Q1 a) WHO ladder for cancer pain management. 5marks (b) gate control theory of pain 5mark (c) pain pathway Q2 a) Enumerate the causes of acute hepatic failure. [3] b) What are the principles of management of acute hepa�c failure in the ICU? [7]. Answer these question from standard text for dnb anesthesia exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed to write comprehensive DNB-standard answers. Let me compose the full response.
DNB Anaesthesia Exam Answers
QUESTION 1
Q1(a) WHO Analgesic Ladder for Cancer Pain Management (5 marks)
The WHO analgesic ladder was introduced in 1986 as a three-step framework for cancer pain management. The underlying principle is to match analgesic potency to the severity of pain, using oral medications in the simplest, most cost-effective manner, titrating regularly around the clock ("by the clock") rather than on demand, and advancing a step only when pain persists or increases at the current step.
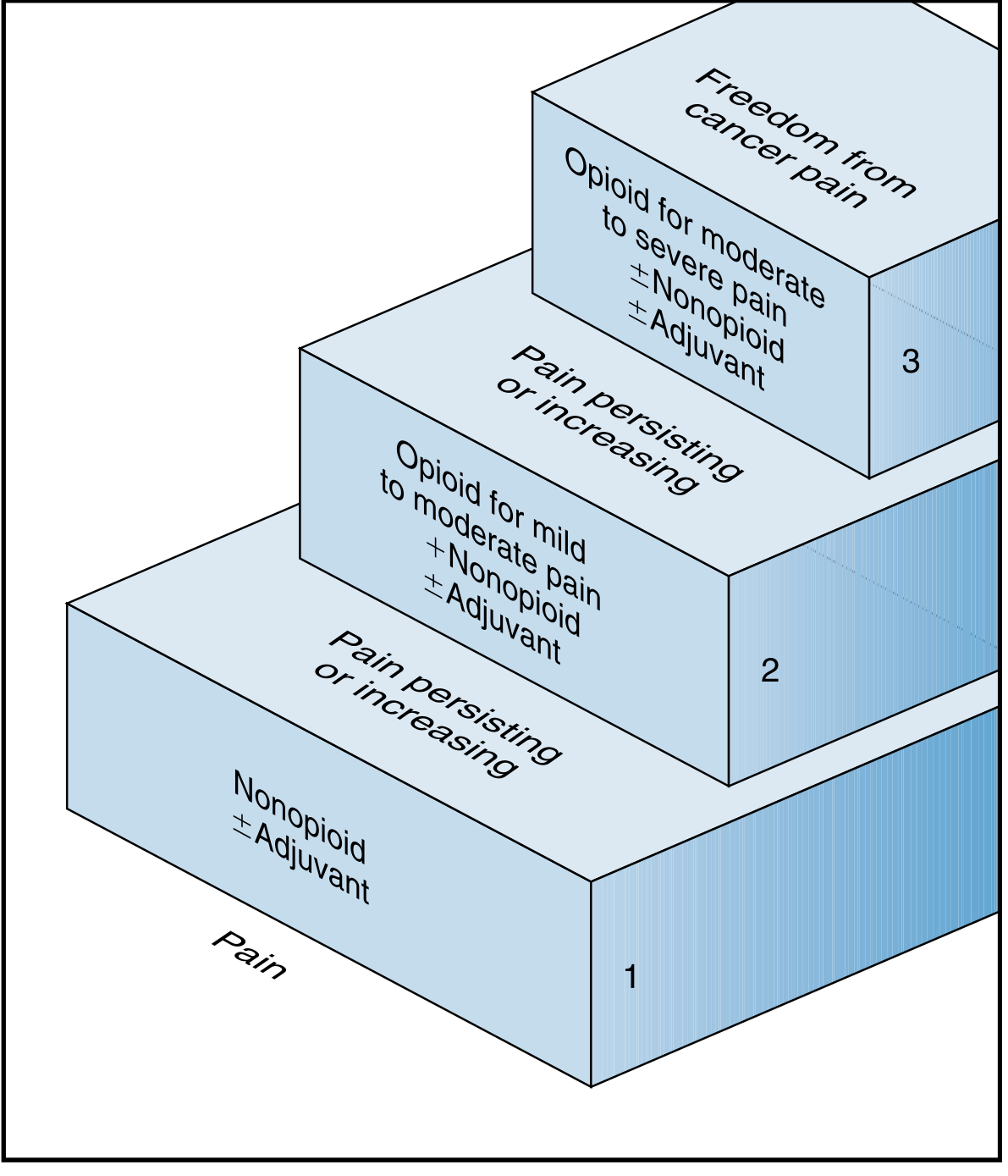
Step 1 - Mild Pain (NRS 1-3): Non-Opioid + Adjuvant
- Paracetamol (acetaminophen), aspirin, or NSAIDs (e.g., ibuprofen, diclofenac)
- +/- Adjuvant drugs (e.g., tricyclic antidepressants, anticonvulsants, corticosteroids, bisphosphonates)
- Covers approximately 20-25% of cancer patients adequately
Step 2 - Mild to Moderate Pain (NRS 4-6): Weak Opioid + Non-Opioid + Adjuvant
- Codeine, tramadol, dihydrocodeine
- Continue non-opioid (add to, do not replace)
- +/- Adjuvant
- Used when Step 1 fails to control pain
Step 3 - Moderate to Severe Pain (NRS 7-10): Strong Opioid + Non-Opioid + Adjuvant
- Morphine (drug of first choice), oxycodone, hydromorphone, fentanyl, methadone, buprenorphine
- Oral morphine is the gold standard - initially short-acting every 4 hours, then converted to sustained-release (MST) twice daily once a stable dose is established
