 blade most common, 15 for fine work) |
| Dissecting forceps (tissue/non-toothed) | Hold/manipulate tissue |
| Artery forceps (haemostat) — Kocher, Spencer-Wells | Clamp vessels |
| Allis forceps | Grasp tissue firmly |
| Needle holder (Mayo-Hegar) | Hold suture needle |
| Metzenbaum scissors | Dissect delicate tissue |
| Mayo scissors | Cut sutures, tougher tissue |
| Retractors — Deaver, Langenbeck, Balfour | Expose operative field |
| Diathermy (electrocautery) | Cutting + coagulation (monopolar/bipolar) |
| Suction — Yankauer, Poole | Clear blood/fluid |
Diathermy (Electrocautery)
- Monopolar: current passes through patient's body → return plate on thigh; used for cutting and coagulation; NOT safe near pacemakers/implants
- Bipolar: current passes only between two tips of forceps; used for delicate/precision work (e.g., neurosurgery, vascular)
- Cutting mode: continuous current → cuts cleanly
- Coagulation mode: pulsed current → seals vessels
Sutures — What You Must Know
| Absorbable | Non-absorbable |
|---|---|
| Vicryl (polyglactin) | Prolene (polypropylene) |
| Monocryl | Nylon (Ethilon) |
| PDS | Silk |
| Gut (plain/chromic) | Steel wire |
- Deep layers / bowel anastomosis / fascia → Absorbable (Vicryl, PDS)
- Skin → Non-absorbable removed after healing (Prolene, Nylon) OR absorbable Monocryl (subcuticular, no removal needed)
- Vascular anastomosis → Prolene (non-absorbable, permanent)
- Quick ties / ligatures → Silk, Vicryl
Surgical Knots
- Square knot (reef knot) — standard, most used
- Surgeon's knot — first throw is double, more secure
- Rule of 3: minimum 3 throws for any knot to be secure
PART 4: Post-operative Phase ("After the Cut")
Immediate Recovery (PACU — Post-anaesthesia Care Unit)
- Awake, oriented, following commands
- Stable vitals
- Pain controlled
- No excessive bleeding from wound/drains
Post-operative Orders (What the Surgeon Writes)
1. Vitals: every 15 min x 4, then hourly x 4, then 4-hourly
2. IV fluids: type, rate
3. Medications: analgesics, antibiotics, antiemetics, DVT prophylaxis
4. NBM or diet order (when to start feeding)
5. Drain: monitor output, when to remove
6. Catheter: monitor urine output (>0.5 mL/kg/hr)
7. Wound: dressing instructions
8. Special orders: blood glucose monitoring, O₂, positioning
Post-operative Complications — "The 5 Ws"
| Day | "W" | Cause |
|---|---|---|
| Day 1–2 | Wind | Atelectasis (collapsed lung segments) |
| Day 3–5 | Water | UTI (urinary tract infection) |
| Day 3–5 | Wound | Wound infection |
| Day 5–7 | Walking | DVT / PE |
| Day 7+ | Wonder drugs | Drug fever / abscess / anastomotic leak |
Early Mobilisation
- Start Day 0 or 1 post-op
- Reduces: atelectasis, DVT, ileus, pressure sores, hospital stay
- DVT prophylaxis: TED stockings + LMWH (e.g., enoxaparin 40 mg SC OD) + early mobilisation
Surgical Site Infection (SSI) Prevention
- Pre-op antibiotics: within 60 minutes before skin incision (timing is critical)
- Maintain normothermia (warm patient intraoperatively)
- Maintain normal glucose (hyperglycaemia impairs wound healing)
- Antiseptic skin preparation (chlorhexidine preferred over povidone iodine)
- Sterile technique throughout
PART 5: Surgical Positions (Know These for Theatre)
| Position | Used for |
|---|---|
| Supine | Laparotomy, hernia repair, appendicectomy |
| Lithotomy | Perianal/rectal surgery, gynaecology, TURP |
| Trendelenburg | Pelvic surgery, laparoscopy (bowel falls away from pelvis) |
| Reverse Trendelenburg | Upper abdominal/laparoscopic cholecystectomy |
| Lateral decubitus | Thoracotomy, nephrectomy |
| Prone | Posterior spinal surgery, pilonidal sinus |
| Sitting (beach chair) | Shoulder surgery |
Quick Summary Card
Pre-op: History + Ix → ASA grading → Consent → NBM 2-4-6 → Mark site
In OT: WHO checklist → Anaesthesia triad → Sterile field → Instruments
Sutures: Absorbable (deep) vs Non-absorbable (skin/vascular)
Post-op: Monitor vitals/drains/UO → 5 Ws for fever → Mobilise early
Antibiotics: Give WITHIN 60 mins before incision
DVT: TED stockings + LMWH + mobilise
Basic surgery 10
- "Basic surgery 101" (introductory guide — maybe you just meant that?)
