Ventilation and perfusion and it's inequality full details for md exam answer 15 marks from fishman and Murray combined structured condensed
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed from both Fishman and Murray. Let me compose the comprehensive MD exam answer.
Ventilation, Perfusion, and V/Q Inequality
MD Exam Answer - 15 Marks
Sources: Fishman's Pulmonary Diseases & Disorders (Fishman) + Murray & Nadel's Textbook of Respiratory Medicine (Murray)
1. DEFINITIONS AND NORMAL VALUES
Alveolar ventilation (VA): The volume of fresh gas reaching the alveoli per minute, normally ~4-5 L/min at rest.
Pulmonary perfusion (Q): Total pulmonary blood flow, equal to cardiac output, normally ~5 L/min at rest.
V/Q ratio: The ratio of alveolar ventilation to perfusion for any lung unit. The whole-lung mean V/Q ratio is approximately 0.8-1.0 (since VA ~4 L/min and Q ~5 L/min).
At extremes:
- V/Q = 0 (perfusion but no ventilation) → unit behaves as intrapulmonary shunt; end-capillary blood has the same composition as mixed venous blood
- V/Q = ∞ (ventilation but no perfusion) → unit behaves as alveolar dead space; alveolar gas has the same composition as inspired gas
2. THE O2-CO2 DIAGRAM AND THE V/Q LINE
(Murray & Nadel, Chapter 10)
The behavior of any single lung unit is elegantly captured by the oxygen-carbon dioxide diagram. For any given inspired gas (I) and mixed venous blood (V̄), all possible combinations of alveolar PO2 and PCO2 lie on a single curve - the ventilation-perfusion line.
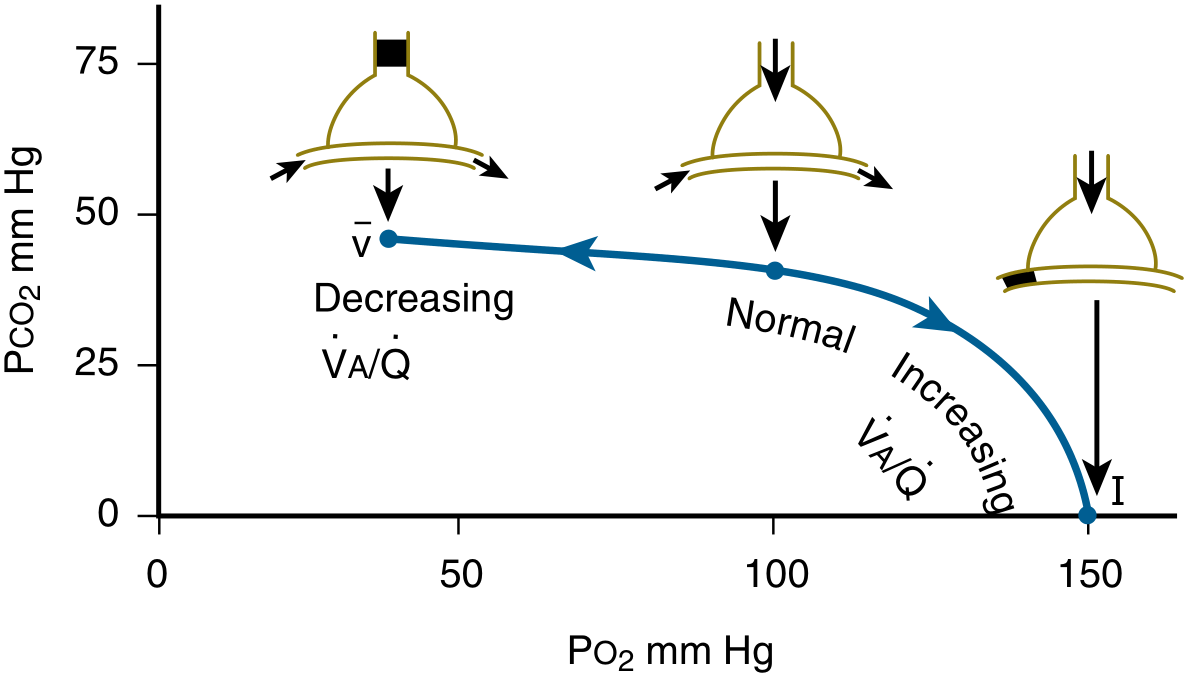
Figure: The V/Q line - each point uniquely corresponds to a V/Q ratio. V̄ = mixed venous blood; I = inspired gas.
