Tests to be sent in first time dvt
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive breakdown of investigations to be sent in a first-time (unprovoked or provoked) DVT:
Investigations for First-Time DVT
Step 1 — Assess Pretest Probability (Wells Score)
Before ordering tests, calculate the Wells DVT Score:
| Clinical Feature | Points |
|---|---|
| Active cancer | +1 |
| Paralysis/paresis/recent plaster cast | +1 |
| Bedrest >3 days or major surgery within 3 months | +1 |
| Localized tenderness along deep veins | +1 |
| Entire leg swollen | +1 |
| Calf swelling >3 cm vs. asymptomatic side | +1 |
| Pitting edema (symptomatic leg only) | +1 |
| Collateral superficial veins (non-varicose) | +1 |
| Previously documented DVT | +1 |
| Alternative diagnosis as likely or more likely | −2 |
Score ≤0 = low probability | 1–2 = moderate | ≥3 = high probability
Step 2 — Diagnostic Algorithm
A. Confirming DVT
| Test | Role |
|---|---|
| D-dimer | First-line for low/moderate pretest probability. A negative D-dimer effectively excludes DVT — no further testing needed. Elevated in cancer, infection, pregnancy, surgery, advanced age (low specificity). |
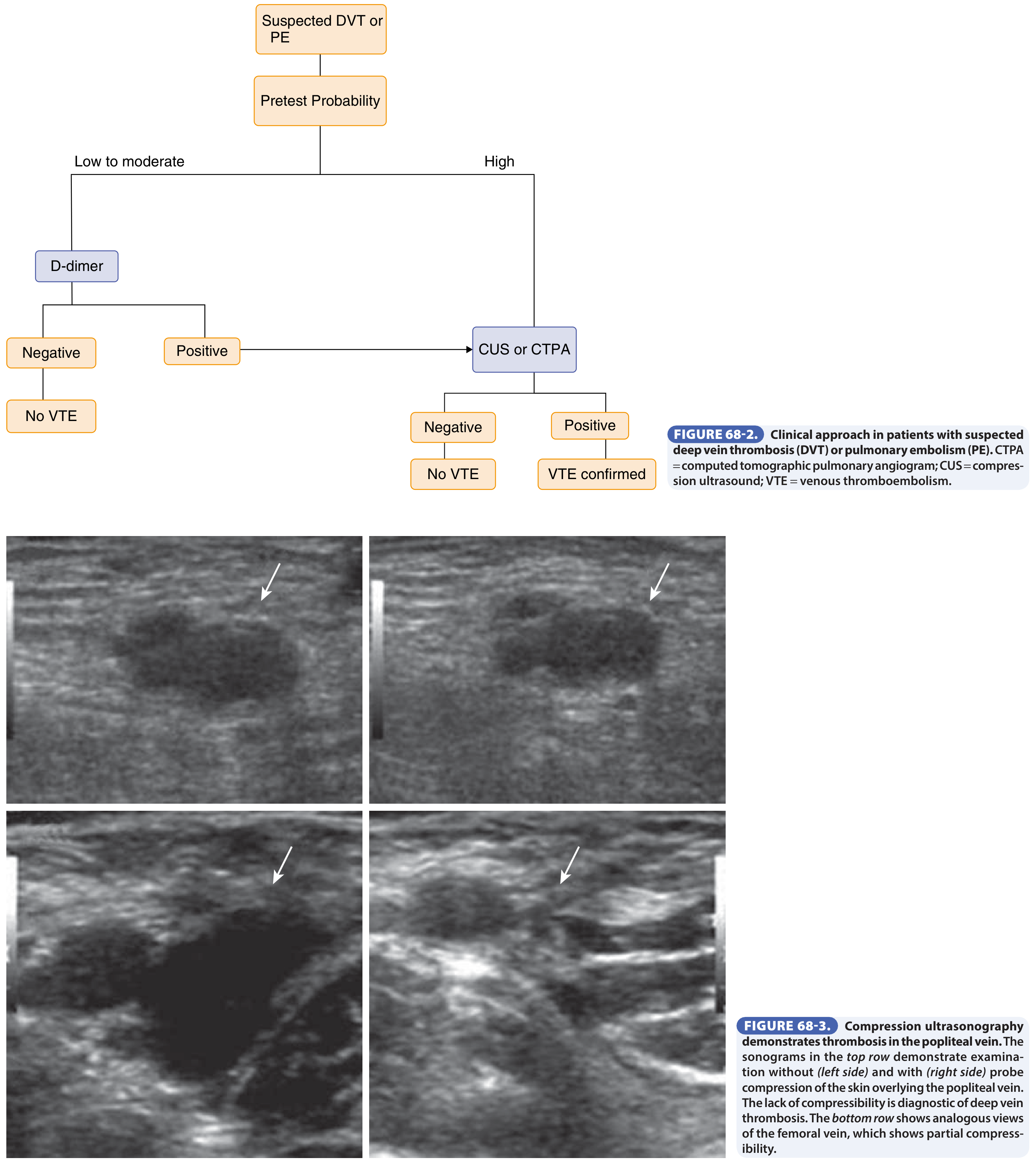
| Compression Ultrasonography (CUS) | Test of choice for all patients with high pretest probability or positive D-dimer. Non-compressibility of proximal leg veins is diagnostic. Sensitivity is lower for calf DVT — if only proximal veins examined, repeat in 1 week. |
| Contrast Venography | Gold standard — reserved for equivocal cases. Rarely done due to cost, discomfort, and risk of complications. |
| MRI venography | Useful for recurrent ipsilateral DVT or when ultrasound is inconclusive; avoids radiation. |
B. Baseline / Routine Blood Tests
These are sent in every first-time DVT:
- CBC (complete blood count) — exclude polycythemia, thrombocytosis, or malignancy
- LFTs, RFTs, electrolytes — baseline before anticoagulation
- PT/INR and aPTT — baseline coagulation; needed if starting warfarin
- Blood group and screen
- Urinalysis — occult blood/protein may suggest underlying renal pathology or malignancy
- Fecal occult blood test
- Chest X-ray — screen for malignancy; PE signs if suspected
C. Thrombophilia Screen (Hypercoagulable Workup)
For first unprovoked DVT, especially in young patients or with strong family history:
| Test | Target |
|---|---|
| Antithrombin III activity | Inherited antithrombin deficiency |
| Protein C activity | Protein C deficiency |
| Protein S antigen/activity | Protein S deficiency |
| Factor V Leiden (PCR or APC resistance assay) | Most common inherited thrombophilia |
| Prothrombin gene mutation (G20210A) | Second most common |
| Lupus anticoagulant | Antiphospholipid syndrome |
| Anticardiolipin antibodies (IgG & IgM) | Antiphospholipid syndrome |
| Anti-β2-glycoprotein I antibodies | Antiphospholipid syndrome |
| Homocysteine level | Hyperhomocysteinemia |
| JAK2 V617F mutation | Myeloproliferative neoplasm (especially portal/hepatic vein thrombosis) |