- A specific topic like "basic surgical skills" (scrubbing, knots, sutures, drains)
- A numbered list of something specific (e.g., "top 10 things a surgery student must know")
- Something from your posting today you want to prep for?
On operative surgery
if the patient vomited fresh blood and malena with liver cirrhosis
Thyroid ca 101
Thyroid Cancer — Quick Recap
The 4 Types: "People Fear My Anger"
| Type | Frequency | Origin | Key Feature | Spread | Prognosis |
|---|---|---|---|---|---|
| Papillary | ~85% | Follicular cell | Orphan Annie nuclei + psammoma bodies | Lymphatics | Excellent (>95% 10-yr) |
| Follicular | 5–15% | Follicular cell | Can't diagnose by FNAC alone | Blood (lung, bone) | Good–moderate |
| Medullary | <5% | C cells | Calcitonin marker + amyloid | Lymph + blood | Intermediate |
| Anaplastic | ~1% | Follicular cell (dedifferentiated) | Rapidly enlarging hard mass | Local + blood | Uniformly lethal |
Key Facts by Type
- BRAF V600E mutation (up to 80%)
- Diagnosis by FNAC: nuclear grooves, pseudo-inclusions, psammoma bodies
- Lymph node mets don't significantly worsen prognosis in young patients
- Treatment: total thyroidectomy ± radioiodine (RAI)
- More common in iodine-deficient areas
- Diagnosis requires surgical specimen (capsular/vascular invasion) — FNAC only says "follicular lesion" → operate
- PAX8/PPARG fusion; MET mutations
- Treatment: total thyroidectomy + RAI
- 70% sporadic, 30% familial (germline RET mutation)
- MEN2A: MTC + Phaeochromocytoma + Hyperparathyroidism
- MEN2B: MTC + Phaeochromocytoma + Mucosal neuromas
- Marker: Calcitonin (diagnosis + follow-up)
- NOT RAI-sensitive → surgery + central neck dissection
- Screen for phaeochromocytoma before surgery
- TP53 loss → dedifferentiation from PTC/follicular
- Rapid growth, dysphagia, hoarseness, stridor
- Death usually within 1 year
- NOT RAI-sensitive; mainly palliative
Work-up of a Thyroid Nodule
TSH → USS → FNAC (Bethesda I–VI) → Surgery if needed
- I: Non-diagnostic → repeat
- II: Benign → observe
- III: AUS → repeat/molecular testing
- IV: Follicular neoplasm → hemithyroidectomy
- V: Suspicious → surgery
- VI: Malignant → surgery
Red Flags for Malignancy
Hard + fixed nodule | Rapid growth | Hoarseness
Cervical LN | Neck radiation history | Male sex
Age <20 or >60 | Family history of MTC/MEN
Post-op Monitoring
| Cancer | Marker | Method |
|---|---|---|
| PTC / FTC | Thyroglobulin + USS | Serial monitoring |
| MTC | Calcitonin | Serial monitoring |
Make a comparison table of thyroid cancer types
Thyroid Cancer — Comprehensive Comparison Table
| Feature | Papillary | Follicular | Medullary | Anaplastic |
|---|---|---|---|---|
| Frequency | ~85% | 5–15% | <5% | ~1% |
| Cell of origin | Follicular epithelium | Follicular epithelium | Parafollicular C cells | Follicular epithelium (dedifferentiated) |
| Age group | 30–50 yrs | 40–60 yrs | 40–50 yrs (sporadic) | >60 yrs |
| Sex predilection | F > M | F > M (3:1) | F = M | F > M |
| Associated conditions | Radiation exposure, Hashimoto's | Iodine deficiency | MEN 2A, MEN 2B, Familial MTC | Pre-existing PTC/follicular |
| Key mutation | BRAF V600E (~80%), RET fusion | RAS, PAX8/PPARG fusion | RET point mutation (germline + somatic) | TP53 loss |
| Gross appearance | Solid/cystic, may be multifocal | Single nodule, well-circumscribed | Firm, pale-grey, no capsule | Bulky, infiltrative, necrotic |
| Histology hallmarks | Orphan Annie nuclei, nuclear grooves, pseudo-inclusions, psammoma bodies, papillary fronds | Well-formed follicles resembling normal thyroid; diagnosis by capsular/vascular invasion | Polygonal-spindle cells in nests; amyloid in stroma; neuroendocrine granules | Pleomorphic/giant cells, spindle cells, no differentiation |
| Psammoma bodies | Yes (pathognomonic) | No | No | No |
| Amyloid stroma | No | No | Yes | No |
| FNAC diagnosis | Yes — nuclear features diagnostic | No — only says "follicular lesion"; needs surgery | Yes — calcitonin IHC helps | Yes — usually obvious |
