Tell me about ankylosing spondylitis all thing including treatment in deep
Reading File
Finding Sources
Searching PubMed
"ankylosing spondylitis"[MeSH Terms] AND treatment
Searching the Web
ankylosing spondylitis 2024 2025 treatment guidelines biologics
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information to write a thorough answer. Let me compile everything.
Ankylosing Spondylitis (AS) - A Complete Guide
Overview and Nomenclature
Ankylosing spondylitis (AS) is a chronic, immune-mediated inflammatory disease that primarily targets the axial skeleton - the sacroiliac (SI) joints and spine. It belongs to the broader family of spondyloarthropathies (SpAs), and is now frequently referred to as radiographic axial spondyloarthritis (r-axSpA) under the newer ASAS classification, to distinguish it from non-radiographic axial SpA (nr-axSpA), which shares the same disease biology but has not yet shown structural damage on plain X-ray.
The term "ankylosing" means fusion (ankylosis), and "spondylitis" means inflammation of the spine - together describing its hallmark: progressive spinal inflammation leading to new bone formation and eventual fusion.
Epidemiology
- Prevalence roughly 0.1-1.4% in Western populations; varies with HLA-B27 frequency
- Onset typically in adolescents and young adults (usually before age 45)
- Historically thought to be male-predominant (3:1), but modern data suggest women are equally affected though often diagnosed later due to milder radiographic changes
- Sibling recurrence risk: ~9.2% vs. 0.1-0.4% in the general population, with heritability estimated >95%
Pathogenesis and Genetics
HLA-B27 - The Key Genetic Factor
90% of White AS patients carry HLA-B27, compared to ~8% of unaffected individuals, giving a relative risk of 50-100 or higher. Despite this strong association, only ~2% of HLA-B27-positive individuals develop AS, confirming that additional genetic and environmental factors are required.
Three major hypotheses explain how HLA-B27 drives disease:
- Arthritogenic peptide hypothesis - HLA-B27 presents self-peptides to cytotoxic T cells, triggering autoreactivity
- HLA-B27 misfolding hypothesis - misfolded heavy chains accumulate in the ER, inducing an unfolded protein response and IL-23 production
- HLA-B27 homodimer hypothesis - surface homodimers activate NK and T cells
Beyond HLA-B27
Over 80 additional risk loci have been identified, including:
- ERAP1/ERAP2 - aminopeptidase genes involved in peptide trimming for HLA presentation (ERAP1 only associates in HLA-B27-positive patients - a classic example of genetic epistasis)
- IL-23R, IL-12B, IL-27 - genes in the IL-23/IL-17 axis, explaining why IL-17 inhibitors work in AS
- Notably, IL-23 inhibitors (e.g. risankizumab, ustekinumab) have failed in AS trials despite working in psoriasis and IBD - suggesting the pathogenic IL-17 in AS may be driven by an IL-23-independent, innate-like lymphocyte pathway
Clinical Features
Axial (Spinal and SI Joint) Disease
The hallmark presentation is chronic inflammatory back pain, with these distinguishing features:
- Onset before age 45
- Insidious onset over weeks to months
- Morning stiffness lasting >60 minutes
- Improvement with exercise, NOT with rest
- Nocturnal pain (often waking the patient in the second half of the night)
- Alternating buttock pain (suggesting SI joint involvement)
Peripheral Joint Involvement
Up to 30% of patients develop peripheral arthritis. The hip is the second most common joint after the SI joint, and hip involvement is a marker of more severe disease. Peripheral arthritis is typically asymmetric oligoarthritis affecting lower limbs.
