Meninges and types of meninges route of transmission
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
I now have comprehensive information to provide a detailed answer about the meninges and routes of transmission to them. Let me compile everything.
The Meninges: Anatomy, Types, and Routes of Infection
What Are the Meninges?
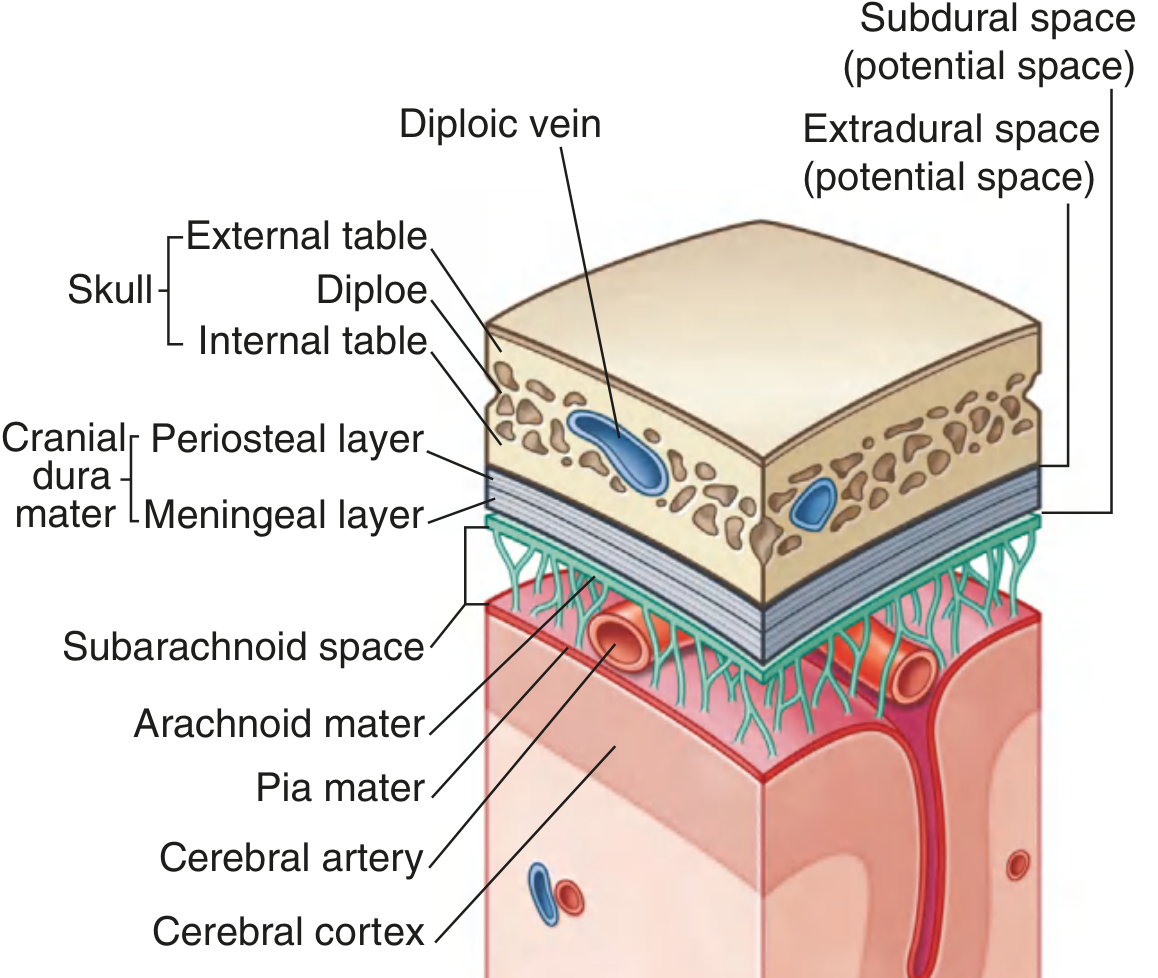
The meninges are three concentric layers of connective tissue that surround, protect, and suspend the brain and spinal cord within the cranial cavity and vertebral canal. The cranial meninges are continuous with the spinal meninges through the foramen magnum.