Key relationships derived from mass conservation equations (Murray Eqs. 29 & 30):
For CO2:
$$\frac{\dot{V}A}{\dot{Q}} = K \times \frac{(C\bar{v}{CO_2} - Cc'{CO_2})}{P{ACO_2}}$$
For O2:
$$\frac{\dot{V}A}{\dot{Q}} = K \times \frac{(Cc'{O_2} - C\bar{v}{O_2})}{(P{IO_2} - P_{AO_2})}$$
The alveolar PO2 and PCO2 are thus determined by three factors: (1) the V/Q ratio, (2) composition of inspired gas and mixed venous blood, and (3) the relevant blood-gas dissociation curves.
Practical consequence: When V/Q falls below normal, PO2 falls and PCO2 rises in that unit; when V/Q rises above normal, PO2 rises and PCO2 falls.
3. REGIONAL DISTRIBUTION OF VENTILATION AND PERFUSION IN THE NORMAL LUNG
3a. Gravity-Based Inequality (the dominant mechanism)
(Fishman, Chapter 14; Murray, Chapter 10)
In the upright lung, both ventilation and blood flow increase from apex to base - but the gradient for blood flow far exceeds that for ventilation. This is because:
- Ventilation gradient: Due to the weight of the lung parenchyma, pleural pressure is less negative (more positive) at the base. Basal alveoli sit on a steeper part of the pressure-volume curve and expand more per unit pressure change.
- Perfusion gradient: Due to hydrostatic pressure of blood in the pulmonary vessels. Pulmonary arterial pressure at the base is ~25 cmH2O higher than at the apex.
Result: The V/Q ratio rises exponentially from base to apex:
- Apex (Region 9): V/Q ~3.0 (high V/Q; relative dead space behavior; PO2 high ~130 mmHg, PCO2 low ~28 mmHg)
- Base (Region 1): V/Q ~0.6 (low V/Q; relative shunt behavior; PO2 low ~89 mmHg, PCO2 high ~42 mmHg)
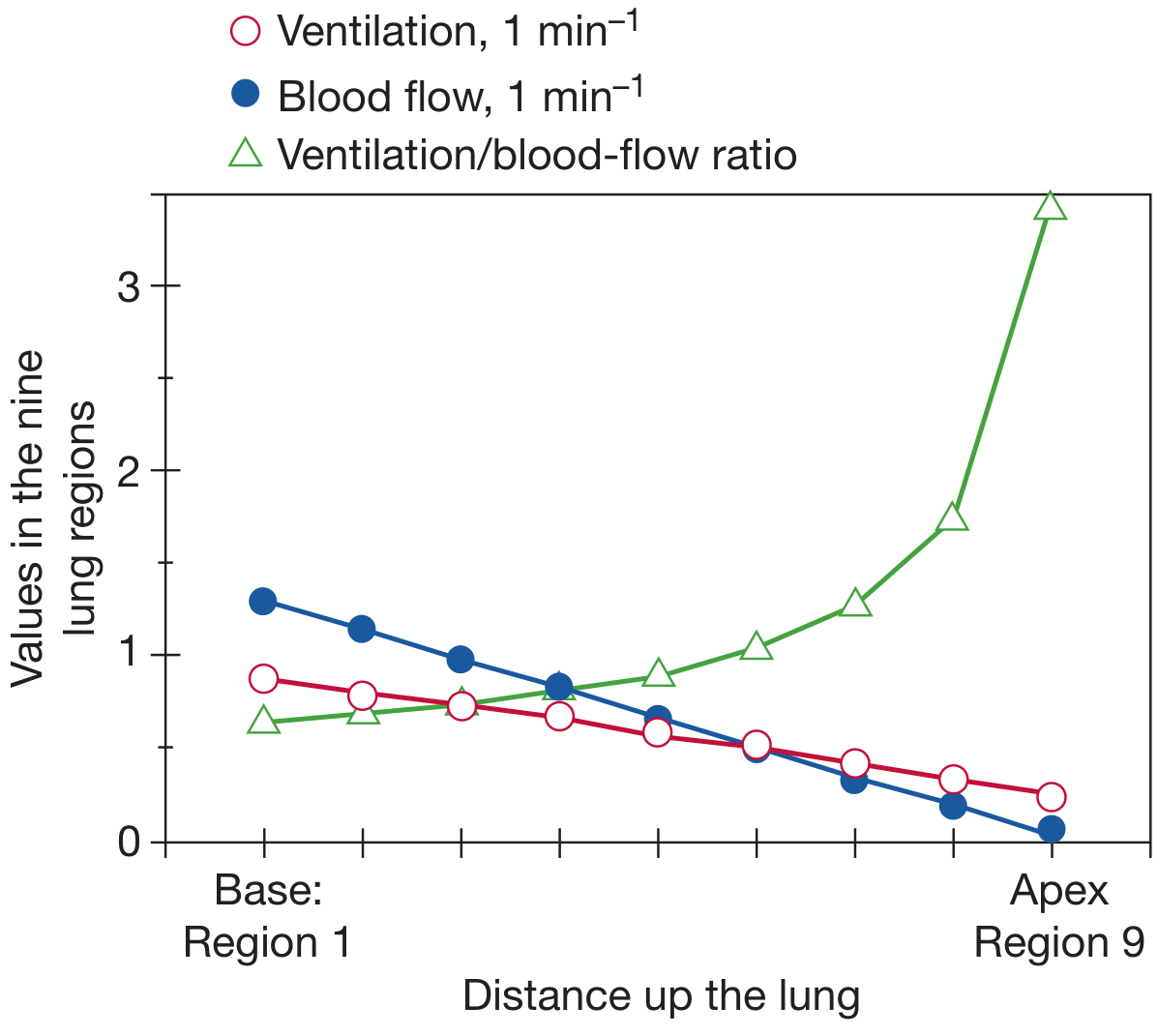
Figure: Topographic V/Q distribution in the upright lung (adapted from West). The V/Q gradient from base to apex is approximately 5-fold.
This normal gravitational gradient produces only about a 4 mmHg drop in arterial PO2 (i.e., a 4 mmHg alveolar-arterial PO2 difference).