- Short-acting opioids kept as "rescue doses" for breakthrough pain
- Note: pethidine is no longer recommended due to accumulation of its toxic metabolite norpethidine
Key Principles of the WHO Ladder:
- By mouth - oral route preferred
- By the clock - regular dosing, not PRN
- By the ladder - step-wise progression
- For the individual - individual dose titration
- With attention to detail - adjuvants used at every step for neuropathic, bone, or visceral pain
Adjuvant Analgesics used at any step include:
- Neuropathic pain: anticonvulsants (gabapentin, carbamazepine), tricyclics (amitriptyline, desipramine)
- Bone pain: NSAIDs, bisphosphonates, corticosteroids
- Visceral/inflammatory: corticosteroids
When Step 3 Fails (Step 4 - interventional):
- Epidural or intrathecal opioid infusion, nerve blocks
- Neurolytic procedures (coeliac plexus block for pancreatic/upper GI cancer, intrathecal phenol, cordotomy)
- Spinal cord stimulation
(Sources: Bailey and Love's Short Practice of Surgery, 28th Ed; Bradley and Daroff's Neurology in Clinical Practice; Swanson's Family Medicine Review)
Q1(b) Gate Control Theory of Pain (5 marks)
Historical Context:
The Gate Control Theory was proposed by Ronald Melzack and Patrick Wall in 1965 (Science, 150:971) while they were working at MIT. It was a landmark revision of the older specificity and pattern theories of pain, introducing the concept that pain transmission is not a simple one-way system but is actively modulated at the spinal level.
Core Concept:
Pain perception is not solely determined by peripheral nociceptive input; it is gated (modulated) by a balance of activity between large-diameter (Aβ) non-nociceptive fibers and small-diameter (Aδ and C) nociceptive fibers converging on projection neurons in the dorsal horn of the spinal cord.