| Lymph node spread | Common (up to 50%) | Uncommon | Moderate | Extensive, early |
| Distant metastasis | Rare (lung) | Common — lung, bone, liver (haematogenous) | Liver, lung, bone | Lung, widespread |
| Route of spread | Lymphatics | Blood (haematogenous) | Both | Local invasion + blood |
| Functional status | Non-functional (cold nodule) | Usually cold; rarely hyperfunctional | Non-functional | Non-functional |
| Tumour marker | Thyroglobulin | Thyroglobulin | Calcitonin, CEA | None reliable |
| Radioiodine (RAI) sensitive? | Yes | Yes | No | No |
| TSH suppression therapy? | Yes | Yes | No | No |
| Surgery | Total thyroidectomy ± central neck dissection | Total thyroidectomy | Total thyroidectomy + central neck dissection | Palliative / debulking |
| Pre-op screening required | — | — | Phaeochromocytoma screen before surgery | — |
| 10-year survival | >95% | ~70–90% (minimally invasive); ~50% (widely invasive) | ~70–80% | <10% (most die within 1 year) |
| Post-op monitoring | Thyroglobulin + neck USS | Thyroglobulin + neck USS | Calcitonin + neck USS | CT imaging |
| Unique associations | Childhood radiation | Iodine-deficient regions | MEN2A/2B; screen family with RET testing | Previous thyroid cancer |
| Prognosis drivers | Age >40, extrathyroidal extension, distant mets | Degree of invasion (minimal vs. wide) | Distant mets, HVPG >20, RET mutation type | Always poor regardless of treatment |
Key Memory Hooks
| Type | Remember by |
|---|---|
| Papillary | "Paps smear the Lymph nodes" — spreads to Lymphatics; Psammoma bodies |
| Follicular | "Follicular needs the Blood" — haematogenous spread; FNAC can't diagnose it |
| Medullary | "Medullary Makes calcitonin + MEN" — the one with amyloid + RET |
| Anaplastic | "Anaplastic = Always fatal" — TP53, hard mass, rapid death |
The One Table to Rule Them All (Ultra-condensed)
Papillary Follicular Medullary Anaplastic
Origin: Follicular Follicular C cells Follicular
Spread: Lymph Blood Both Local+Blood
Marker: Tg Tg Calcitonin None
RAI: Yes Yes NO NO
Survive: Excellent Good Moderate Lethal
Mutate: BRAF RAS/PAX8 RET TP53
Dr Rashide's questions : 1. Anaplastic vs lymphoma 2. Follicular vs papillary 3. Medullary : Sporadic vs Familial 4. FNAC vs Tru-cut 5. Prognosis and tumour market of anaplastic, lymphoma, follicular, papillary, medullary CA
Dr. Rashide's Questions — Answered
Q1. Anaplastic Thyroid Carcinoma vs Primary Thyroid Lymphoma
| Feature | Anaplastic Carcinoma | Primary Thyroid Lymphoma |
|---|---|---|
| Age | >60 years | >60 years |
| Sex | F > M | F > M |
| Background | Pre-existing PTC/follicular CA or goitre | Hashimoto's thyroiditis (40–80% of cases) |
| Risk increase | Prior well-differentiated thyroid CA | Hashimoto's → 60–80x increased lymphoma risk |
| Onset | Weeks | Weeks–months |
| Consistency | Rock hard, stony, fixed | Firm, "rubbery," may be less hard |
| Pain | Variable | Variable |
| B symptoms | Absent | Present — fever, night sweats, weight loss |
| Compressive symptoms | Dysphagia, hoarseness, stridor | Dysphagia, stridor |
| Cell type | Epithelial (follicular cell origin) | Lymphoid — usually diffuse large B-cell lymphoma (DLBCL) |
| Key mutation | TP53 loss | BCL-2 rearrangement, MYC |
| Histology | Pleomorphic/giant/spindle cells; no differentiation | Sheets of atypical lymphoid cells |
| IHC markers | CK+, thyroglobulin −, TTF-1 − | CD20+, CD3−, LCA+ |
| FNAC | Anaplastic cells — may be adequate | Lymphoid cells — but architecture needed |
| Preferred biopsy | Tru-cut / core needle | Tru-cut / core needle (FNAC often insufficient — need architecture) |
| Radioiodine | No | No |
| Treatment | Palliative (surgery/tracheostomy + RT ± chemo) | Chemotherapy (R-CHOP) + Radiotherapy — potentially CURABLE |
| Prognosis | Median survival <6 months; 1-yr survival <10% | Much better — 5-yr survival 50–70% with treatment |
Surgeon's pearl: If you see a rapidly enlarging thyroid mass in an elderly woman with Hashimoto's — think lymphoma first. It's treatable. Mistaking it for anaplastic and doing aggressive surgery is harmful.