West's Zones of the Lung (Perfusion)
The pulmonary circulation is a low-pressure system. The relationship between pulmonary arterial pressure (Pa), alveolar pressure (PA), and pulmonary venous pressure (Pv) defines three zones:
| Zone | Condition | Flow Status |
|---|---|---|
| Zone 1 (Apex) | PA > Pa > Pv | No flow (alveolar dead space); seen only in hemorrhage or positive-pressure ventilation |
| Zone 2 (Mid) | Pa > PA > Pv | Flow determined by Pa - PA ("waterfall" effect) |
| Zone 3 (Base) | Pa > Pv > PA | Flow determined by Pa - Pv (venous pressure-dependent, greatest flow) |
3b. Fractal-Based Inequality
(Fishman, Chapter 14)
The dichotomously branching airway and vascular tree constitutes a fractal system inherently prone to V/Q inequality independent of gravity. A trivially asymmetric 49:51 split at each of 16 consecutive branch points results in a nearly 2-fold difference in ventilation between the best- and worst-ventilated terminal units. However, the lung must correlate VA and Q distribution through the same branching structure, otherwise the resultant hypoxemia would be far greater than is observed clinically.
3c. Longitudinal (Acinar) Inequality
As airways and blood vessels narrow with each branch generation, resistance increases. Alveoli at different distances from the terminal bronchiole receive different amounts of ventilation and blood flow, creating further small-scale V/Q heterogeneity within the acinus.
3d. Compensatory Mechanisms
(i) Hypoxic pulmonary vasoconstriction (HPV): Local alveolar hypoxia (from low V/Q) triggers O2-sensitive K⁺ channel-mediated constriction of pulmonary arterioles, reducing blood flow to the hypoxic region and redirecting it to better-ventilated zones. This partially normalizes local V/Q. Prolonged HPV can cause pulmonary hypertension and right heart failure.