"The brain, as well as the spinal cord, is surrounded by three layers of membranes (the meninges) — a tough, outer layer (the dura mater), a delicate, middle layer (the arachnoid mater), and an inner layer firmly attached to the surface of the brain (the pia mater)." — Gray's Anatomy for Students
The Three Types of Meninges
1. Dura Mater ("Tough Mother")
- The thickest and most external layer; dense irregular connective tissue
- In the cranium, it has two fused layers:
- Outer periosteal layer — adherent to the skull, serves as cranial periosteum, contains meningeal arteries
- Inner meningeal layer — closely contacts the arachnoid mater; continuous with the spinal dura through the foramen magnum
- The two layers separate in certain regions to form:
- Dural venous sinuses (e.g., superior sagittal sinus) — receive cerebral venous drainage
- Dural partitions — falx cerebri, tentorium cerebelli, falx cerebelli, diaphragma sellae
- In the spine, the dura is a single meningeal layer separated from the vertebral periosteum by the epidural space (containing fat and venous plexuses)
- Innervation: Meningeal branches of CN V (V1, V2, V3), CN X (vagus), and C1–C3
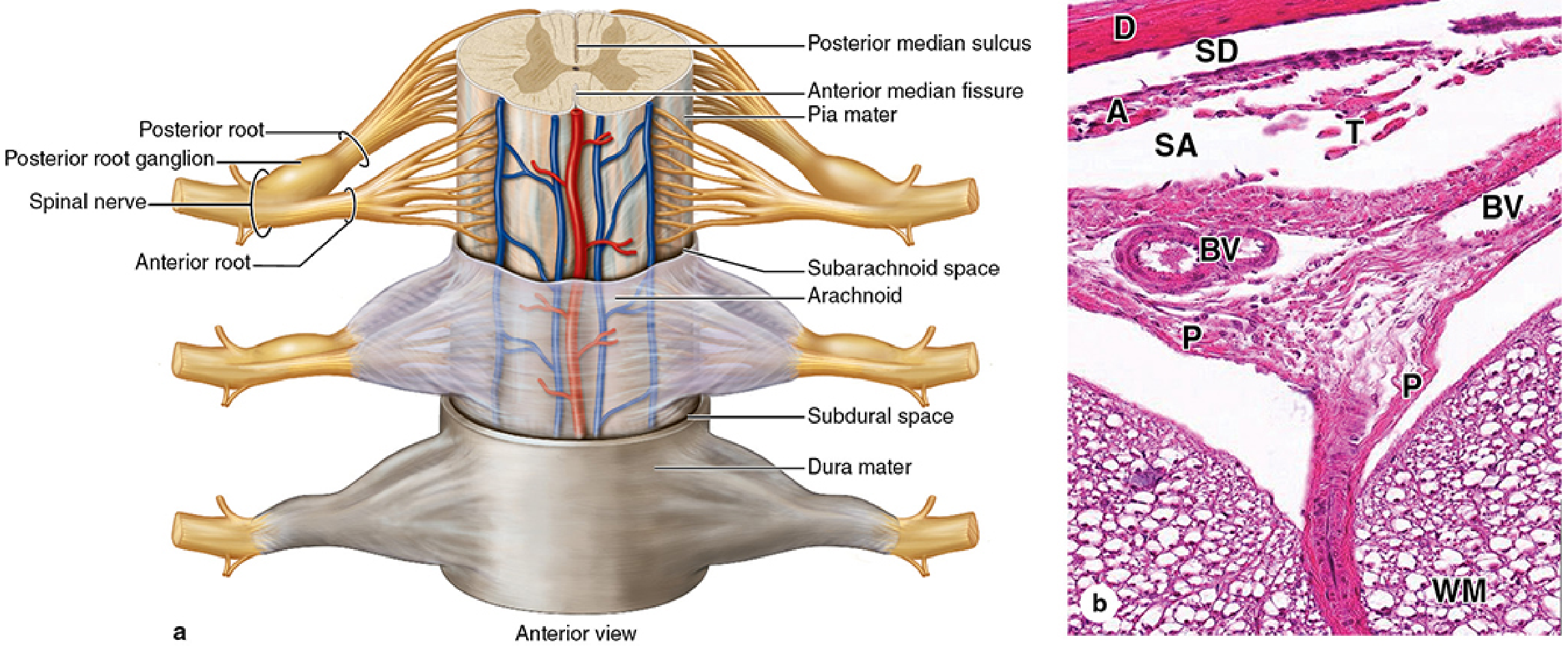
2. Arachnoid Mater ("Spider-web-like")
- A thin, avascular membrane lying against the inner surface of the dura (not adherent to it)
- Has two components:
- A sheet of connective tissue in contact with the dura
- A system of loose trabeculae (collagen + fibroblasts) extending to the pia mater
- Does not follow the brain's grooves/fissures (except the longitudinal fissure)
- Forms arachnoid villi — finger-like projections that penetrate dural venous sinuses and reabsorb CSF into the blood
- The arachnoid, not the dura, is the primary barrier to drug movement through the meninges
3. Pia Mater ("Tender/Delicate Mother")
- The innermost, thin, delicate membrane closely adherent to the entire surface of the brain and spinal cord
- Follows every groove and fissure (unlike the arachnoid)
- Not in direct contact with nerve cells — separated from neural elements by the glial limiting membrane (astrocytic end feet)
- Blood vessels travel through perivascular channels covered by pia; lose this covering at the capillary level
Meningeal Spaces
| Space | Location | Type | Clinical Significance |
|---|---|---|---|
| Extradural (epidural) | Between dura and bone | Potential (cranial); Real (spinal) | Epidural hematoma (meningeal artery rupture); epidural anesthesia |
| Subdural | Between dura and arachnoid (dural border cell layer) | Potential | Subdural hematoma (tearing of bridging veins) |
| Subarachnoid | Between arachnoid and pia | Real, fluid-filled | Contains CSF + blood vessels; site of SAH; LP samples fluid here |
The subarachnoid space contains CSF (produced by the choroid plexus in the ventricles) and enlarges in certain areas into subarachnoid cisterns.