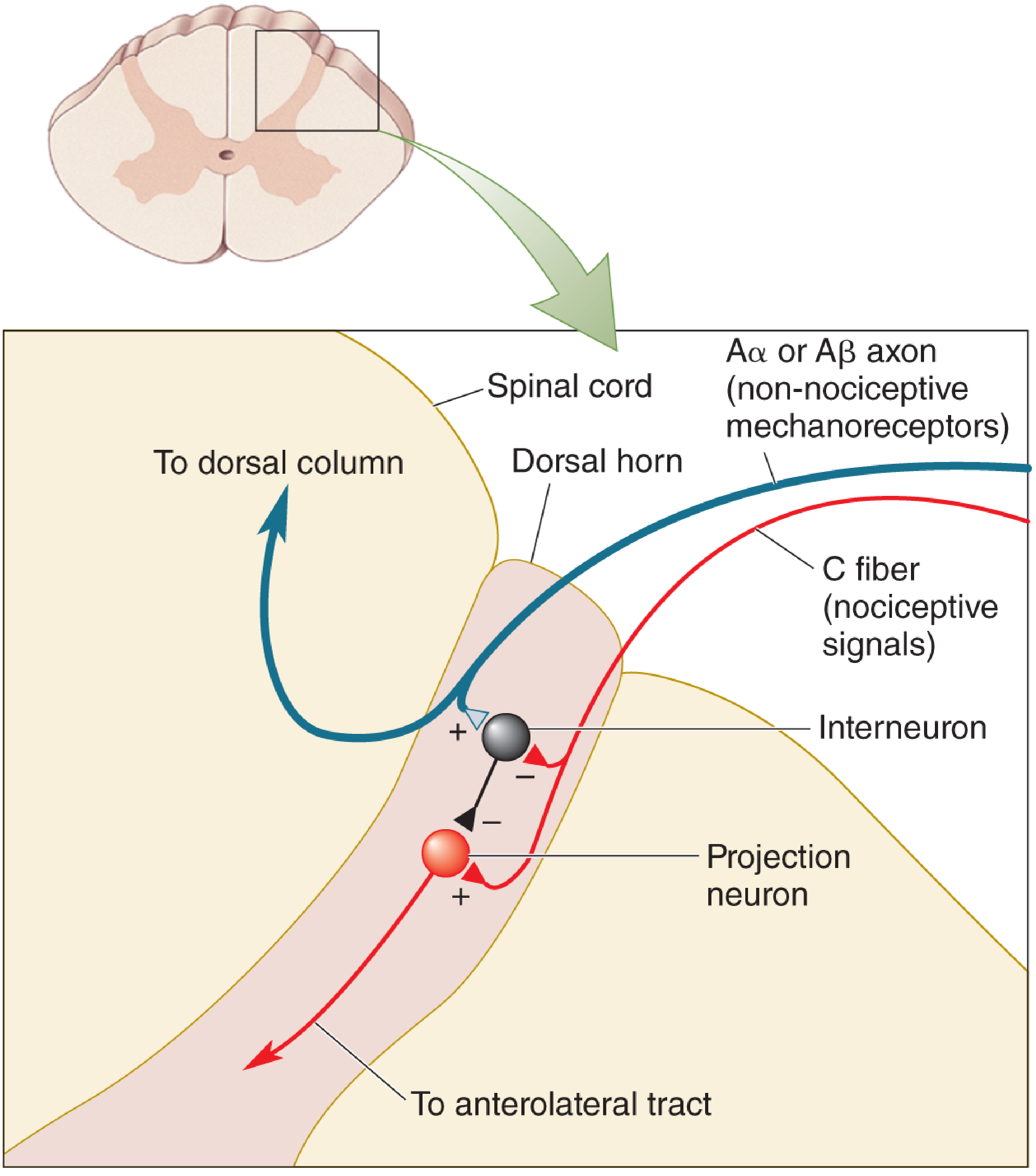
Neural Circuit:
| Component | Role |
|---|---|
| Aβ fibers (large-diameter, myelinated) | Touch, pressure, vibration - non-nociceptive |
| Aδ / C fibers (small-diameter, thinly/unmyelinated) | Pain and temperature - nociceptive |
| Inhibitory interneuron (substantia gelatinosa, lamina II) | The "gate" controller |
| Projection neuron (transmission cell, lamina I and V) | Sends signal up spinothalamic tract to brain |
Mechanism of Gating:
-
Gate OPEN (pain perceived): C fiber nociceptive input inhibits the inhibitory interneuron (disinhibition), which allows the projection neuron to fire, transmitting pain signals up the anterolateral tract to the brain.
-
Gate CLOSED (pain reduced): Aβ fiber activity (e.g., from rubbing, TENS) excites the inhibitory interneuron, which then inhibits the projection neuron, reducing the transmission of nociceptive signals - "closing the gate."