(ii) Hypocapnic bronchoconstriction: When V/Q rises (e.g., pulmonary embolism), local PCO2 falls and triggers bronchoconstriction, reducing ventilation to that area and tending to normalize V/Q.
4. V/Q INEQUALITY: CONCEPT AND DEFINITION
(Fishman, Chapter 14)
V/Q inequality exists whenever the V/Q ratio is not identical in all lung units - i.e., there is a distribution (range) of V/Q ratios across the lung. The pathologic cause (airway disease vs. vascular disease) is irrelevant to the concept.
Key principle: Compared with a perfectly homogeneous lung with the same total ventilation and blood flow, a lung with V/Q inequality exchanges all gases inefficiently, resulting in hypoxemia and potentially hypercapnia.
V/Q inequality can manifest at multiple scales:
- Large-scale: Whole-lung differences (e.g., unilateral atelectasis, pneumonia, pneumothorax, massive pulmonary embolism)
- Medium-scale: Segmental or subsegmental (e.g., COPD, asthma, pulmonary fibrosis)
- Small-scale: Adjacent alveolar units; however, rapid diffusion and collateral ventilation tend to maintain homogeneity at this level
Even the normal young lung has mild V/Q inequality, explaining the normal 5-10 mmHg alveolar-arterial PO2 difference.
5. EFFECTS OF V/Q INEQUALITY ON GAS EXCHANGE
5a. Effect on PO2 (Hypoxemia)
(Murray, Chapter 10; Fishman, Chapter 14)
The critical reason V/Q inequality causes hypoxemia is the nonlinear shape of the oxyhemoglobin dissociation curve:
- High V/Q units have high PO2, but the Hb is already nearly fully saturated - so the extra O2 carried is trivial.
- Low V/Q units have low PO2 and low Hb saturation, significantly reducing O2 content.
When blood from high and low V/Q units mixes, the high-V/Q blood cannot compensate for the low-V/Q blood, because:
- Blood O2 content cannot exceed ~20 mL/100 mL regardless of PO2 (flat part of curve)
- But O2 content falls steeply at low PO2 (steep part of curve)
Net result: Mixed arterial blood PO2 is pulled down toward the low V/Q units. The resulting A-a gradient for O2 is widened.
Additionally, the PO2 of "ideal alveolar gas" (calculated from the alveolar gas equation) is higher than measured arterial PO2, yielding the A-a gradient (PAO2 - PaO2).
In contrast, breathing 100% O2 abolishes hypoxemia from V/Q mismatch (but not from true shunt), because even low-V/Q units receive enough O2 to fully saturate Hb.
5b. Effect on PCO2 (Hypercapnia or Normocapnia)
(Murray, Chapter 10; Fishman, Chapter 14)
CO2 dissociation curve behavior is quite different from O2:
- The CO2 dissociation curve is nearly linear over the physiologic range (steep slope ~10x that of O2)
- This means high-V/Q units can blow off extra CO2 efficiently, and low-V/Q units retain extra CO2
Consequence: V/Q inequality does NOT automatically cause CO2 retention in clinical practice, because:
- The central chemoreceptors respond to any rise in PaCO2
- Increased total ventilation (hyperventilation) can compensate by increasing CO2 elimination from high-V/Q units
- This extra ventilation barely raises O2 (because Hb is already near-saturated)
Therefore, in most patients with V/Q mismatch:
- PaO2 is low (hypoxemia - cannot be compensated)
- PaCO2 is normal or low (due to reflex hyperventilation)
- The A-a gradient for O2 is widened
CO2 retention does occur when:
- Ventilatory reserve is exhausted (severe disease)
- Respiratory muscle fatigue prevents compensatory hyperventilation
- V/Q inequality is extreme (very large dead space fraction)
5c. Summary of V/Q Inequality Effects (Fishman, Chapter 14)
V/Q inequality:
- Affects both O2 and CO2 exchange, regardless of pathologic basis
- Causes arterial hypoxemia (invariably) and potentially hypercapnia (when compensation fails)
- Causes more severe hypoxemia than hypercapnia (asymmetry due to dissociation curve shapes)
- Has greater effect on O2 than CO2 when very low V/Q regions predominate (airway obstruction)
- Has greater effect on CO2 than O2 when very high V/Q regions predominate (vascular obstruction/dead space)
- Impairs total O2 and CO2 exchange by the lung
- Creates alveolar-arterial differences for both gases
6. THREE-COMPARTMENT MODEL (RILEY AND COURNAND)
(Murray, Chapter 10)
For clinical purposes, the lung is conceptually divided into three compartments:
| Compartment | V/Q | Represents |
|---|---|---|
| Shunt (Qs) | = 0 | Unventilated, perfused alveoli; contributes venous admixture |
| Ideal alveolus | Normal | Perfectly matched V/Q |
| Dead space (Vd) | = ∞ | Ventilated, unperfused alveoli; wasted ventilation |
Physiologic dead space (Bohr equation):
$$\frac{V_D}{V_T} = \frac{P_aCO_2 - P_{\bar{E}}CO_2}{P_aCO_2}$$
Normal VD/VT < 0.3.