⚠️ Timing matters: Acute thrombosis and anticoagulation (especially heparin and warfarin) can falsely reduce antithrombin, protein C, and protein S levels. Ideally test after completing anticoagulation or use genetic tests (Factor V Leiden, prothrombin mutation) which are unaffected. The lupus anticoagulant can be affected by DOACs.
D. Malignancy Screen
Unprovoked DVT carries increased risk of occult malignancy. A limited workup is recommended:
- Thorough history and physical examination
- CBC, LFTs, calcium, LDH
- Urinalysis
- Fecal occult blood
- Chest X-ray
- PSA (in men)
- Mammogram (in women)
- CT chest/abdomen/pelvis only if initial screening reveals abnormalities
E. Imaging for PE (if clinically suspected)
- CT Pulmonary Angiography (CTPA) — standard of care; directly visualizes thrombus in pulmonary arteries
- V/Q scan — preferred in renal impairment, contrast allergy, pregnancy, or young women (<40 years)
Key principle: The diagnosis of DVT is not reliably made on clinical signs alone (fewer than 50% of DVT patients present with classic signs). A structured approach using Wells score → D-dimer → CUS is mandatory.
— Goldman-Cecil Medicine, Chapter 68; Chapter 157
So which Thrombophilia Screening test should be sent prior to anticoagulation
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
This is a very clinically important question. Here is the precise answer:
Thrombophilia Tests That Can Be Sent BEFORE Anticoagulation
The core problem is that most functional assays are unreliable once anticoagulation starts — and even the acute thrombotic event itself can consume plasma factors and cause false results.
Tests Unaffected by Anticoagulation — Send ANY Time (including before/during)
| Test | Why unaffected |
|---|---|
| Factor V Leiden mutation (PCR) | Genetic test — anticoagulants don't alter DNA |
| Prothrombin G20210A mutation (PCR) | Genetic test — same reason |
| JAK2 V617F mutation | Genetic test |
These genetic/molecular tests can be sent at any point — before, during, or after anticoagulation.
Tests Best Sent BEFORE Starting Anticoagulation (but tricky even then)
The window between presentation and starting anticoagulation is very narrow and imperfect:
| Test | Problem if anticoagulated |
|---|---|
| Antithrombin III (AT III) activity | Heparin decreases AT III levels → false deficiency |
| Protein C activity | Warfarin decreases protein C → false deficiency. DOACs may falsely increase levels in clot-based assays |
| Protein S activity/antigen | Warfarin decreases protein S. Heparin increases it. Acute thrombosis also consumes it |
| Lupus anticoagulant (LA) | Heparin may mask LA (unless heparinase neutralization used). DOACs cause false-positive LA |
| Anticardiolipin antibodies (IgG/IgM) | Relatively unaffected by anticoagulation — can be sent at any time |
| Anti-β2-glycoprotein I antibodies | Relatively unaffected — can be sent at any time |
⚠️ Even in the immediate pre-anticoagulation period, plasma factors (AT III, Protein C, Protein S) may be consumed by the acute thrombotic event itself, risking false positives. The ideal time is several months after the event, off anticoagulation.