Enthesitis
Inflammation at sites of tendon and ligament insertion into bone:
- Achilles tendon insertion
- Plantar fascia
- Iliac crests
- Tibial tuberosities
- Elbow epicondyles
Extra-Articular Manifestations
| Manifestation | Notes |
|---|---|
| Anterior uveitis | Most common (25-40%); unilateral, acute, painful red eye - a rheumatological emergency |
| Inflammatory bowel disease | ~10% have Crohn's or UC; microscopic gut inflammation in up to 60% |
| Psoriasis | ~10% |
| Aortitis / Aortic regurgitation | Rare but serious; due to inflammation of aortic root |
| Cardiac conduction defects | AV block |
| Apical pulmonary fibrosis | Bilateral upper lobe fibrobullous disease - no effective treatment |
| IgA nephropathy | Uncommon |
| Amyloidosis (AA type) | Rare, secondary to chronic inflammation |
| Osteoporosis / spinal fractures | Paradoxically, the rigid ankylosed spine is highly prone to catastrophic transverse fractures even with minor trauma |
Imaging
Plain Radiography
The earliest radiographic sign is sacroiliitis - bilateral and symmetric in AS (unlike psoriatic arthritis, which is asymmetric). Graded 0-4:
- Grade 0: Normal
- Grade 1: Suspicious
- Grade 2: Erosions + sclerosis
- Grade 3: Definite erosions with sclerosis and partial ankylosis
- Grade 4: Complete fusion
Spinal changes (lateral lumbar/thoracic views):