Practical Applications of Gate Control Theory:
- TENS (Transcutaneous Electrical Nerve Stimulation): Activates large Aβ fibers to close the gate - explains why TENS relieves chronic pain (arthritis, tendonitis)
- Spinal cord stimulation (SCS/dorsal column stimulation): Activates large dorsal column fibers
- Rubbing an injury: Activates mechanoreceptors (Aβ) to inhibit pain
- Acupuncture: Possible gate-closing via large fiber activation
Descending Modulation (extension of the theory):
Melzack and Wall's theory was later expanded to include descending inhibitory control. The periaqueductal gray (PAG) in the midbrain, when activated (by stress, emotion, or stimulation), sends descending projections via the raphe-spinal pathway (serotonin) and locus coeruleus (noradrenaline) to inhibit dorsal horn neurons, providing supraspinal "gating." This explains stress-induced analgesia and is the basis for epidural/intrathecal opioids and alpha-2 agonists.
(Sources: Neuroscience: Exploring the Brain, 5th Ed; Eric Kandel - Principles of Neural Science, 6th Ed; Adams and Victor's Principles of Neurology, 12th Ed)
Q1(c) Pain Pathway (5 marks)
The pain pathway involves three orders of neurons from the periphery to the cortex.
1. First-Order Neurons (Peripheral/Primary Afferents)
Nociceptors are free nerve endings in skin, muscle, joints, and viscera. They are activated by noxious stimuli (thermal, mechanical, chemical).
Fiber types:
- Aδ fibers (thinly myelinated, 2-5 m/s): Respond to sharp, well-localized "first pain"; thermal and mechanical nociceptors
- C fibers (unmyelinated, 0.5-2 m/s): Dull, burning, diffuse "second pain"; polymodal nociceptors
Peripheral sensitization: Tissue injury releases inflammatory mediators - bradykinin, prostaglandins, histamine, substance P, CGRP, ATP. These lower the threshold of nociceptors (hyperalgesia) and activate silent nociceptors (allodynia). Prostaglandins (via COX enzymes) sensitize nociceptors - the basis for NSAIDs.
Entry into spinal cord: Primary afferents enter via the dorsal root ganglion (cell body) and synapse in the dorsal horn at Rexed's laminae:
- Aδ fibers: synapse in laminae I and V
- C fibers: synapse in laminae I and II (substantia gelatinosa)
- Neurotransmitters released: glutamate (fast), substance P and CGRP (slow, sustained)
2. Second-Order Neurons (Spinal Cord to Thalamus - Four Ascending Tracts)
a) Spinothalamic Tract (most prominent):
- Axons of nociceptive-specific and wide-dynamic-range (WDR) neurons from laminae I, V, VI
- Cross the midline at the anterior commissure near the level of entry
- Ascend in the anterolateral white matter
- Terminate in the ventroposterolateral (VPL) thalamus
- Carry information about location, quality, intensity of pain (sensory-discriminative component)
- Basis of anterolateral cordotomy for intractable cancer pain (pain relief contralateral to the lesion)
b) Spinoreticular Tract:
- Axons from laminae VII and VIII
- Ascends in anterolateral column to reticular formation and thalamus
- Large, bilateral receptive fields - responsible for diffuse, poorly localized pain
- Mediates autonomic and arousal responses to pain
c) Spinoparabrachial Tract:
- Axons from laminae I and V
- Projects to parabrachial nucleus of the dorsolateral pons
- Parabrachial neurons project to the amygdala and anterior cingulate cortex
- Mediates the affective/emotional ("suffering") component of pain
- Collaterals to periaqueductal gray (PAG) - descending modulation
d) Spinohypothalamic Tract:
- Axons from laminae I, V, VII, VIII
- Projects to hypothalamic autonomic control centers
- Mediates neuroendocrine and cardiovascular responses accompanying pain (e.g., tachycardia, hypertension)
Central sensitization: Repeated C fiber input causes wind-up via NMDA receptor activation, calcium influx, and upregulation of c-fos. This leads to allodynia and hyperalgesia characteristic of neuropathic pain.
