reactive arthritis whole topic discussion
Reading File
Finding Sources
Searching PubMed
"reactive arthritis"[MeSH Terms]
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Searching Images
reactive arthritis keratoderma blenorrhagicum skin lesions
Reading File
Searching Images
reactive arthritis circinate balanitis oral ulcers conjunctivitis
I now have comprehensive data from multiple authoritative textbooks. Let me compile the full topic discussion.
Reactive Arthritis — Comprehensive Review
1. Definition & Nomenclature
Reactive arthritis (ReA) is an aseptic, inflammatory arthritis that arises subsequent to an extra-articular infection — most typically of the gastrointestinal (GI) or genitourinary (GU) tract — where no viable organism can be cultured directly from the inflamed joint. It is classified within the spondyloarthritis (SpA) family, alongside ankylosing spondylitis (AS), psoriatic arthritis, and IBD-associated arthritis.
Formerly called Reiter syndrome (or Fiessinger-Leroy syndrome), this term is now largely abandoned due to its historical association with war-crime perpetrators. The classic triad of urethritis + conjunctivitis + arthritis is present in the minority of patients.
- Goldman-Cecil Medicine, 26th ed.; Fitzpatrick's Dermatology, 9th ed.
2. Epidemiology
| Parameter | Details |
|---|---|
| Peak age | 3rd–5th decade of life |
| Sex | Male predominance for post-venereal form; equal sex in enteric form |
| Prevalence | ~20–40 per 100,000 |
| Incidence | ~25 per 100,000/year |
| Risk after GI outbreak | 2–7% of infected; up to 20% in HLA-B27 positive individuals |
| Risk after Chlamydia | ~8% develop ReA |
| HLA-B27 | Present in 30–50% of ReA patients; associated with more severe and chronic disease |
Epidemiologic studies are challenging due to lack of validated, standardized diagnostic criteria. GU infections may be asymptomatic in the majority, which accounts for underdiagnosis — especially in women (cervicitis is less symptomatic than urethritis).
- Fitzpatrick's Dermatology; Goldman-Cecil Medicine
3. Etiology & Triggering Pathogens
Gastrointestinal (Enteric) Pathogens
- Salmonella typhimurium
- Yersinia enterocolitica
- Shigella flexneri
- Campylobacter jejuni
- Clostridium difficile
- Escherichia coli (occasionally)
Genitourinary (Venereal) Pathogens
- Chlamydia trachomatis — the most common offender
- Ureaplasma urealyticum
- Chlamydia pneumoniae
Other described triggers include intravesicular Bacillus Calmette-Guérin (BCG) therapy. Streptococcal pharyngitis, Giardia infection, and Chlamydia pneumoniae have been associated with postinfectious syndromes but lack the full spondyloarthritis phenotype and HLA-B27 association of classic ReA.
4. Pathobiology
Mechanism of Aseptic Arthritis
Although the joint itself is sterile by culture, bacterial antigens and even viable organisms may persist in synovial tissue:
- PCR studies of synovial tissue are most consistently positive in post-Chlamydia ReA, suggesting viable organisms persist in a metabolically altered state within joints.
- Immunofluorescence studies show bacterial antigens in joints after both GI and GU infections.
Immune Pathways
- Genetic susceptibility: HLA-B27 confers risk for onset, axial involvement, and chronicity.
- Toll-like receptor 2 (TLR-2) genetic variants implicate host innate immunity as central.
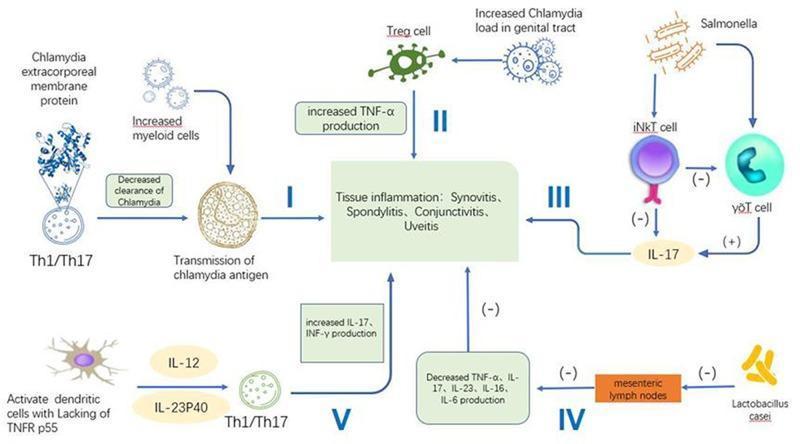
- Th1/Th17 dysregulation, elevated TNF-α, IL-17, and IL-23 are key cytokine axes.
