Meningioma
Reading File
Finding Sources
Searching PubMed
meningioma
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to write a thorough, well-organized answer on meningioma.
Meningioma
Overview
Meningiomas are the most common primary intracranial tumors, accounting for approximately 35% of newly diagnosed nervous system tumors. They arise from meningothelial (arachnoid cap) cells of the dura mater, and their incidence increases with age. They are more common in women and in patients with neurofibromatosis type 2 (NF2), and also occur more frequently in patients with a history of cranial irradiation.
- Harrison's Principles of Internal Medicine 22E, p. 765
- Bradley and Daroff's Neurology in Clinical Practice, p. 1560
Anatomy & Location
- 90% are supratentorial, arising in decreasing frequency from:
- Parasagittal region / superior sagittal sinus
- Cerebral convexities
- Sphenoid ridge
- Olfactory groove
- Infratentorial meningiomas favor the posterior surface of the petrous bones and clivus, and can mimic vestibular schwannomas
- Meningioma is the second most common CPA tumor (after vestibular schwannoma)
- Rare variants: meningioma en plaque (flat, infiltrating), intraventricular meningiomas
Grainger & Allison's Diagnostic Radiology, p. 1419-1420
WHO Classification (Histologic Grading)
| Grade | Category | Subtypes |
|---|---|---|
| I | Benign (~92%) | Meningothelial, fibrous/fibroblastic, transitional, psammomatous, angiomatous, secretory, lymphoplasmacyte-rich, metaplastic |
| II | Atypical (~6%) | Chordoid, clear cell, atypical; defined by high mitotic index, disordered growth, or brain invasion |
| III | Anaplastic/Malignant (~2%) | Papillary, rhabdoid, anaplastic; sarcoma/carcinoma/melanoma-like under light microscopy |
Grade I tumors have a low recurrence rate after complete resection. Grades II and III recur despite surgery and radiation.
K.J. Lee's Essential Otolaryngology, p. 489; Grainger & Allison's, p. 1420
Imaging
CT
- 60% are spontaneously hyperdense on non-contrast CT
- Up to 20% contain calcification
- Intense, uniform contrast enhancement
- Hyperostosis of adjacent bone is characteristic (vs. bone thinning with schwannomas)
- Bone destruction suggests atypical/malignant grade
MRI
- Frequently isointense to gray matter on both T1 and T2 - may be invisible without contrast
- Vivid, homogeneous enhancement after gadolinium
- Classic "dural tail" sign: thickened enhanced dura extending from the mass - frequent but NOT pathognomonic
- May have "capping cysts" with CSF-like signal
- Vasogenic edema is not uncommon; its extent does not correlate with tumor size, but presence may predict higher recurrence risk
Advanced MRI
- MR spectroscopy: alanine peak is characteristic, but seen in <50% of cases
- Perfusion-weighted imaging (PWI): markedly elevated rCBV, helping differentiate from dural metastases (which have lower rCBV)
- DWI/ADC: conflicting results for grading; may help suggest higher-grade transformation
Grainger & Allison's Diagnostic Radiology, pp. 1419-1421
MRI appearance - T2 (A) and post-gadolinium T1 with dural tail (B):
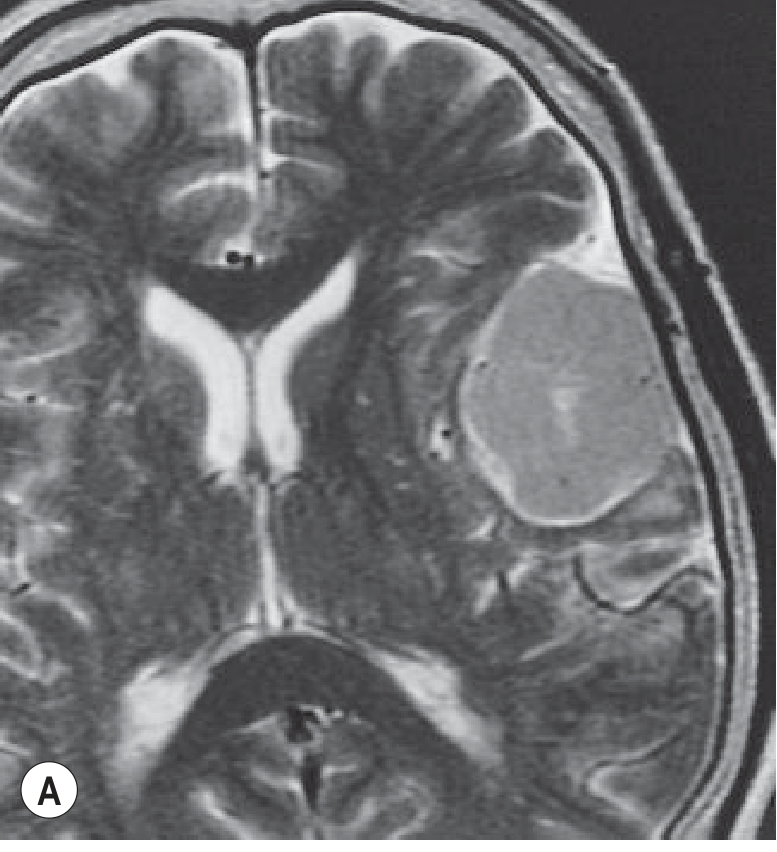

Fig. 55.27 from Grainger & Allison's: T1 (A) and gadolinium-enhanced T1 (B). The broad dural base, displaced sulci, and dural tail (arrow) are hallmarks of an extra-axial meningioma.