3. Third-Order Neurons (Thalamus to Cortex)
Lateral thalamic group (VPL, VPM, posterior/pulvinar):
- Receives spinothalamic tract input
- Projects to somatosensory cortex (S1, S2)
- Encodes location, quality, intensity of pain (small receptive fields)
- Lesion causes Dejerine-Roussy (thalamic pain) syndrome
Medial thalamic group (medial dorsal, intralaminar complex):
- Receives paleospinothalamic input
- Projects to anterior cingulate cortex, insular cortex, prefrontal cortex
- Encodes affective/motivational dimensions (the "unpleasantness" of pain)
Cortical processing:
- S1 cortex: sensory-discriminative aspect (where does it hurt, how bad?)
- Anterior cingulate cortex: emotional/affective suffering
- Insular cortex: interoceptive and autonomic integration
- Prefrontal cortex: cognitive evaluation, anticipation
Descending Modulation
- PAG (periaqueductal gray) activates raphe nucleus (serotonin) and locus coeruleus (noradrenaline)
- These descend via the dorsolateral funiculus to the dorsal horn
- Inhibit transmission neurons (the basis of opioid, alpha-2 agonist, and SSRI analgesia)
- Endogenous opioids (enkephalins, beta-endorphin) act at mu, kappa, delta receptors in the dorsal horn
(Sources: Eric Kandel - Principles of Neural Science, 6th Ed; Neuroscience: Exploring the Brain, 5th Ed)
QUESTION 2
Q2(a) Causes of Acute Hepatic Failure (3 marks)
Acute liver failure (ALF) is defined by the development of coagulopathy (INR >1.5) and hepatic encephalopathy in a patient without pre-existing liver disease, within 26 weeks of the onset of illness.
Classification by onset:
- Hyperacute (0-7 days from jaundice to encephalopathy): e.g., acetaminophen, HAV - high risk of cerebral edema but better chance of spontaneous recovery
- Acute (8-28 days): e.g., HBV
- Subacute (4-24 weeks): e.g., drug reactions, seronegative hepatitis - lower risk of cerebral edema but poor prognosis
Causes (enumerated):
A. Drugs and Toxins (most common in developed countries):
- Acetaminophen (paracetamol) overdose - No. 1 cause in UK (54%) and USA (46%); dose-dependent hepatotoxin; antidote is N-acetylcysteine within 16 hours
- Idiosyncratic drug reactions (non-dose-dependent DILI):
- Antitubercular drugs (isoniazid, rifampicin, pyrazinamide) - most common DILI in India
- Antiepileptics (phenytoin, valproic acid)
- Antibiotics (amoxicillin-clavulanate, tetracyclines)
- Antineoplastic agents
- Antiretroviral drugs (NRTIs - mitochondrial toxicity)
- NSAIDs
- MDMA (ecstasy), halothane (now rare)
- Herbal/complementary medicines (e.g., kava, germander, pyrrolizidine alkaloids)
- Mushroom poisoning: Amanita phalloides (death cap) - amatoxin
B. Viral Hepatitis:
5. Hepatitis B virus (HBV) - including acute HBV, reactivation, and delta co-infection
6. Hepatitis A virus (HAV) - rare but possible, especially in elderly
7. Hepatitis E virus (HEV) - major cause in India and South Asia (38% of cases); especially severe in pregnancy
8. Herpes simplex virus (HSV) - important in immunocompromised and pregnancy
9. Cytomegalovirus (CMV), Epstein-Barr virus (EBV), varicella-zoster virus
C. Vascular:
10. Budd-Chiari syndrome (acute hepatic vein thrombosis)
11. Ischemic hepatitis ("shock liver") - from cardiogenic shock, sepsis, heat stroke, right heart failure, severe hypotension
12. Hepatic artery thrombosis (post-transplant)
13. Sinusoidal obstruction syndrome (veno-occlusive disease)
D. Metabolic:
14. Wilson disease (acute presentation - high ceruloplasmin, Kayser-Fleischer rings, Coombs-negative hemolysis)
15. Acute fatty liver of pregnancy (AFLP)
16. HELLP syndrome (Hemolysis, Elevated Liver Enzymes, Low Platelets)
17. Reye's syndrome (children - aspirin + viral illness)
E. Autoimmune:
18. Autoimmune hepatitis (AIH) - acute severe presentation
F. Malignant infiltration:
19. Metastatic carcinoma (breast, lymphoma, melanoma) - massive hepatic infiltration
20. Primary hepatic malignancy (rare)
G. Indeterminate/Seronegative:
21. Up to 14-32% of ALF cases have no identifiable cause (seronegative hepatitis); middle-aged women, subacute presentation
(Source: Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Schwartz's Principles of Surgery, 11th Ed)
Q2(b) Principles of Management of Acute Hepatic Failure in the ICU (7 marks)
ALF is a multi-system catastrophe requiring admission to a liver transplant-capable ICU. Management is supportive while the liver either regenerates spontaneously or a donor organ is secured. Every system is affected.