- Decreased Chlamydia clearance and antigen presentation perpetuate inflammation.
Dactylitis
Dactylitis ("sausage digit") is the net result of inflammatory changes simultaneously affecting the joint capsule, entheses, periarticular structures, and periosteal bone — not just the joint itself.
5. Clinical Manifestations
Onset
Arthritis develops 1–4 weeks after the triggering GI or GU infection.
Articular Features
| Feature | Description |
|---|---|
| Pattern | Asymmetric oligoarthritis (2–4 joints), lower limb predominance |
| Common joints | Knees, ankles, feet; MTP joints |
| Enthesitis | Achilles tendinitis, plantar fasciitis |
| Dactylitis | "Sausage digits" — entire digit involvement |
| Sacroiliitis | Often unilateral (vs. bilateral in AS) — may appear in acute or chronic phase |
| Axial involvement | Asymmetric, bulky, non-marginal syndesmophytes (vs. fine marginal ones in AS) |
Extra-articular Features
1. Genitourinary
- Urethritis/Cervicitis: dysuria, purulent discharge (may be asymptomatic in women)
- Circinate balanitis: shallow, painless ulcerations or vesicles on the glans penis; circinate (serpiginous) margins

2. Ocular
- Conjunctivitis: bilateral, painful; most common ocular manifestation
- Anterior uveitis: tends to be unilateral, less painful than conjunctivitis; can occur in chronic disease

3. Cutaneous — Key Manifestations
Keratoderma blenorrhagicum (KB)
- The classic skin lesion of ReA
- Painless papulosquamous eruption on the palms and soles
- Begins as vesicles or pustules → evolves into hyperkeratotic, "mountain-in-relief" plaques with waxy, yellow-brown scale
- Histologically identical to pustular psoriasis


Nail changes
- Pitting, onycholysis, subungual keratosis (similar to psoriatic nail disease)
Oral ulcers
- Painless lingual and oral mucosal ulcerations (aphthous-like)
Circinate vulvitis
- Equivalent to circinate balanitis in females; linear ulcerations at the base of labia majora folds.
4. Cardiac
- Aortic regurgitation (rare, seen in chronic disease with significant HLA-B27 positivity)
- Conduction abnormalities (rarely AV block)
6. Diagnosis
1995 Third International Workshop Criteria (most cited, not formally validated)
- Arthritis predominantly involving the lower limb, oligoarticular, and asymmetric
- Evidence of preceding infection: either a positive culture OR documented diarrhea/urethritis in the prior 4 weeks (culture confirmation not required)
- Exclusion of septic arthritis and other causes of oligoarthritis (gout, pseudogout, RA, other SpA)
Laboratory Workup
| Test | Finding |
|---|---|
| ESR / CRP | Elevated (nonspecific) |
| RF / ANA | Negative (seronegative arthropathy) |
| HLA-B27 | Positive in 30–50%; not diagnostic; helps assess chronicity risk |
| Synovial fluid | Sterile inflammation; WBC 4,000–50,000/μL, PMN predominance; negative crystals, Gram stain, and culture |
| Stool/urine cultures | For Shigella, Salmonella, Yersinia, Campylobacter, C. difficile |
| Chlamydia NAAT | Urethral/cervical swab or urine |
| Serology for enteric pathogens | Not reliable — not recommended |
Synovial fluid differentiates ReA (sterile, <50,000 WBC) from septic arthritis (>50,000 WBC, positive Gram stain/culture).