Q2. Follicular vs Papillary Thyroid Carcinoma
| Feature | Papillary (PTC) | Follicular (FTC) |
|---|---|---|
| Frequency | ~85% | 5–15% |
| Age | 30–50 yrs | 40–60 yrs |
| Association | Radiation, Hashimoto's | Iodine deficiency |
| Key mutation | BRAF V600E (~80%), RET/PTC fusion | RAS, PAX8/PPARG fusion |
| Gross | Multifocal, may be bilateral | Usually solitary, encapsulated |
| Histology | Papillary fronds, Orphan Annie nuclei, nuclear grooves, psammoma bodies | Uniform follicles resembling normal thyroid |
| Psammoma bodies | Yes | No |
| Capsular invasion | Not a requirement for diagnosis | Required for diagnosis |
| Vascular invasion | Uncommon | Common — defines malignancy |
| FNAC diagnosis | Yes — nuclear features diagnostic | No — only "follicular lesion"; can't distinguish adenoma from carcinoma |
| Route of spread | Lymphatics → cervical LN (up to 50%) | Blood → lung, bone, liver |
| LN metastasis | Common | Rare |
| Distant mets | Uncommon | More common |
| RAI sensitivity | Yes | Yes |
| Prognosis | Excellent — >95% 10-yr survival | Good (minimally invasive) to moderate (widely invasive) |
| Tumour marker | Thyroglobulin | Thyroglobulin |
| Surgery | Total thyroidectomy ± neck dissection | Hemithyroidectomy (if follicular lesion on FNAC) → completion thyroidectomy if carcinoma confirmed |
Key distinction: PTC is diagnosed by nuclear features on FNAC. FTC can only be diagnosed on surgical histology by finding capsular or vascular invasion. This is why all "follicular lesions" on FNAC go to the theatre.
Q3. Medullary Thyroid Carcinoma — Sporadic vs Familial
| Feature | Sporadic MTC | Familial MTC |
|---|---|---|
| Frequency | ~70% | ~30% |
| Inheritance | Acquired somatic mutation | Autosomal dominant |
| Gene | Somatic RET point mutation | Germline RET mutation |
| Age at presentation | 40s–50s (adults) | Younger — even 1st decade in MEN2B |
| Laterality | Unilateral, solitary | Bilateral + multifocal |
| C-cell hyperplasia | Absent | Present (precursor lesion in contralateral lobe) |
| Associated syndromes | None | MEN2A, MEN2B, Familial MTC (FMTC) |
| MEN2A components | — | MTC + Phaeochromocytoma + Hyperparathyroidism |
| MEN2B components | — | MTC + Phaeochromocytoma + Mucosal neuromas + Marfanoid habitus |
| Pre-op screening | Phaeochromocytoma screen | Mandatory phaeochromocytoma screen before any surgery |
| Family screening | Not needed | Genetic screening of all 1st-degree relatives (RET mutation testing) |
| Prophylactic thyroidectomy | Not applicable | Yes — offered to RET mutation carriers; timing based on mutation risk category |
| Prognosis | Better (localized) | Worse in MEN2B (most aggressive); FMTC has best prognosis |
| Marker | Calcitonin, CEA | Calcitonin, CEA |
High-yield: In any MTC patient — screen for phaeochromocytoma first. Operating on an undiagnosed phaeochromocytoma can precipitate a fatal hypertensive crisis on the table.