1. General ICU Setup and Monitoring
- Transfer to a liver transplant center early
- Continuous monitoring: arterial line (IBP), CVP, hourly urine output, pulse oximetry, ECG
- Serial monitoring: INR/PT, LFTs, creatinine, electrolytes, glucose, arterial pH, lactate, blood cultures, ammonia levels
- Grade encephalopathy (Grade 1-4) at regular intervals
- Early intubation for Grade 3-4 encephalopathy (GCS <8) to protect the airway and allow ICP management
2. Neurological Complications - Cerebral Edema and Raised ICP
This is the leading cause of death in ALF (30-40% of patients, especially hyperacute). Cerebral edema results from cytotoxic and vasogenic mechanisms, driven by hyperammonemia and inflammatory cytokines.
Management:
- Head positioning: 30 degrees elevation
- Avoid triggers: Hyperthermia, hyponatremia, seizures, agitation
- ICP monitoring: Intracranial pressure (ICP) bolt/monitor for Grade 3-4 encephalopathy; target CPP >50 mmHg, ICP <20-25 mmHg
- Mannitol: 0.5-1 g/kg IV bolus for acute rises in ICP (serum osmolality must be <320 mOsm/L)
- Hypertonic saline (3%): Induce hypernatremia (Na 145-155 mmol/L) to reduce cerebral edema
- Hypothermia (mild, 33-35°C): Reduces cerebral blood flow, ammonia, and cerebral metabolic rate - used as a bridge to transplant in refractory cerebral edema
- Hyperventilation (short-term): For acute ICP crises (target PaCO2 4-4.5 kPa)
- Ammonia reduction: Rifaximin, lactulose (limited evidence in ALF), avoidance of protein catabolism, CRRT (continuous renal replacement therapy) clears ammonia effectively
3. Cardiovascular Support
- ALF produces a high-output, low-resistance state similar to sepsis (systemic vasodilatation)
- Fluid resuscitation: Crystalloids preferred; aggressive resuscitation for hypotension
- Vasopressors: Noradrenaline (norepinephrine) is first line for refractory hypotension
- Vasopressin/terlipressin: May be added for refractory vasodilation
- Monitor for and treat precipitating sepsis
4. Renal Support
- Acute kidney injury (AKI) occurs in 55% of ALF patients (especially acetaminophen)
- CRRT (continuous venovenous hemofiltration/hemodialysis): Preferred over intermittent HD in hemodynamically unstable patients; also lowers ammonia and lactate, manages fluid overload
- Avoid nephrotoxic agents
- Maintain adequate MAP (>65 mmHg) for renal perfusion
5. Coagulopathy and Bleeding Management
- Coagulopathy (raised INR/PT) is both a marker of severity and a cause of bleeding
- Do NOT correct INR with FFP routinely as it is used as a prognostic marker; only correct before invasive procedures or in the setting of active bleeding
- Vitamin K 10 mg IV (may improve PT if cholestasis is contributing)
- Platelets: Transfuse if <50,000 before invasive procedures
- Recombinant factor VIIa: Consider for life-threatening hemorrhage
- Avoid NSAIDs and anticoagulants
6. Metabolic and Nutritional Management
- Hypoglycemia: Common; monitor blood glucose every 1-2 hours; correct with 10-50% dextrose infusion (blood glucose target 6-10 mmol/L)
- Hyponatremia: Avoid hypotonic fluids; if dilutional, fluid restrict; hypertonic saline for severe cases
- Hypokalemia, hypomagnesemia, hypophosphatemia: Monitor and replace
- Metabolic acidosis: Treat underlying cause (hypoperfusion); if persistent, initiate CRRT
- Nutrition: Enteral nutrition via NG tube within 24 hours of ICU admission (25-30 kcal/kg/day, 1-1.2 g protein/kg/day); do not restrict protein except in severe uncontrolled hyperammonemia
