Mri in orthopedics
Reading File
Finding Sources
Finding Sources
Searching the Web
MRI in orthopedics clinical applications indications 2024
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative orthopedic and rheumatology textbooks, along with actual MRI images. Let me compile the full answer.
MRI in Orthopedics
MRI is the most valuable soft-tissue imaging tool in orthopedics. Unlike plain radiographs and CT (which excel at cortical bone), MRI uniquely visualizes bone marrow, articular cartilage, ligaments, tendons, menisci, synovium, nerves, and muscles - all without ionizing radiation.
1. Basic Principles Relevant to Orthopedics
MRI signal depends on the sequence used:
| Sequence | Key Use | Appearance |
|---|---|---|
| T1-weighted | Anatomic orientation, tissue characterization, fat | Fat = bright; Water/edema = dark |
| T2-weighted | Fluid, edema, joint effusion | Water = bright; cortical bone = dark |
| PDFS (Proton Density Fat Saturation) | Cartilage evaluation, subtle edema | Hyaline cartilage = high signal; fat suppressed |
| STIR (Short Tau Inversion Recovery) | Bone marrow edema, stress reactions | Edema = bright; fat suppressed |
| Gadolinium contrast (T1+Gd) | Infection, tumors, synovitis | Enhances vascular/inflamed tissue |
| DWI (Diffusion Weighted Imaging) | Differentiating abscess vs. reactive marrow | Restricted diffusion = bright |