7. Imaging
Plain Radiography
- Often normal in early/acute disease
- Soft tissue swelling and juxta-articular osteopenia are early signs
- Periostitis and new bone formation ("whiskering") appear in peripheral joints with chronicity
Sacroiliac Joints
- Unilateral sacroiliitis with erosions, pseudowidening, ileal sclerosis
- Contrast to AS: bilateral, symmetrical sacroiliitis

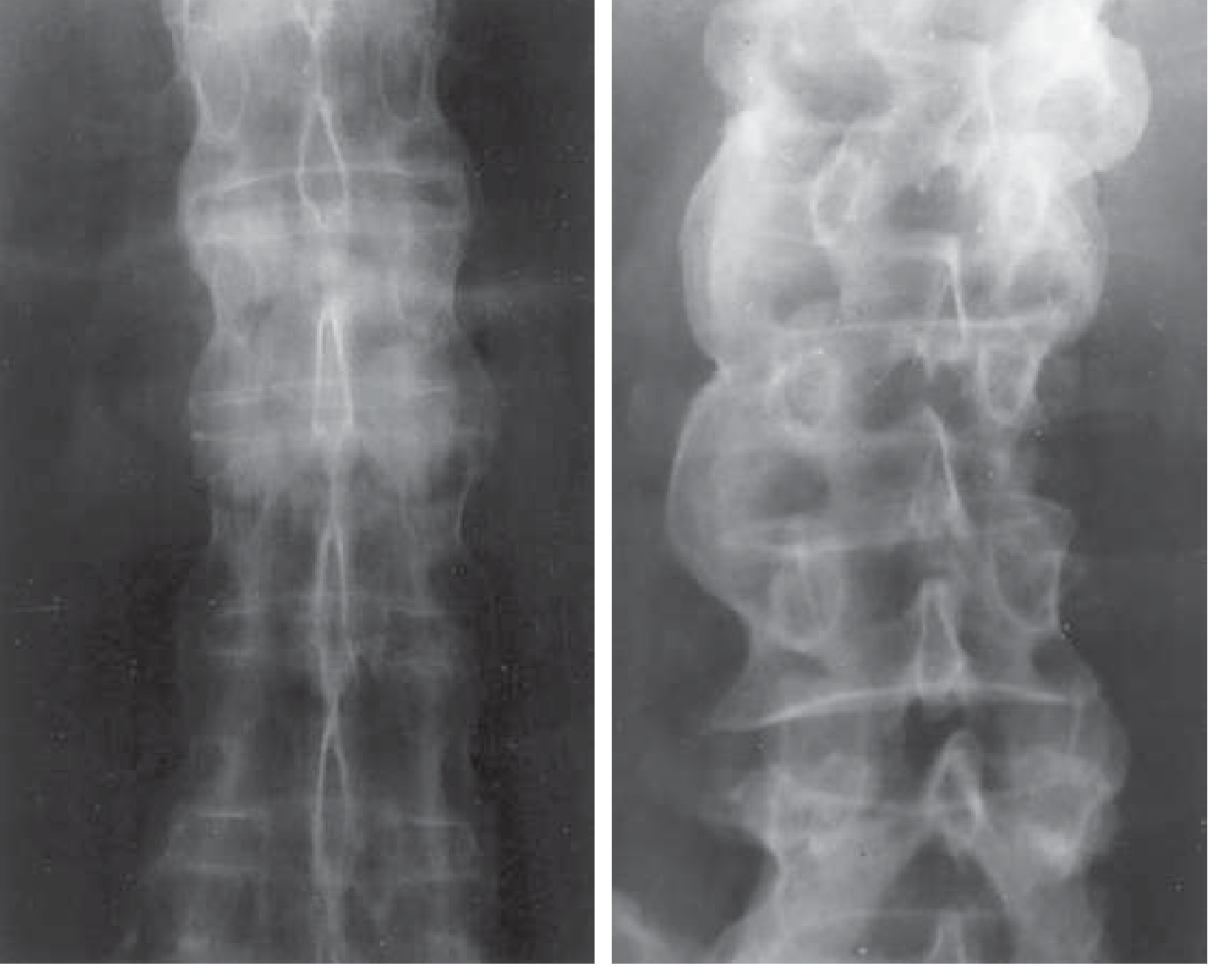
Spine
- Asymmetric, bulky, non-marginal syndesmophytes (differ from the fine marginal syndesmophytes of AS)
- In advanced disease: "bamboo spine" from ligament calcification and ankylosis
8. Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Septic arthritis | Monoarthritis; culture-positive synovial fluid; WBC >50,000/μL; Gram stain +ve |
| Disseminated gonococcal infection | Migratory polyarthritis; skin pustules; positive gonorrhea culture |
| Lyme disease | Tick exposure; serologic evidence; migratory arthritis |
| Gout / Pseudogout | Urate or CPP crystals in synovial fluid |
| Psoriatic arthritis | Psoriatic skin/nail changes; DIP involvement; RF negative |
| Ankylosing spondylitis | Bilateral symmetric sacroiliitis; younger male; no preceding infection |
| Rheumatoid arthritis | Symmetric small-joint polyarthritis; RF+ / anti-CCP+ |
| SLE | ANA+; multi-system involvement |
| IBD-associated arthritis | GI symptoms of IBD; peripheral arthritis correlates with disease activity |
| Viral arthritis (HIV, Parvovirus B19) | Polyarthritis rather than oligoarthritis |
| Subacute bacterial endocarditis | Murmur; blood cultures positive; embolic phenomena |
9. ReA in HIV Infection
ReA is not more frequent in HIV, but HIV alters the course:
- More aggressive and refractory joint disease
- Additive, asymmetrical polyarthritis OR intermittent lower-extremity oligoarthritis
- Enthesitis, fasciitis, conjunctivitis, and urethritis can all occur
- Most North American patients with HIV-ReA are B27 positive, but African cohorts show a significant B27-negative subgroup
- Extensive spinal syndesmophyte formation is uncommon
Preferred treatment in HIV-associated ReA: acitretin, sulfasalazine, and antiretroviral therapy (ART); avoid immunosuppressive agents.