- Shiny corner sign / Romanus lesions - sclerosis at vertebral corners from enthesitis at Sharpey fiber insertions
- Squared vertebral bodies - from erosion and anterior longitudinal ligament ossification
- Syndesmophytes - thin, vertical bone outgrowths bridging vertebral bodies (distinguishable from the coarser, non-marginal syndesmophytes of psoriatic/reactive arthritis and the horizontal osteophytes of degenerative disease)
- Bamboo spine - complete fusion of vertebral bodies and facet joints (end-stage)
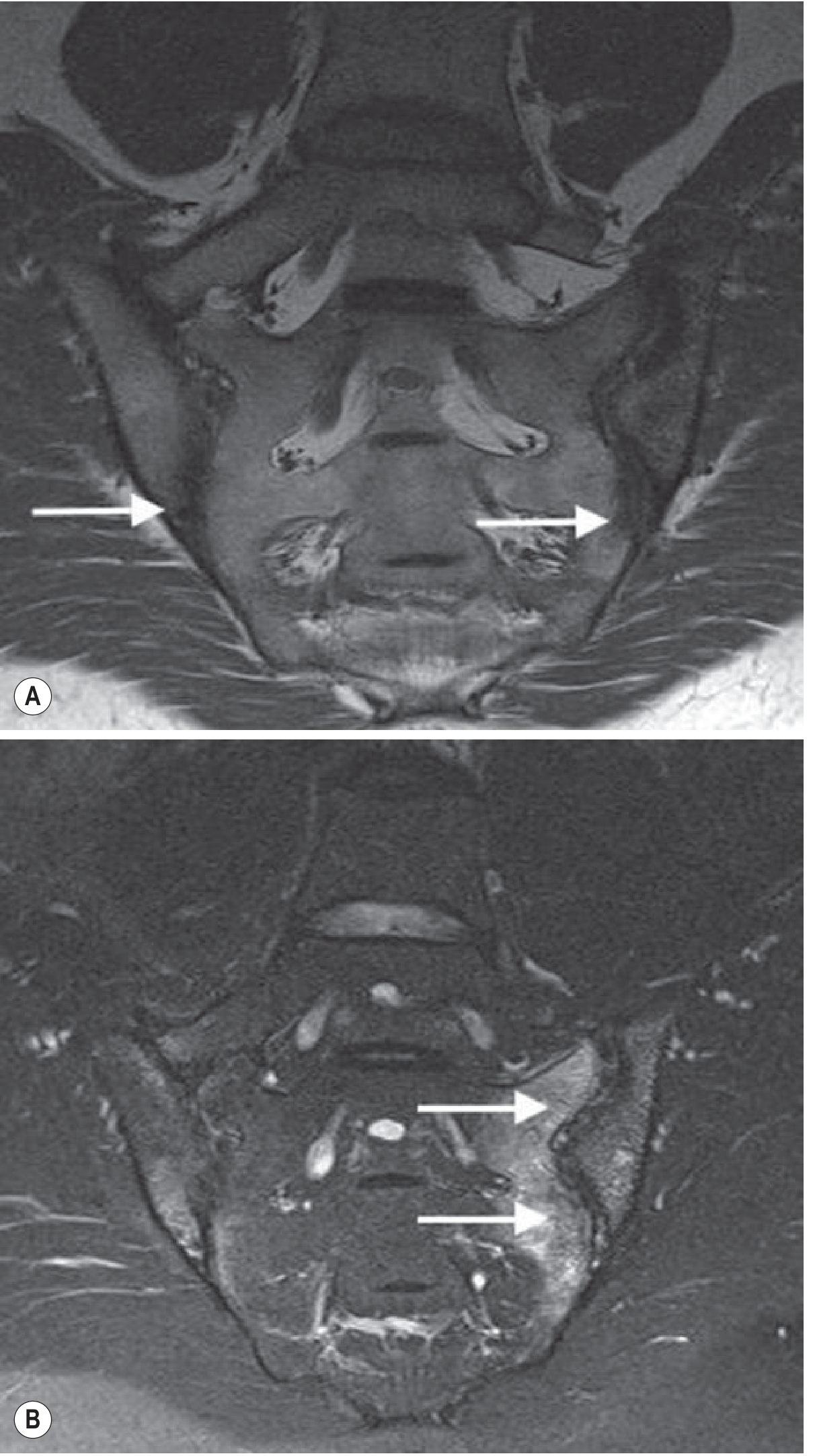
MRI of sacroiliac joints in AS: T1-weighted (A) shows erosions and joint space loss; T2 fat-suppressed (B) shows extensive subchondral bone marrow oedema reflecting disease activity. (Grainger & Allison's Diagnostic Radiology)
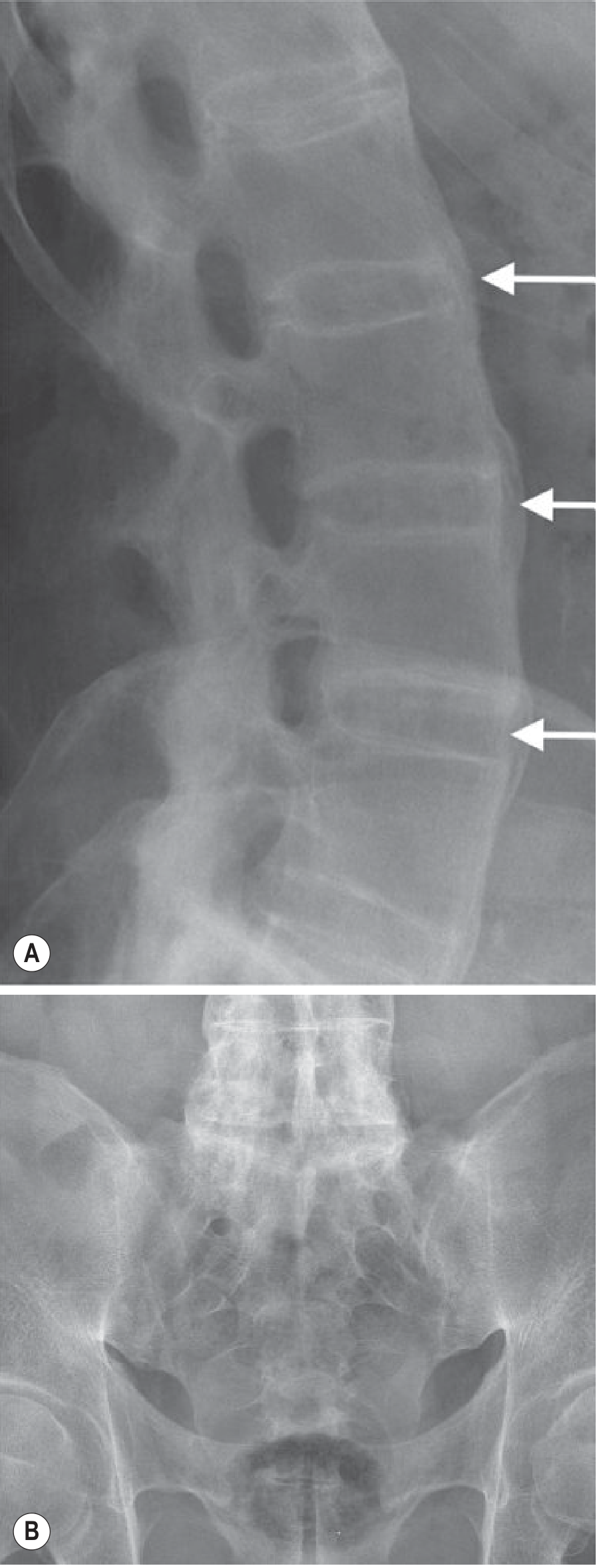
Advanced AS: (A) Bridging vertical syndesmophytes (arrows) around intervertebral discs with no visible facet joint spaces (posterior fusion L3-S1). (B) Complete bilateral fusion of the sacroiliac joints. Classic "bamboo spine" appearance. (Grainger & Allison's Diagnostic Radiology)
MRI
MRI is the most sensitive modality for early disease detection, showing bone marrow oedema (BME) before any radiographic change appears. The ASAS definition requires active sacroiliitis on MRI to include characteristic subchondral BME. MRI also detects costovertebral, facet joint, and posterior element enthesitis.