Post-gadolinium MRI showing multiple falcine meningiomas:
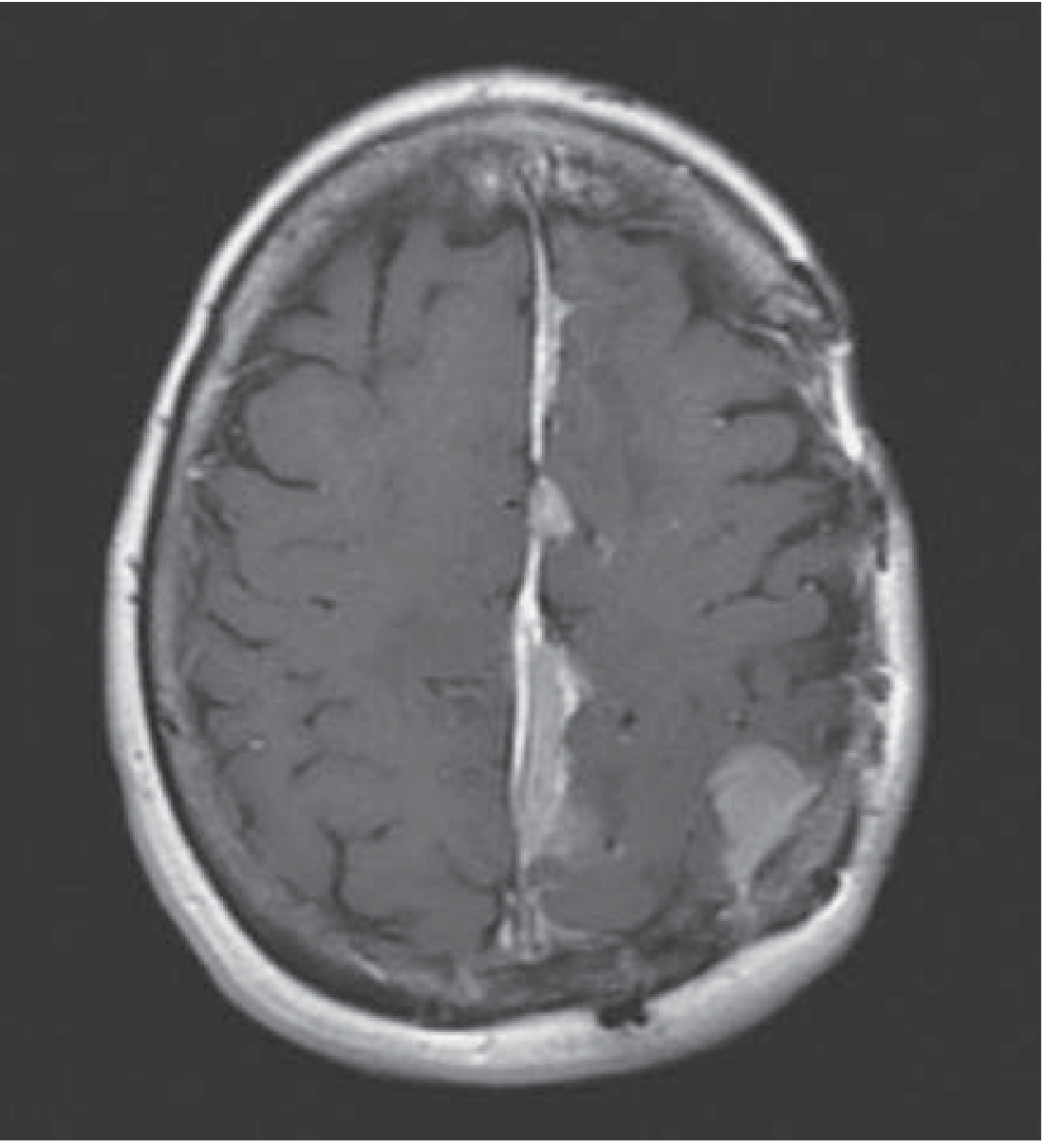
Multiple meningiomas along the falx and left parietal cortex (Harrison's Principles, Fig. 95-5)
Clinical Presentation
Many meningiomas are found incidentally on neuroimaging done for unrelated reasons. Symptomatic presentations depend on location:
- Headache
- Seizures (convexity tumors compressing cortex)
- Focal neurologic deficits (motor, sensory, visual, cranial nerve palsies)
- Cognitive/behavioral change (frontal lobe tumors)
- CPA tumors: sensorineural hearing loss, tinnitus, imbalance, facial paresthesia, diplopia, ataxia
- Hearing preservation is more common with meningiomas than with vestibular schwannomas
Molecular Pathogenesis
| Molecular Feature | Details |
|---|---|
| NF2 gene (chr 22q12.2) loss | ~60% of meningiomas; encodes merlin (membrane adhesion mediator). Found in 80% of transitional and fibroblastic types, but only 25% of meningothelial and virtually none of secretory/microcystic types. Associated with hemispheric/lateral skull base location |
| TRAF7 mutation | Most common feature in NF2-wildtype meningiomas (E3 ubiquitin ligase, pro-apoptotic) |
| KLF4 mutation | Seen with TRAF7; strongly associated with secretory meningiomas |
| AKT1 mutation | Common in meningothelial meningiomas; often with TRAF7 |
| SMO mutation | ~5% of non-NF2 meningiomas; localizes to medial anterior skull base |
| Del 1p, monosomy 14, del 9p21 | Found in higher-grade tumors; associated with shortened survival |
| NF2 mutations or non-NF2 mutations are nearly always benign | NF2-mutant tumors more likely to be atypical |
Quick Compendium of Clinical Pathology 5th ed.; Bradley and Daroff's, p. 1561
DNA methylation profiling (6 distinct methylation classes) has been shown to be a better predictor of recurrence and survival than WHO grades alone.
Histology
- Psammoma bodies (concentric calcified lamellae) are a hallmark
- Characteristic whorled pattern of meningothelial cells
- EMA (epithelial membrane antigen) positive
Management
Observation
- Small, asymptomatic meningiomas without mass effect or venous sinus compression can be followed with serial MRI