10. Treatment
Step 1: Treat the Triggering Infection
| Pathogen | Treatment |
|---|---|
| C. trachomatis | Azithromycin 1 g single dose OR doxycycline 100 mg BD × 7 days; treat sexual partner |
| Enteric pathogens | Antibiotics if active infection confirmed |
| Chlamydia-induced chronic ReA (PCR+) | Combination antibiotic therapy for 6 months: rifampin 300 mg/day + doxycycline 100 mg BD OR azithromycin 500 mg/day × 5 days, then 500 mg weekly → ~65% response rate, 20% complete remission vs 0% placebo |
Long-term antibiotics for non-Chlamydia ReA with ongoing synovitis have no convincing evidence of benefit.
Step 2: NSAIDs
- First-line symptomatic therapy for acute ReA
- Prescription-strength preparations (e.g., indomethacin, naproxen, diclofenac)
- Provide antiinflammatory and analgesic effects
- Do not alter or shorten the natural course of disease
- Caution in renal/hepatic insufficiency and GI risk patients
Step 3: Corticosteroids
| Route | Indication |
|---|---|
| Intraarticular injection | Oligoarticular flare; short-term relief |
| Systemic (oral) | More widespread joint involvement; limited benefit for axial disease |
| Topical | Keratoderma blenorrhagicum, inflammatory eye disease, circinate balanitis |
Step 4: Disease-Modifying Antirheumatic Drugs (DMARDs)
| Drug | Role |
|---|---|
| Sulfasalazine 1–2 g/day | Preferred DMARD; improves peripheral arthritis; best started within first 3 months; no effect on axial disease |
| Methotrexate 7.5–25 mg/week | Peripheral joint benefit; no robust axial benefit |
| Leflunomide | Used for peripheral disease; less data in ReA specifically |
Step 5: Biologics (Chronic/Refractory Disease)
| Agent | Class | Notes |
|---|---|---|
| Etanercept, Infliximab, Adalimumab, Golimumab | Anti-TNF-α | Most data; used in chronic HLA-B27+ spondyloarthritis; efficacy in ReA unproven but commonly used |
| Secukinumab, Ixekizumab | Anti-IL-17A | Effective in SpA generally |
| Tofacitinib (JAK inhibitor) | JAK1/3 inhibitor | Emerging evidence for refractory ReA (case reports, including refractory KBs) |
~50% of ReA patients recover within 6 months, so biologics are generally reserved for chronic, HLA-B27-positive, DMARD-refractory disease.