CT
Excellent for showing structural damage (erosions, sclerosis, ankylosis), particularly in the SI joints. Less favored due to radiation, but useful for spinal fracture assessment.
Diagnosis and Classification
Modified New York Criteria (1984) - for AS
Clinical criteria:
- Low back pain and stiffness >3 months, improving with exercise, not relieved by rest
- Limitation of lumbar spine motion in both sagittal and frontal planes
- Limitation of chest expansion relative to normal values for age and sex
Radiological criterion:
- Bilateral sacroiliitis grade 2-4, OR unilateral sacroiliitis grade 3-4
Definite AS = radiological criterion + ≥1 clinical criterion
ASAS Classification Criteria (2009) - for axial SpA (broader)
For patients with chronic back pain ≥3 months with age of onset <45:
- Imaging arm: Sacroiliitis on MRI or X-ray + ≥1 SpA feature
- Clinical arm: HLA-B27 positive + ≥2 SpA features
SpA features include: inflammatory back pain, arthritis, enthesitis, uveitis, dactylitis, psoriasis, IBD, good response to NSAIDs, family history of SpA, elevated CRP
Laboratory Tests
- HLA-B27: Positive in >90% of White AS patients; useful for diagnosis but not sufficient alone
- CRP / ESR: Elevated in only 50-60% of patients; ESR and CRP often correlate poorly with disease activity, but elevated CRP is a risk factor for radiographic progression
- No specific autoantibodies - RF and ANA are typically negative (hence "seronegative")
Disease Activity Scores
- BASDAI (Bath Ankylosing Spondylitis Disease Activity Index) - patient-reported; scores six domains; ≥4 = active disease
- ASDAS (Ankylosing Spondylitis Disease Activity Score) - incorporates CRP or ESR; preferred in guidelines
- <1.3 = inactive disease
- 1.3-2.1 = low disease activity
- 2.1-3.5 = high disease activity
-
3.5 = very high disease activity
Treatment
Treatment follows a stepwise approach based on disease activity, guided by ASAS-EULAR (2022 update) and ACR/SAA/SPARTAN (2019 update) guidelines.
Step 1: Non-Pharmacologic Therapy
Physical therapy and exercise are the cornerstone of AS management and should continue throughout the disease course, regardless of pharmacologic treatment. Goals include:
- Maintaining spinal mobility and posture
- Strengthening axial and peripheral muscles
- Improving chest expansion and respiratory function
Exercise regimens combine cervical extension and rotation, thoracic extension, breathing exercises, and hip/pelvic mobility work. Supervised physiotherapy is superior to unsupervised home exercise. Hydrotherapy is also beneficial.
Patient education regarding posture, ergonomics, and disease management is essential.
Step 2: NSAIDs - First-Line Pharmacologic Therapy
NSAIDs remain the first-line pharmacologic treatment for active AS with no contraindications. Key points:
- No single NSAID is preferred over another; evidence shows most are equally effective for axial disease
- Full dose is often needed; response is typically seen within 2 weeks
- If first NSAID fails, try a second NSAID before escalating to biologics
- For nocturnal symptoms, a long-acting nighttime formulation may be sufficient
- Extended-release formulations provide better overnight coverage
Studied NSAIDs and doses:
| Drug | Dosage | Notes |
|---|---|---|
| Indomethacin | Up to 150 mg/day | Traditional first choice |
| Diclofenac | Up to 150 mg/day | Equally effective to indomethacin |
| Naproxen | Up to 1000 mg/day | Inferior to etoricoxib |
| Celecoxib | Up to 400 mg/day | COX-2, comparable to traditional NSAIDs |
| Etoricoxib | 90-120 mg/day | Superior to naproxen in trials |
| Meloxicam | Up to 22.5 mg/day | Comparable to piroxicam |
Continuous vs. on-demand NSAIDs: One study with celecoxib showed continuous use reduced spinal radiographic progression compared to on-demand use at 2 years. However, the ENRADAS trial with diclofenac found no benefit for continuous use. Current guidelines conditionally recommend continuous NSAIDs for active disease, on-demand when disease is stable.