7. Infection Prevention and Management
- ALF patients are highly susceptible to bacterial (Gram-positive and Gram-negative) and fungal infections
- Low threshold for blood cultures and empiric broad-spectrum antibiotics if clinical deterioration
- Prophylactic antifungals: Fluconazole considered
- Infection can precipitate or worsen encephalopathy; treat aggressively
- Avoid unnecessary invasive lines/catheters where possible
8. Respiratory Support
- Mechanical ventilation for Grade 3-4 encephalopathy
- Use lung-protective ventilation (6 ml/kg tidal volume)
- Avoid high PEEP that increases intrathoracic pressure and raises ICP
- Treat ARDS if present
9. Specific Antidotes and Disease-Directed Therapy
- Acetaminophen: N-acetylcysteine (NAC) - standard dose IV; beneficial even with late presentation for its inotropic and anti-inflammatory effects
- HBV: Nucleoside analogues (tenofovir, entecavir) - even in acute HBV ALF to reduce viremia and for potential reactivation
- Amanita phalloides: IV penicillin G and silymarin (milk thistle)
- AIH: Glucocorticoids are controversial (may precipitate infection); consider only in absence of sepsis
- Wilson disease: D-penicillamine; liver transplant if established ALF
- AFLP/HELLP: Delivery of the fetus (emergency cesarean section)
10. Prognostication and Liver Transplantation
- King's College Criteria (poor prognosis, consider urgent LT):
- Acetaminophen: arterial pH <7.25 after resuscitation, OR all of: INR >6.5 + creatinine >300 μmol/L + Grade 3-4 encephalopathy
- Non-acetaminophen: INR >6.7 alone, OR any 3 of: unfavorable etiology, age <10 or >40, jaundice >7 days before encephalopathy, bilirubin >300 μmol/L, INR >3.5
- MELD score (Model for End-Stage Liver Disease) increasingly used
- Orthotopic liver transplantation (OLT) is the definitive treatment for ALF that does not recover spontaneously; ALF patients receive highest priority on the transplant list
- Auxiliary liver transplantation (partial transplant): Allows native liver to regenerate while the auxiliary graft supports function; immunosuppression can later be withdrawn
- Extracorporeal liver support systems (MARS - Molecular Adsorbent Recirculating System, Prometheus, plasma exchange): Bridge to transplant or native liver recovery; mixed evidence on survival benefit
(Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Plum and Posner's Diagnosis and Treatment of Stupor and Coma; Bailey and Love's Short Practice of Surgery, 28th Ed)
Summary Table for Quick Revision:
| System | Key Issue in ALF | Key Management |
|---|---|---|
| Neurological | Cerebral edema, raised ICP | Mannitol, hypertonic saline, ICP monitoring, mild hypothermia |
| Cardiovascular | Vasodilation, hypotension | Noradrenaline, fluids |
| Renal | AKI in ~55% | CRRT preferred |
| Coagulation | Coagulopathy, bleeding | Vitamin K; FFP only for procedures/active bleed |
| Metabolic | Hypoglycemia, hypoNa, acidosis | Glucose monitoring, electrolyte replacement, CRRT |
| Nutrition | Catabolism | Enteral feeding within 24h, 25-30 kcal/kg/day |
| Infection | Bacterial/fungal sepsis | Low threshold for cultures and antibiotics |
| Respiratory | Encephalopathy, ARDS | Mechanical ventilation, lung-protective strategy |
| Definitive | Liver failure | Liver transplantation (King's criteria) |
ECMO for 5 marks and ventilator associate pneumonia for 5 marks from standard anaesthesia source
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.