11. Prognosis & Course
| Feature | Detail |
|---|---|
| Typical course | Self-limited in weeks to months for most |
| Chronic ReA | Defined as symptoms persisting beyond 6 months; ~30–40% of patients |
| HLA-B27 | Strongest predictor of chronicity, axial involvement, and severity |
| Evolution to AS | Frequency of progression to bona fide AS is not definitively established |
| Recurrence | Possible with re-exposure to triggering pathogens |
12. Summary at a Glance
| Domain | Key Points |
|---|---|
| Definition | Aseptic oligoarthritis 1–4 weeks post-GI/GU infection; spondyloarthritis family |
| Triad | Urethritis + conjunctivitis + arthritis (rarely all 3 present simultaneously) |
| Key pathogens | C. trachomatis (GU); Salmonella, Shigella, Yersinia, Campylobacter (GI) |
| Pathology | Sterile joint; bacterial antigens/DNA persist; Th1/Th17; HLA-B27 |
| Arthritis | Asymmetric oligoarthritis, lower limb; dactylitis; enthesitis |
| Skin | Keratoderma blenorrhagicum (palms/soles), circinate balanitis, oral ulcers, nail changes |
| Sacroiliac | Unilateral, asymmetric; distinct from bilateral symmetric AS |
| Spine | Bulky, non-marginal asymmetric syndesmophytes |
| Diagnosis | Clinical + exclusion; synovial fluid sterile; HLA-B27 for prognosis |
| Treatment | Treat infection → NSAIDs → intraarticular/systemic steroids → sulfasalazine → biologics |
| Prognosis | ~50–70% self-limited; ~30% chronic; HLA-B27 = chronic risk |
Sources: Goldman-Cecil Medicine (International Edition); Fitzpatrick's Dermatology (9th ed.); Textbook of Family Medicine (9th ed.); Grainger & Allison's Diagnostic Radiology; Robbins & Cotran Pathologic Basis of Disease; Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Harrison's Principles of Internal Medicine (22nd ed., 2025)
diff beyween septic and reactive
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
I now have all the data needed. Here is a comprehensive, well-organized comparison:
Septic Arthritis vs. Reactive Arthritis — Full Comparison
Core Conceptual Difference
| Septic Arthritis | Reactive Arthritis | |
|---|---|---|
| Nature | Live organisms within the joint (infective) | Sterile joint — immune response to a remote infection |
| Urgency | Orthopedic emergency | Urgent but not immediately joint-destructive |
| Organism in joint | Yes — culturable | No — culture-negative |
1. Etiology & Pathogenesis
| Septic Arthritis | Reactive Arthritis | |
|---|---|---|
| Mechanism | Hematogenous seeding, direct inoculation, contiguous spread from osteomyelitis | Immune-mediated (Th1/Th17, TNF-α, HLA-B27) response to remote mucosal infection |
| Organisms | S. aureus (most common), Streptococci, Gram-negatives, Gonococci (sexually active adults), Pseudomonas (IV drug users) | No organism in joint; triggered by Chlamydia trachomatis (GU), Salmonella, Shigella, Yersinia, Campylobacter, C. difficile (GI) |
| Route of infection | Bacteremia → synovial membrane invasion | Infection occurs distally (GI/GU tract) → arthritis 1–4 weeks later |
| Joint involvement | Direct destruction by live bacteria and proteases | Immune complex and T-cell mediated synovitis |
2. Epidemiology & Risk Factors
| Septic Arthritis | Reactive Arthritis | |
|---|---|---|
| Incidence | 2–10/100,000 (native joints) | 20–40/100,000 prevalence |
| Peak age | Any age; neonates, elderly, immunocompromised | 3rd–5th decade |
| Sex | No strong predilection | Male predominance (post-venereal form) |
| Risk factors | Rheumatoid arthritis, DM, prosthetic joint, IV drug use, immunosuppression, recent joint surgery | HLA-B27 positivity, prior GI/GU infection, sexual exposure |
| Genetic marker | None specific | HLA-B27 (30–50% of ReA patients) |
3. Clinical Features
| Feature | Septic Arthritis | Reactive Arthritis |
|---|---|---|
| Onset | Acute, hours to days | 1–4 weeks after infection |
| Fever | Present in >80% of children, ~40% of adults | May be low-grade or absent |