"T1-weighted images are primarily suited for anatomic orientation and tissue characterization, while PDFS sequences play an important role in the diagnosis of joint damage because they are very sensitive to edematous changes and allow for the high signal intensity of hyaline articular cartilage." - THIEME Atlas of Musculoskeletal System
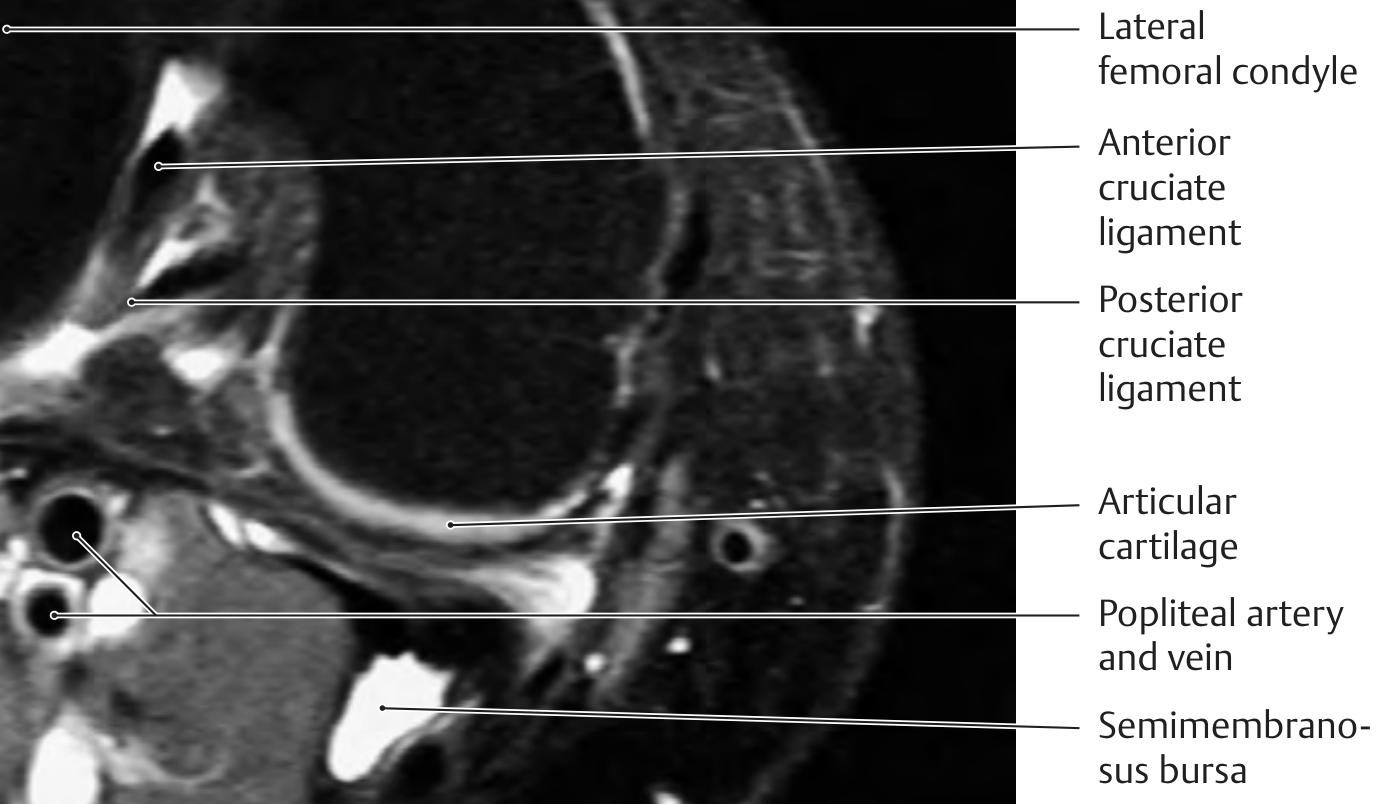
2. MRI of the Knee
The knee is the most commonly imaged joint in orthopedics. MRI gives detailed views of:
Cruciate Ligaments
- Sagittal plane is preferred for viewing both cruciate ligaments in continuity
- The PCL is clearly visible in its entirety in sagittal sections; the ACL requires 15-20° external rotation of the knee for complete visualization
- ACL tear: loss of normal linear fibers, replaced by diffuse high T2 signal or discontinuity
- 1.5T MRI has high accuracy for ACL and meniscal tear diagnosis
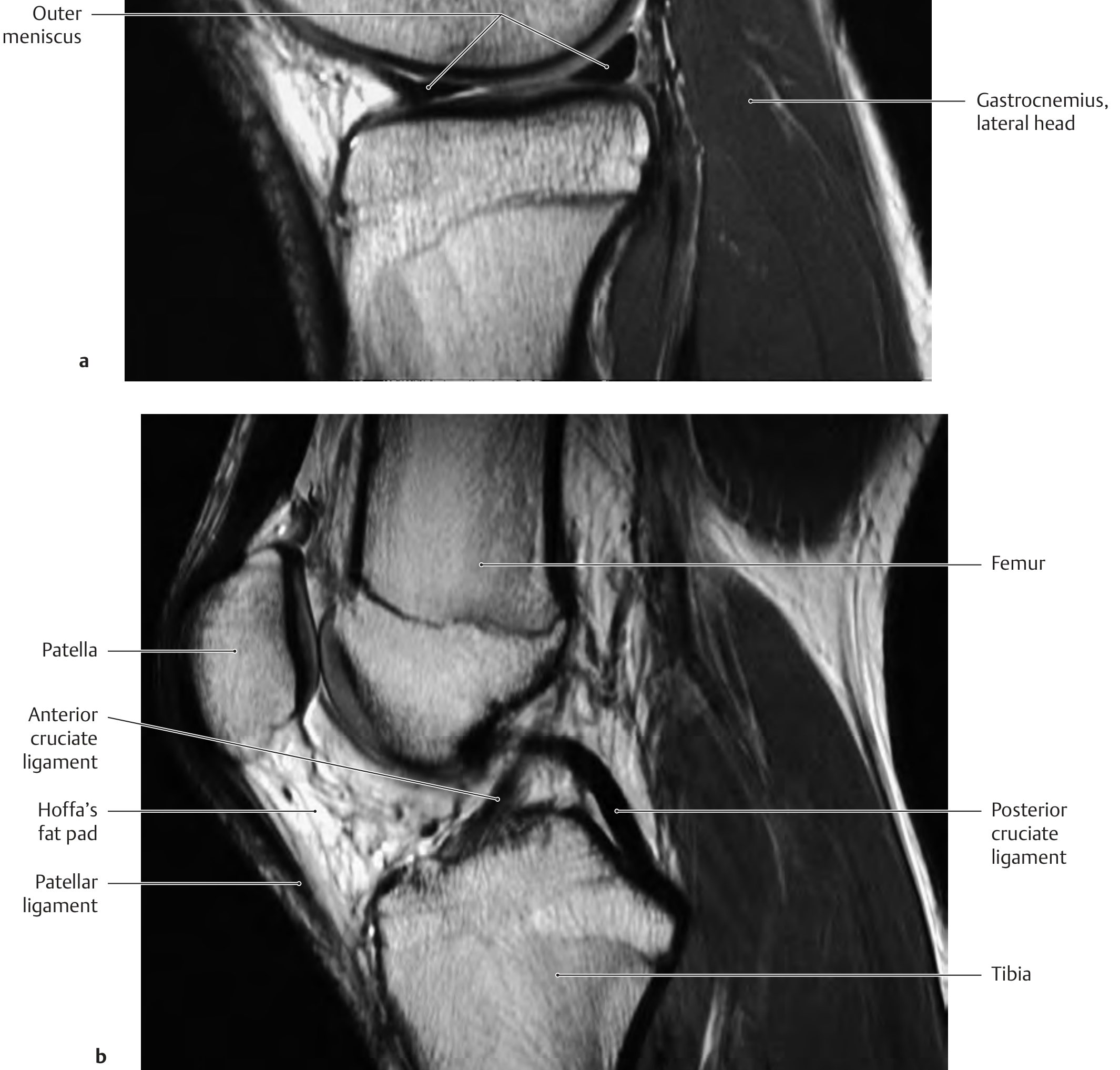
Menisci
- Meniscal tears: best seen on sagittal and coronal sequences
- Normal meniscus = low signal on all sequences (fibrocartilage)
- A tear = linear high signal extending to the articular surface
- Bucket-handle tears are a surgical emergency in young patients who cannot fully extend the knee
Articular Cartilage
- PDFS sequences best resolve cartilage thickness and focal defects
- Grading of chondral lesions (OCD, early OA)

3. MRI of the Spine
Spinal Infection (Spondylodiscitis / Spinal Epidural Abscess)
MRI is the imaging modality of choice with 96% sensitivity and 93% specificity for spinal infection.