Practical Summary: What to Send BEFORE Anticoagulation
Since anticoagulation is usually started urgently and cannot be delayed for thrombophilia workup, the pragmatic approach is:
| Send NOW (before anticoagulation) | Defer until off anticoagulation (3–6 months later) |
|---|---|
| Factor V Leiden (PCR) | Antithrombin III activity |
| Prothrombin G20210A (PCR) | Protein C activity |
| Anticardiolipin antibodies (IgG/IgM) | Protein S activity/antigen |
| Anti-β2-GP1 antibodies | Lupus anticoagulant |
| Homocysteine level | — |
| JAK2 V617F (if atypical site) | — |
Key Rule on Anticoagulant Interference
| Drug | Falsely lowers | Falsely elevates / masks |
|---|---|---|
| Heparin | Antithrombin III | Protein S; masks Lupus anticoagulant |
| Warfarin | Protein C, Protein S | — |
| DOACs (rivaroxaban, apixaban, dabigatran) | — | Protein C, Protein S, AT III (clot-based assays); false-positive Lupus anticoagulant |
Bottom line: Do not delay anticoagulation for thrombophilia testing. Send the genetic tests (Factor V Leiden, Prothrombin G20210A) and antiphospholipid antibodies before starting — these are either unaffected by anticoagulants or relatively robust. Defer the functional assays (Protein C, S, Antithrombin) until the patient has been off anticoagulation for at least 2–4 weeks (warfarin) or 48–72 hours (DOACs).
— Henry's Clinical Diagnosis and Management by Laboratory Methods, Chapter on Thrombophilia
Factor V Leiden (PCR) Antithrombin III activity Prothrombin G20210A (PCR) Protein C activity Anticardiolipin antibodies (IgG/IgM) Protein S activity/antigen Anti-β2-GP1 antibodies Lupus anticoagulant Homocysteine level — JAK2 V617F (if atypical site)- are all these from blue tube
Checking Date & Time
Finding Sources
Finding Sources
Reading File
Finding Sources
No, they are not all from the blue tube. Here is the breakdown:
Collection Tubes for Thrombophilia Tests
| Test | Tube | Colour |
|---|---|---|
| Antithrombin III activity | Sodium citrate (3.2%) | 🔵 Light Blue |
| Protein C activity | Sodium citrate (3.2%) | 🔵 Light Blue |
| Protein S activity/antigen | Sodium citrate (3.2%) | 🔵 Light Blue |
| Lupus anticoagulant | Sodium citrate (3.2%) — platelet-poor plasma required | 🔵 Light Blue |
| Factor V Leiden mutation (PCR) | EDTA | 🟣 Lavender/Purple |
| Prothrombin G20210A mutation (PCR) | EDTA | 🟣 Lavender/Purple |
| JAK2 V617F mutation (PCR) | EDTA | 🟣 Lavender/Purple |
| Anticardiolipin antibodies (IgG/IgM) | Plain/clot activator — serum | 🔴 Red / Gold SST |
| Anti-β2-GP1 antibodies | Plain/clot activator — serum | 🔴 Red / Gold SST |
| Homocysteine level | EDTA (lavender) or fluoride-oxalate | 🟣 Lavender (some labs use green) |
The Logic Behind the Tubes
-
Blue top (sodium citrate) — for functional coagulation assays. Citrate chelates calcium and preserves labile coagulation factors. Requires correct 9:1 blood-to-anticoagulant ratio and processing into platelet-poor plasma. Used for AT III, Protein C, Protein S, Lupus anticoagulant.
-
Lavender/purple top (EDTA) — for molecular/genetic (PCR) tests and haematology. DNA is stable in EDTA. Factor V Leiden, Prothrombin G20210A, JAK2 V617F are all PCR-based and go in lavender.
-
Red/gold top (plain serum) — for immunological/antibody assays (ELISA-based). Anticardiolipin and anti-β2-GP1 antibodies are measured in serum, not plasma.
Practical Note
When collecting for a lupus anticoagulant specifically, the blue tube must be fully filled (underfilling causes excess citrate and falsely prolongs clotting times) and the sample must be processed to double-spun platelet-poor plasma — platelets can neutralise phospholipid-dependent antibodies and give a false-negative result.
— Henry's Clinical Diagnosis and Management by Laboratory Methods; Tietz Textbook of Laboratory Medicine, 7th Edition
This is a shared conversation. Sign in to Orris to start your own chat.