Venous admixture (physiologic shunt):
$$\frac{\dot{Q}_s}{\dot{Q}_T} = \frac{Cc'O_2 - CaO_2}{Cc'O_2 - C\bar{v}O_2}$$
where Cc'O2 = end-capillary O2 content (ideal alveolus), CaO2 = arterial O2 content, CvO2 = mixed venous O2 content. Normal Qs/Qt < 5%.
This "virtual shunt fraction" summarizes how much of the hypoxemia is attributable to low-V/Q regions, as if all were due to a single shunt.
7. QUANTITATIVE MEASUREMENT OF V/Q DISTRIBUTION
7a. Traditional Indices (Fishman & Murray)
(1) Alveolar-arterial PO2 difference (A-a gradient):
$$P_{AO_2} - P_{aO_2} = \left[P_{IO_2} - \frac{P_{aCO_2}}{R} + P_{aCO_2} \cdot F_{IO_2} \cdot \frac{(1-R)}{R}\right] - P_{aO_2}$$
Normal (breathing air): <10-15 mmHg (young); increases with age (~0.3 mmHg/year). Widened in V/Q mismatch, shunt, and diffusion impairment (not in pure hypoventilation).
Limitations: Sensitive to FiO2 and overall ventilation; value of R must be assumed.
(2) PaO2/FiO2 ratio: Useful bedside index; normal ~400-500 mmHg; <300 = acute lung injury; <200 = ARDS. Relatively insensitive to FiO2 changes.
(3) Venous admixture (Qs/Qt): Already described above. Expressed as % of cardiac output.
(4) Physiologic dead space (VD/VT): Reflects high-V/Q regions; useful in monitoring ventilatory efficiency.
7b. Multiple Inert Gas Elimination Technique (MIGET)
(Murray, Chapter 10; Fishman, Chapter 14)
Introduced by Wagner et al., MIGET is the gold standard research technique for measuring the actual distribution of V/Q ratios. It involves:
- Infusing a mixture of 6 inert gases of varying blood-gas solubility (from SF6 to acetone)
- Measuring their retention in arterial blood and elimination in expired gas
- Computing the distribution of ventilation and perfusion across a spectrum of V/Q ratios (0 to ∞)
Findings in normal subjects: A narrow unimodal distribution spanning approximately one log decade of V/Q ratios (0.3 to 3.0). No true shunt detected (because even small shunts, ~0.5% of Qt, would double arterial SF6 concentration). The A-a gradient in normal subjects is entirely explained by this narrow V/Q heterogeneity.