Routes of Transmission / Infection of the Meninges
Meningitis (inflammation of the meninges) results from pathogens reaching the meningeal space via several routes:
1. Hematogenous (Bloodstream) Route — Most Common
- The primary pathway for most bacterial meningitides
- Sequence: colonization of nasopharynx → mucosal invasion → bacteremia → crossing the blood-brain barrier (BBB) into the subarachnoid space
- Examples:
- Streptococcus pneumoniae, Neisseria meningitidis, Haemophilus influenzae type b (Hib) — all gain entry via respiratory tract colonization then bacteremia
- Hib specifically: "causes systemic disease by invasion and hematogenous spread from the respiratory tract to distant sites such as the meninges" — Harrison's Principles of Internal Medicine
- Enteroviruses (most common cause of viral meningitis) also spread hematogenously
2. Direct Extension (Contiguous Spread)
- Infection spreads from an adjacent infected structure directly through bone and dura into the meningeal space
- Sources:
- Sinusitis (especially frontal, ethmoid) → anterior cranial fossa meninges
- Otitis media / mastoiditis → posterior cranial fossa / temporal meninges
- Dental/pharyngeal abscess → contiguous spread
- Subdural empyema: "infection gains entry to the subdural space by direct extension through bone and dura, or by spread from septic thrombosis of the venous sinuses" — Adams and Victor's Principles of Neurology
3. Trauma / Anatomical Defects
- Skull fractures, particularly basilar skull fractures with CSF rhinorrhoea/otorrhoea, create a direct communication between the external environment and the subarachnoid space
- Neurosurgical procedures, lumbar puncture (if not aseptic)
- Congenital defects (e.g., meningomyelocele)
4. CSF Hardware / Iatrogenic
- Ventriculoperitoneal shunts and other CSF devices dramatically increase infection risk
- Common pathogens: coagulase-negative staphylococci, Cutibacterium acnes, gram-negative enteric organisms
5. Neural / Perineural Route
- Some pathogens travel along cranial or peripheral nerves
- Examples:
- Herpes simplex virus — travels retrogradely along trigeminal nerve
- Naegleria fowleri (free-living amoeba) — ascends via the olfactory nerve through the cribriform plate to reach the subarachnoid space (causes primary amoebic meningoencephalitis)
6. Septic Venous Thrombophlebitis
- Infected thrombus in a dural venous sinus (e.g., cavernous sinus thrombosis from facial/orbital infections) can spread infection to the subdural or subarachnoid space
Summary Table
| Route | Examples | Key Pathogens |
|---|---|---|
| Hematogenous | Nasopharyngeal colonization → bacteremia | S. pneumoniae, N. meningitidis, Hib, enteroviruses |
| Direct extension | Sinusitis, otitis, mastoiditis | Mixed flora, anaerobes |
| Trauma/defect | Skull fracture, post-surgical | S. aureus, gram-negatives |
| CSF hardware | VP shunts | CoNS, C. acnes, enteric GNR |
| Perineural | Olfactory nerve, trigeminal nerve | Naegleria, HSV |
| Venous sinuses | Cavernous sinus thrombosis | Mixed |
Sources: Gray's Anatomy for Students | Junqueira's Basic Histology, 17e | Harrison's Principles of Internal Medicine, 22e | Adams and Victor's Principles of Neurology | Tietz Textbook of Laboratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.