- Many meningiomas do not grow over years, especially in older adults
Surgery
- First-line for symptomatic, growing, or large tumors
- Complete surgical resection (Simpson grade I/II) is potentially curative for Grade I
- More challenging locations: dural venous sinus invasion, medial sphenoid, skull base, en plaque, posterior fossa, intraventricular
- Complications: infection, CSF leak, cerebral venous thrombosis, cranial neuropathies
Radiation
- External beam radiotherapy (EBRT) or stereotactic radiosurgery (SRS) for:
- Residual/unresectable tumor
- Recurrence or progression
- Adjuvant to surgery in higher-grade tumors
- Less aggressive surgery + SRS reduces morbidity and may improve progression-free survival (PFS)
Medical/Systemic Therapy
- Hormonal therapy (tamoxifen, mifepristone): disappointing in clinical trials despite receptor expression
- Somatostatin analogs: failed to show clear benefit in recurrent meningioma despite receptor expression
- VEGF inhibitors (bevacizumab, sunitinib, vatalanib): retrospective data suggest disease stability; still investigational
- Hydroxyurea, alpha interferon, chemotherapy regimens: some partial responses in recurrent/malignant cases
- Targeted therapies against NF2, TRAF7/KLF4, AKT1, SMO pathways are under investigation
Bradley and Daroff's, p. 1561; Harrison's, p. 765
Differential Diagnosis
The primary differential for a dural-based enhancing mass is dural metastasis. Other considerations include:
- Hemangiopericytoma / solitary fibrous tumor (SFT) - shares NAB2-STAT6 fusion; higher propensity for local recurrence and systemic metastasis
- Vestibular schwannoma (in CPA)
- Epidermoid cyst
Prognosis
- Grade I: low recurrence after complete resection; excellent prognosis
- Grade II: recurs despite surgery + radiation
- Grade III: aggressive, poor prognosis
- Molecular profile (especially DNA methylation class and del 1p/monosomy 14) predicts outcomes more reliably than WHO grading alone
Recent evidence note: A 2024 systematic review and meta-analysis (PMID 38902484) evaluated diagnostic imaging for meningioma grading, confirming the evolving role of advanced MRI in non-invasively predicting histologic grade - relevant for surgical planning.