NSAID limitations: Caution in patients with IBD (use with care - preferably a COX-2 inhibitor), cardiovascular disease, hypertension, or renal impairment.
Step 3: Glucocorticoids
Systemic glucocorticoids are NOT recommended for axial disease - RCTs have failed to show meaningful benefit.
Intra-articular glucocorticoid injections may be considered for:
- Isolated peripheral joint involvement
- Sacroiliac joint injection (conditional recommendation per ACR/SAA/SPARTAN for isolated sacroiliitis) - although benefit is temporary and additional imaging-guided radiation exposure is a concern
Local glucocorticoid injections to entheseal sites may provide temporary relief.
Step 4: Conventional Synthetic DMARDs (csDMARDs)
Traditional csDMARDs (methotrexate, sulfasalazine, leflunomide) have NO demonstrated benefit for axial disease and are not recommended for the axial manifestations of AS.
A limited role for sulfasalazine exists in patients with predominant peripheral arthritis, where it may modestly reduce peripheral joint symptoms.
Step 5: Biologic DMARDs (bDMARDs) - For NSAID Inadequate Responders
The threshold for escalation to biologics is active disease (BASDAI ≥4 or ASDAS ≥2.1) despite adequate NSAID trial of at least 2 NSAIDs over 4 weeks each.
TNF Inhibitors (TNFi) - First Biologic Choice
Five TNF inhibitors are approved for AS. All have demonstrated remarkable similarity in efficacy in Phase III trials, improving symptoms, CRP, MRI inflammation, health-related quality of life, anemia, and sleep quality:
| Drug | Target | Dose and Route |
|---|---|---|
| Infliximab | TNF (monoclonal Ab) | 5 mg/kg IV - weeks 0, 2, 6, then every 6 weeks |
| Etanercept | TNF receptor fusion | 50 mg SC once weekly |
| Adalimumab | TNF (monoclonal Ab) | 40 mg SC every 2 weeks |
| Golimumab | TNF (monoclonal Ab) | 50 mg SC once monthly |
| Certolizumab pegol | TNF (PEGylated Fab) | 400 mg SC at weeks 0, 2, 4; then 200 mg every 2 weeks |
Key considerations for TNFi choice:
- IBD comorbidity: Use a monoclonal antibody (infliximab, adalimumab, or certolizumab for Crohn's; infliximab, adalimumab, or golimumab for UC) - etanercept does NOT work for IBD
- Recurrent anterior uveitis: Prefer monoclonal antibodies (best evidence for adalimumab and infliximab)
- Pregnancy: Certolizumab pegol has minimal placental transfer and is the preferred TNFi in pregnancy
- Early and continuous treatment with anti-TNF agents has been shown to inhibit radiographic progression in longitudinal cohort studies
Tapering TNFi: Patients reaching remission (ASDAS <1.3) may consider dose tapering per ASAS-EULAR guidelines, but complete discontinuation leads to almost universal flare. ACR 2019 conditionally recommends against tapering.
IL-17A Inhibitors - Alternative First or Second Biologic
The IL-23/IL-17 axis is genetically implicated in AS, and IL-17A inhibitors are highly effective:
| Drug | Target | Dose and Route |
|---|---|---|
| Secukinumab | IL-17A | 150-300 mg SC - weekly for 5 weeks, then monthly |
| Ixekizumab | IL-17A | 160 mg SC at week 0, then 80 mg every 4 weeks |
IL-17A inhibitors are an alternative first-line biologic or second-line after TNFi failure. They may be preferred in patients with concomitant psoriasis. However, they may worsen IBD and should be avoided in patients with IBD.
Important note on IL-23 inhibitors: Drugs targeting IL-23 (ustekinumab, risankizumab, guselkumab) have consistently failed in AS trials despite genetic data implicating this pathway. This is thought to be because in AS, IL-17 is produced through an IL-23-independent pathway via innate-like lymphocytes.