Findings in disease:
- COPD (emphysema type): Bimodal distribution with large amounts of ventilation to very high V/Q units (alveolar dead space); small shunt; predominantly hypoxemia from high dead space
- COPD (chronic bronchitis type): Blood flow shifted to low V/Q units; moderate shunt; more severe hypoxemia and tendency to CO2 retention
- Asthma (acute): Blood flow to low V/Q units; V/Q distribution shifts leftward
- Pulmonary fibrosis: Broadened distribution; diffusion limitation also contributes at exercise
- Pneumonia, atelectasis: True shunt (V/Q = 0)
8. V/Q MISMATCH IN SPECIFIC DISEASES
| Disease | Predominant V/Q Pattern | Gas Exchange Effect |
|---|---|---|
| COPD (emphysema) | High V/Q (dead space ↑) | Mild hypoxemia, hypocapnia or normocarbia |
| COPD (bronchitis) | Low V/Q (shunt-like) | Hypoxemia + CO2 retention (Blue Bloater) |
| Asthma (acute) | Low V/Q regions | Hypoxemia; PaCO2 initially low then rises |
| Pulmonary embolism | High V/Q (Zone 1 expansion) | Hypoxemia; hypocapnia; dead space ↑ |
| Pneumonia/atelectasis | True shunt (V/Q = 0) | Refractory hypoxemia; not corrected by O2 |
| Pulmonary fibrosis | Broadened distribution + diffusion limitation | Hypoxemia, especially on exercise |
9. COMPENSATION AND CLINICAL SIGNIFICANCE
Response to Hyperoxia (O2 therapy)
- V/Q mismatch: Hypoxemia corrects with supplemental O2 (even low-V/Q units receive enough O2 eventually)
- True shunt (V/Q = 0): Hypoxemia does not correct even with 100% O2 (blood bypasses alveoli entirely)
This distinction is clinically important: failure to raise PaO2 with 100% O2 points to a true intracardiac or intrapulmonary shunt.
Increased Minute Ventilation
Hypoxemic drive and hypercapnic drive (if CO2 rises) stimulate chemoreceptors, increasing minute ventilation. This preferentially removes CO2 (linear dissociation curve) but barely improves O2 (flat dissociation curve at high saturation). Hence patients with V/Q mismatch often present with:
- Low PaO2 (uncorrected)
- Normal or low PaCO2 (corrected by hyperventilation)
- Widened A-a gradient
HPV as a Clinical Tool
HPV helps match perfusion to ventilated regions. Its inhibition by vasodilators (sildenafil, nitric oxide, calcium channel blockers) can worsen V/Q matching and paradoxically worsen hypoxemia in COPD patients.
10. SUMMARY TABLE
| Parameter | Normal | V/Q Inequality | True Shunt | Pure Dead Space |
|---|---|---|---|---|
| PaO2 | Normal | Decreased | Severely decreased | Variable |
| PaCO2 | Normal | Normal/Low* | Normal | Increased |
| A-a gradient | <15 mmHg | Widened | Widened | Normal |
| Response to O2 | - | Corrects | Does NOT correct | Corrects |
| Qs/Qt | <5% | Increased | Greatly increased | Normal |
| VD/VT | <0.30 | Increased | Normal | Greatly increased |
*PaCO2 normal/low because hyperventilation compensates
KEY POINTS FOR EXAM
- V/Q mismatch is the most common cause of hypoxemia in lung disease (Murray & Nadel)
- The V/Q ratio ranges from 0 (pure shunt) to ∞ (pure dead space); normal mean ~0.8
- In the upright lung: apex V/Q ~3, base V/Q ~0.6 (5-fold gradient); blood flow gradient exceeds ventilation gradient
- Hypoxemia from V/Q mismatch is due to the nonlinear O2 dissociation curve - high V/Q units cannot compensate for low V/Q units
- CO2 retention from V/Q mismatch is usually compensated by hyperventilation (linear CO2 curve allows compensation)
- The A-a gradient is the key clinical tool; widens in V/Q mismatch, shunt, and diffusion impairment
- MIGET is the gold standard research tool; shows normal lungs have narrow unimodal V/Q distribution without true shunt
- Hypoxic pulmonary vasoconstriction is the key compensatory mechanism, redirecting flow from low-V/Q to normal areas
- Responding to 100% O2 distinguishes V/Q mismatch (corrects) from true shunt (does not correct)
- West's Zones explain why Zone 1 (apex) is physiologic dead space territory and Zone 3 (base) has highest flow
Sources: Fishman's Pulmonary Diseases and Disorders, Chapter 14 (V/Q Relationships and Gas Exchange) | Murray & Nadel's Textbook of Respiratory Medicine, Chapter 10 (Gas Exchange)
This is a shared conversation. Sign in to Orris to start your own chat.