Pathogenesis
Reading File
Finding Sources
Finding Sources
Searching PubMed
meningioma pathogenesis molecular genetics
Finding Sources
Finding Sources
Reading Article
Finding Sources
Finding Sources
Reading Article
Reading File
Reading File
Finding Sources
Finding Sources
I now have sufficient material from the textbooks and recent PubMed literature to deliver a thorough answer on meningioma pathogenesis.
Meningioma - Pathogenesis
The pathogenesis of meningioma involves a well-defined interplay of predisposing risk factors, cell of origin, and distinct molecular/genetic pathways that differ by tumor subtype, location, and grade.
Cell of Origin
Meningiomas arise from meningothelial (arachnoid cap) cells - specialized epithelioid cells found in arachnoid granulations of the dura mater. These cells can undergo neoplastic transformation at any site where arachnoid cell rests exist along the neuroaxis, which explains the wide distribution of meningioma locations.
Grainger & Allison's Diagnostic Radiology; Harrison's Principles, p. 765
Risk Factors
| Factor | Mechanism/Notes |
|---|---|
| Ionizing radiation | Strongest established environmental risk; dose-dependent; latency of 20-30 years; both therapeutic and low-dose diagnostic exposure implicated |
| NF2 germline mutation | Autosomal dominant; causes bilateral vestibular schwannomas + multiple meningiomas; germline loss of one NF2 allele, somatic loss of the second ("two-hit") drives tumorigenesis |
| Female sex | Meningiomas more common in women; hormonally responsive (express estrogen and progesterone receptors); peak incidence in 5th-7th decades |
| Sporadic (no germline cause) | ~90% of cases; driven by acquired somatic mutations |
Goldman-Cecil Medicine, p. (Chapter 175); Bradley and Daroff's
Two Major Molecular Subtypes
The molecular landscape of meningioma is broadly divided into two groups based on NF2 status:
1. NF2-Mutant Meningiomas (~60%)
Genetics:
- Loss of chromosome 22q12.2 (monosomy 22 or focal deletion) is present in ~60% of sporadic meningiomas
- This is an early event in tumorigenesis
- NF2 is a classical tumor suppressor gene - both alleles must be lost (two-hit model)
Merlin protein:
- The NF2 gene encodes merlin (also called schwannomin), a membrane-cytoskeleton scaffolding protein
- Merlin mediates cell-cell contact inhibition and acts upstream of multiple oncogenic pathways
- Loss of merlin disrupts:
- Hippo pathway - normally activates LATS1/2 kinases → phosphorylates YAP/TAZ → inhibits nuclear entry. Without merlin, YAP/TAZ translocate to the nucleus and drive proliferation genes
- mTOR/PI3K signaling - merlin suppresses mTORC1; loss activates mTOR-driven cell growth
- FAK/Src signaling - merlin normally suppresses focal adhesion kinase; loss promotes invasion
- EGFR/ErbB2 recycling - merlin limits receptor tyrosine kinase signaling; loss causes sustained growth factor receptor activation
Histologic correlation:
- NF2 mutations found in 80% of transitional and fibroblastic meningiomas
- Only 25% of meningothelial meningiomas
- Virtually none of secretory or microcystic meningiomas
- Predominantly hemispheric convexity and lateral skull base location
Quick Compendium of Clinical Pathology, 5th ed.; Bradley and Daroff's, p. 1561
2. NF2-Wildtype Meningiomas (~40%)
These are more heterogeneous. The most common driver mutations are:
| Mutation | Frequency | Key Features |
|---|---|---|
| TRAF7 | Most common in NF2-wt group | Pro-apoptotic E3 ubiquitin ligase; often co-occurs with KLF4 or AKT1 |
| KLF4 | With TRAF7 | Transcription factor; strongly associated with secretory meningiomas |
| AKT1 (E17K) | Common | Constitutively activates PI3K/AKT/mTOR pathway; predominant in meningothelial subtype; medial skull base location |