Q4. FNAC vs Tru-cut (Core Needle Biopsy)
| Feature | FNAC (Fine Needle Aspiration Cytology) | Tru-cut (Core Needle Biopsy) |
|---|---|---|
| Needle size | 22–25G (fine) | 14–18G (large bore, cutting) |
| What you get | Individual cells (cytology) | Core of tissue (histology) |
| Anaesthesia | Local or none | Local anaesthesia |
| Architecture preserved? | No | Yes — intact tissue architecture |
| Capsular invasion visible? | No | Yes |
| IHC possible? | Limited | Yes — full panel possible |
| Speed | Fast, result in hours | Slower, 24–48 hrs |
| Pain/discomfort | Minimal | More |
| Complication risk | Very low | Low but higher than FNAC |
| Seeding risk | Very low | Slightly higher (theoretical) |
| Best for | PTC (nuclear features on cytology), benign cysts, initial triage | Lymphoma, anaplastic (need architecture + IHC), indeterminate FNAC |
| Cannot diagnose | Follicular carcinoma (needs capsular invasion), lymphoma (needs architecture) | — |
| Bethesda system | Applies to FNAC | Does not apply |
When to use which in thyroid:
| Scenario | Preferred biopsy |
|---|---|
| Suspicious thyroid nodule — first line | FNAC |
| FNAC shows "follicular lesion" (Bethesda IV) | Surgery (hemithyroidectomy) |
| Rapidly enlarging mass — ? lymphoma / ? anaplastic | Tru-cut |
| Recurrent thyroid mass post-surgery | Tru-cut or FNAC (US-guided) |
| Metastatic neck node — unknown primary | Tru-cut |
Q5. Prognosis and Tumour Markers
| Cancer | Tumour Marker(s) | 5-year Survival | 10-year Survival | Prognostic Factors |
|---|---|---|---|---|
| Papillary | Thyroglobulin (Tg) | ~98% | >95% | Age >40, extrathyroidal extension, distant mets, BRAF V600E |
| Follicular | Thyroglobulin (Tg) | ~85–90% | ~70–90% (minimally invasive); ~50% (widely invasive) | Degree of vascular invasion, distant mets, age |
| Medullary | Calcitonin, CEA | ~75–80% | ~65–70% | Distant mets, RET mutation type, MEN2B worst |
| Anaplastic | None reliable (thyroglobulin −, calcitonin −) | <10% | ~0% | Median survival 4–6 months; essentially uniformly fatal |
| Lymphoma | LDH, Beta-2 microglobulin (not thyroid-specific) | ~50–70% (DLBCL) | Depends on stage/type | Stage, International Prognostic Index (IPI), DLBCL vs MALT (MALT has better prognosis) |
Notes on markers:
- Thyroglobulin — only useful POST-total thyroidectomy. A rising Tg = recurrence of PTC or FTC. Useless if thyroid tissue remains.
- Calcitonin — used pre-op (diagnosis) AND post-op (surveillance). Undetectable calcitonin post-operatively = cure. Rising calcitonin = recurrence.
- CEA — elevated in MTC alongside calcitonin; rising CEA with falling calcitonin = poorly differentiated MTC (worse prognosis).
- Anaplastic — no useful serum marker; follow with CT imaging.
- Lymphoma — LDH reflects tumour burden; not thyroid-specific.
Summary Cheat Sheet for Dr. Rashide's Rounds
Anaplastic vs Lymphoma:
Both = rapid hard mass in elderly
Lymphoma → Hashimoto's background, B symptoms, CD20+, CURABLE with R-CHOP
Anaplastic → prior thyroid CA, TP53, CK+, always fatal
Papillary vs Follicular:
PTC → FNAC works, lymphatic spread, psammoma bodies, BRAF
FTC → FNAC can't diagnose, blood spread, needs capsular invasion, RAS/PAX8
Medullary Sporadic vs Familial:
Sporadic → unilateral, somatic RET, adults
Familial → bilateral/multifocal, germline RET, younger, MEN2 → SCREEN FAMILY
FNAC vs Tru-cut:
FNAC = cells only; good for PTC, first-line
Tru-cut = tissue architecture; needed for lymphoma, anaplastic, follicular adenoma vs CA
Markers:
PTC/FTC → Thyroglobulin
MTC → Calcitonin + CEA
Anaplastic → None
Lymphoma → LDH, Beta-2 microglobulin
Icsol
Choledocholethiasis 101
Thyroid ca 101