Step 6: JAK Inhibitors (tsDMARDs) - For bDMARD Failures or Contraindications
Oral targeted synthetic DMARDs have now been approved for AS:
| Drug | Type | Key Trial Data |
|---|---|---|
| Tofacitinib | Pan-JAK inhibitor | Phase III: ASAS20 met by 56.4% vs 12.5% placebo; response as early as 2-4 weeks |
| Upadacitinib | Selective JAK-1 inhibitor | Phase II/III positive; now approved |
Safety considerations with JAK inhibitors: Monitor for herpes zoster (2.3% with tofacitinib), serious infections, hepatic events, thromboembolism, and cardiovascular events (class-wide warning). Not preferred in patients with cardiovascular risk factors.
Agents that have FAILED in AS trials (important to know):
- Rituximab (anti-CD20) - Phase II failure in TNFi inadequate responders
- Abatacept (CTLA4-Ig) - no efficacy
- Tocilizumab / sarilumab (IL-6 pathway) - no efficacy, no MRI improvement
- Ustekinumab (IL-12/23) - Phase III closed early for failure in biologic-naive AS
- Risankizumab (IL-23) - failed primary endpoint
Surgery
- Total hip arthroplasty for severe hip disease - often very successful in improving function
- Spinal osteotomy for severe kyphotic deformity causing inability to look forward - high-risk procedure requiring specialized centers
- Spinal fracture management - transverse fractures through fused segments are highly unstable and frequently catastrophic; treated surgically
Monitoring and Treat-to-Target
The TICOSPA pragmatic trial tested a treat-to-target approach (target: ASDAS <2.1 every 4 weeks) versus usual care. Although the primary endpoint difference was not achieved, the 2022 ASAS-EULAR guidelines recommend monitoring ASDAS and requiring at least a clinically important improvement (ΔASDAS ≥1.1) to continue a given therapy.
Disease monitoring tools:
- ASDAS - preferred composite measure (includes CRP)
- BASDAI - patient-reported, widely used clinically
- BASFI (Bath Ankylosing Spondylitis Functional Index) - measures functional limitation
- BASMI (Bath Ankylosing Spondylitis Metrology Index) - measures spinal mobility; lateral spinal flexion is the most sensitive single measure
- MRI - for monitoring inflammation; spine scored using SPARCC or Berlin scores
- Modified Stoke AS Spine Score (mSASSS) - radiographic progression in the spine
Prognosis
- Disease course is variable; some have mild intermittent symptoms, others have progressive disabling disease
- Predictors of worse radiographic outcome: elevated CRP, presence of syndesmophytes at baseline, male sex, smoking
- Life expectancy is moderately reduced due to cardiovascular disease, osteoporosis-related fractures, and amyloidosis
- Early biologic therapy reduces inflammation and may slow structural progression
- NSAIDs, physiotherapy, and patient education remain the foundation; biologics and JAK inhibitors have transformed outcomes for moderate-to-severe disease
Summary of Treatment Algorithm
Active AS (BASDAI ≥4 / ASDAS ≥2.1)
|
▼
1. NSAID (full dose) + Physiotherapy
- Trial 2 NSAIDs (4 weeks each)
|
Inadequate response
▼
2. Biologic DMARD:
- TNF inhibitor (first choice)
OR IL-17A inhibitor (especially if psoriasis; avoid if IBD)
|
Inadequate response / failure
▼
3. Switch to different TNFi OR switch class (IL-17A ↔ TNFi)
|
Still failing
▼
4. JAK inhibitor (tofacitinib, upadacitinib)
Special considerations:
- IBD present → TNFi monoclonal Ab preferred
- Recurrent uveitis → Adalimumab / infliximab preferred
- Peripheral arthritis → Sulfasalazine may add benefit
- Hip disease → Total hip arthroplasty
Sources:
- Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set - Chapters on axial SpA genetics, TNF inhibitors, JAK inhibitors, and management
- Rheumatology, 2-Volume Set (Elsevier, 2022) - Chapters 125 on AS management, NSAIDs table, bDMARD table, ASAS/EULAR management flowchart
- Grainger & Allison's Diagnostic Radiology - Chapter 44, AS imaging
- Washington Manual of Medical Therapeutics - Chapter 25, SpA clinical presentation and features
- 2024 update on biologic therapies for AS (Allergologia et Immunopathologia)
- 2025 British Society for Rheumatology guideline for axial SpA
This is a shared conversation. Sign in to Orris to start your own chat.