| SMO | ~5% | Activates Hedgehog signaling; exclusively in medial anterior skull base meningiomas; nearly always benign |
| PIK3CA | Subset | Activates PI3K pathway; skull base location |
| BAP1 | Rare | Histone deubiquitinase; associated with rhabdoid subtype; poor prognosis |
NF2-wildtype meningiomas are nearly always benign (Grade I). Location strongly correlates with genotype:
- Cerebral convexity / spinal meningiomas → 22q deletion / NF2 mutations
- Skull base meningiomas → AKT1, TRAF7, SMO, PIK3CA mutations
AJNR Review 2025 [PMID 38844366]; Bradley and Daroff's, p. 1561; Goldman-Cecil Medicine
Progression to Higher Grade
Malignant transformation (Grade II/III) involves accumulation of additional genomic hits on top of the initiating mutation:
| Molecular Event | Significance |
|---|---|
| Del 1p | Most consistent secondary change in higher-grade tumors; co-occurring with 22q loss now upgrades Grade I morphology to Grade II (per cIMPACT-NOW update 8) |
| Monosomy 14 / del 14q | Associated with shortened survival |
| Del 9p21 (CDKN2A/B deletion) | Homozygous deletion = WHO Grade III marker (per 2021 WHO CNS5); major cell cycle deregulation via loss of p16 and p15 |
| TERT promoter mutation | Also defines WHO Grade III in the 2021 classification; telomerase reactivation → limitless replicative potential |
| Loss of SMARCB1 | Chromatin remodeling complex loss; associated with rhabdoid/anaplastic variants |
| DNA methylation class | Six distinct methylation classes identified by genome-wide profiling; outperforms WHO histologic grade in predicting recurrence and survival |
The 2021 WHO CNS5 classification was the first to integrate molecular markers into meningioma grading: TERT promoter mutations and homozygous CDKN2A/B deletions now independently define Grade III, regardless of histology. The cIMPACT-NOW update 8 (2025) further proposes upgrading Grade I-morphology tumors to Grade II when 1p deletion co-occurs with 22q/NF2 alterations. - PMID 39212325
Quick Compendium of Clinical Pathology, 5th ed.; AJNR 2025 [PMID 38844366]
Hormonal Influence
- Meningiomas express estrogen receptors (ER) and progesterone receptors (PR)
- Female predominance, association with pregnancy, and increased growth with exogenous progestin use support a hormonal role in growth modulation
- However, clinical trials with tamoxifen (anti-estrogen) and mifepristone (PR antagonist/RU-486) have been disappointing - hormones modulate growth but are not primary drivers
- Somatostatin receptors are also expressed but somatostatin analogs have failed to show benefit
Bradley and Daroff's, p. 1561
Vascular Pathogenesis
- Meningiomas are highly vascular tumors supplied primarily by dural (meningeal) arteries
- Overexpression of VEGF contributes to tumor vascularity and peritumoral edema
- This has rationale for VEGF-targeted therapies (bevacizumab, sunitinib) in recurrent cases
- Vasogenic edema extent does not always correlate with tumor size but is more common around higher-grade and secretory variants
Summary Diagram (Conceptual)
Arachnoid cap cell
|
Initiating event
/ \
NF2 loss (~60%) NF2-wildtype (~40%)
(Chr 22q12) TRAF7, AKT1, SMO, KLF4, PIK3CA
|
Loss of MERLIN
|
↑Hippo → YAP/TAZ nuclear entry → proliferation
↑mTOR → growth
↑FAK → invasion
↑EGFR → sustained signaling
|
Grade I (benign)
|
+ del 1p, monosomy 14, del 9p21
+ TERT promoter mutation
+ CDKN2A/B homozygous deletion
|
Grade II / Grade III
Key references:
- Quick Compendium of Clinical Pathology 5th ed.
- Bradley and Daroff's Neurology in Clinical Practice
- Goldman-Cecil Medicine, Chapter 175
- 2025 AJNR molecular review (PMID 38844366)
- cIMPACT-NOW Update 8, 2025 (PMID 39212325)
- EANO guideline on molecular testing for meningioma (PMID 39577862)
This is a shared conversation. Sign in to Orris to start your own chat.