Key points from Campbell's Operative Orthopaedics 15th Ed 2026:
- Entire spine must be imaged because noncontiguous infection occurs in 15-20% of cases
- T1 sequences: decreased signal in infected vertebral bodies and disc spaces; disc-vertebral body margin cannot be differentiated
- T2 sequences: increased signal in the intervertebral disc, markedly increased in the vertebral body; paravertebral abscesses and thecal sac compression shown as areas of increased signal
- Fat suppression + post-gadolinium sequences improve sensitivity of T2 and T1 respectively
- DWI helps characterize fluid collections and differentiate spondylodiscitis from benign reactive marrow changes
- Gadolinium enhances delineation of epidural abscesses and determines their level/position relative to neural elements
- Serial MRI is NOT indicated to follow treatment response unless patient is clinically failing - bony findings often worsen or remain unchanged despite clinical improvement; monitor soft-tissue findings (paraspinal abscesses, epidural collections, T2 disc changes) instead
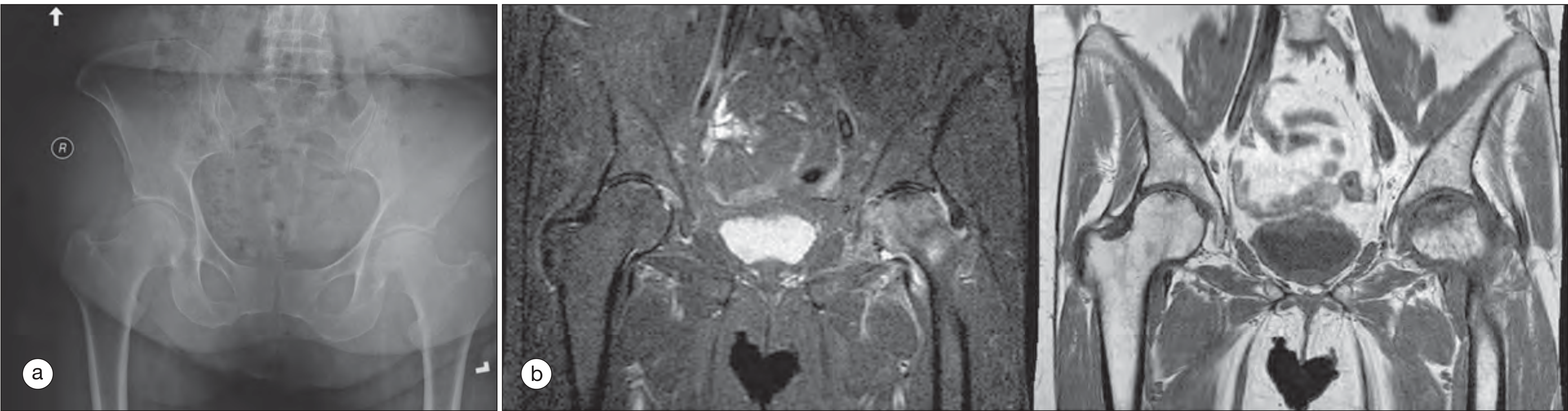
4. MRI of the Hip - Avascular Necrosis (AVN / Osteonecrosis)
MRI is the gold standard for early diagnosis of AVN, far more sensitive than plain X-rays.
From Rheumatology 2022, Elsevier:
- Negative radiographic findings with clinical suspicion should always prompt MRI
- T1-weighted coronal: geographic lesion of low signal in the weight-bearing surface of the femoral head - "double line sign" is pathognomonic
- STIR (coronal): confirms the geographic lesion with high signal intensity corresponding to marrow edema
- ACR recommends bilateral hip MRI to detect contralateral early osteonecrosis before collapse
- Radionuclide bone scan is the second-line substitute when MRI is contraindicated
5. MRI of the Ankle and Foot
From Campbell's Operative Orthopaedics 15th Ed 2026:
- Axial MRI with local gradient: best for anterior talofibular ligament (ATFL), posterior talofibular ligament (PTFL), deep layers/tibionavicular component of deltoid ligament
- Coronal MRI: best for calcaneofibular ligament (CFL), posterior talofibular ligament, tibiocalcaneal and posterior tibiotalar ligaments; also differentiates deep vs. superficial layers of the medial collateral ligament
- MRI is more specific than sensitive for CFL injuries
- Bone bruises occur in a significant number of ankle sprains; multiple bone bruises suggest multi-ligament injury; can persist >1 year after injury
- 3T MRI with AI-based reconstruction can produce high-quality ligament/tendon images in <10 minutes - improving accuracy and efficiency
6. MRI in Rheumatoid Arthritis (RA)
From Rheumatology 2022, Elsevier:
- MRI uniquely images bone, articular structures, and soft tissues without ionizing radiation
- Initially used for large joints (hips, knees, shoulders); improved technology now resolves smaller joints
- 3.0T MRI provides quantitative measurement of bone marrow edema; combined with CT gives comprehensive analysis of joint inflammation and bone damage
- Coupling of serologic tests with symmetric synovitis + bone edema or bone erosion on MRI helps discriminate RA from undifferentiated arthritis and spondyloarthritis
- Extremity MRI (E-MRI): smaller units for peripheral joints; lower cost, better positioning; growing role in clinical rheumatology
7. MRI Advantages Over Other Modalities in Orthopedics
| Feature | X-ray | CT | MRI |
|---|---|---|---|
| Cortical bone | ++ | +++ | + |
| Bone marrow / medullary | + | ++ | +++ |
| Articular cartilage | - | + | +++ |
| Ligaments/tendons | - | - | +++ |
| Menisci | - | + | +++ |
| Soft tissue infection/abscess | - | ++ | +++ |
| Spinal cord/nerve roots | - | + | +++ |
| Ionizing radiation | Yes | Yes | No |
8. Contraindications and Practical Points
- Absolute contraindications: ferromagnetic implants (older pacemakers, cochlear implants, certain intracranial aneurysm clips), intraocular metallic foreign bodies
- Passive orthopedic implants (prosthetic joints, plates, screws) are generally MRI-safe but require manufacturer confirmation; newer scanners with MARS (Metal Artifact Reduction Sequences) significantly reduce streak artifact from hardware
- Claustrophobia: managed with open scanners or anxiolytics
- Gadolinium contrast is avoided in severe renal impairment (risk of nephrogenic systemic fibrosis)
- Not indicated routinely for initial evaluation of low back pain (no red flags) - clinical history + exam + plain films are sufficient first steps per AAFP guidelines
Summary of Key Orthopedic Indications for MRI
| Indication | Why MRI |
|---|---|
| ACL/PCL tear | Best ligament visualization, confirms diagnosis pre-op |
| Meniscal tear | Detects tears, bucket-handle patterns, repair vs. resection decision |
| AVN of hip (early) | Most sensitive; detects before X-ray changes |
| Spinal infection | 96% sensitivity; detects abscesses, guides surgical approach |
| Bone tumors | Characterizes marrow involvement, soft-tissue extension |
| Stress fracture | STIR shows marrow edema before X-ray changes |
| Rotator cuff tear | Full-thickness vs. partial; repair feasibility |
| Ankle ligament injury | Ligament integrity, bone bruises, peroneal pathology |
| Osteochondral lesions | Cartilage thickness, subchondral bone, staging |
| Septic arthritis | Synovial thickening, effusion, bone involvement |
Sources:
- Campbell's Operative Orthopaedics 15th Ed 2026 (Spinal MRI sections)
- THIEME Atlas of General Anatomy and Musculoskeletal System (Knee MRI)
- Rheumatology 2-Volume Set, Elsevier 2022 (RA imaging, AVN of hip)
- Bailey & Love's Short Practice of Surgery 28th Ed (ACL injury)
This is a shared conversation. Sign in to Orris to start your own chat.