| Number of joints | Usually monoarticular (<10–20% polyarticular) | Oligoarticular (2–4 joints) |
| Symmetry | Usually single joint | Asymmetric |
| Joint distribution | Knee (50%), hip (25%), shoulder (15%); any large joint | Lower limb predominance (knee, ankle, foot) |
| Enthesitis | No | Yes — Achilles tendinitis, plantar fasciitis |
| Dactylitis | No | Yes — "sausage digit" |
| Sacroiliac involvement | Rare; SI joint septic arthritis is a specific entity | Yes — unilateral asymmetric sacroiliitis |
| Preceding infection history | May have bacteremic source (skin, respiratory, endocarditis) | Clear history of diarrhea or urethritis 1–4 weeks prior |
| Pain severity | Exquisite; any motion intolerable | Moderate inflammatory pain |
| Inability to bear weight | Common | Variable |
| Systemic toxicity | Often present (tachycardia, hypotension in severe cases) | Usually absent |
4. Extra-articular Manifestations
| Feature | Septic Arthritis | Reactive Arthritis |
|---|---|---|
| Skin | Possible pustular lesions in gonococcal dissemination | Keratoderma blenorrhagicum (palms/soles), circinate balanitis/vulvitis |
| Eyes | No | Conjunctivitis (bilateral), anterior uveitis (unilateral) |
| Mucous membranes | No | Painless oral/lingual ulcers |
| GU | No | Urethritis, cervicitis (may be asymptomatic) |
| Cardiac | Possible if endocarditis-related | Aortic regurgitation, conduction defects (chronic) |
| Nails | No | Pitting, onycholysis, subungual keratosis |
The classic triad of urethritis + conjunctivitis + arthritis = reactive arthritis; this triad does NOT occur in septic arthritis.
5. Synovial Fluid Analysis — The Key Differentiator
| Parameter | Septic Arthritis | Reactive Arthritis |
|---|---|---|
| Appearance | Turbid, purulent | Turbid/inflammatory |
| WBC count | Usually >50,000/μL (often >100,000) | 4,000–50,000/μL |
| Differential | PMN predominance (>90%) | PMN predominance |
| Gram stain | Positive in ~50–75% | Negative |
| Culture | Positive (definitive diagnosis) | Negative (sterile) |
| Crystals | Negative | Negative |
| Glucose | Low | Normal or mildly low |
| Lactate | High | Normal |
Arthrocentesis is mandatory whenever septic arthritis is suspected. A positive Gram stain or culture confirms septic arthritis. Sterile fluid with <50,000 WBC favors reactive arthritis.
6. Laboratory & Serology
| Test | Septic Arthritis | Reactive Arthritis |
|---|---|---|
| WBC (serum) | Elevated | Mildly elevated or normal |
| ESR / CRP | Markedly elevated | Elevated (nonspecific) |
| Procalcitonin | Elevated (90% specific for septic arthritis) | Normal or mildly elevated |
| Blood cultures | Positive in bacteremia (~25–50%) | Negative |
| RF / ANA | Negative | Negative |
| HLA-B27 | Not relevant | Present in 30–50% |
| Chlamydia NAAT | Negative | May be positive on urethral/cervical swab |
| Stool cultures | Negative | May be positive for triggering enteric pathogen |
| Uric acid | Normal | Normal |
7. Imaging
| Septic Arthritis | Reactive Arthritis | |
|---|---|---|
| Plain X-ray (early) | Soft tissue swelling, joint space widening; osteopenia | Soft tissue swelling, juxta-articular osteopenia |
| Plain X-ray (late) | Joint space narrowing, bone destruction, erosions | Periostitis ("whiskering"), unilateral sacroiliitis, asymmetric non-marginal syndesmophytes |
| MRI | Synovitis, effusion, adjacent osteomyelitis possible | Enthesitis, sacroilitis, bone marrow edema |
| Bone scan | Used for early detection; whole-body survey | Less commonly used |
8. Treatment
| Septic Arthritis | Reactive Arthritis | |
|---|---|---|
| Priority | Antibiotic therapy + joint drainage (emergency) | Treat underlying infection if still active |
| Antibiotics | Empiric IV antibiotics immediately after aspiration (S. aureus coverage: anti-staphylococcal PCN or vancomycin); tailored to culture results | Only if active Chlamydia (azithromycin 1 g single dose or doxycycline 100 mg BD × 7 days); no benefit for ongoing ReA in enteric-triggered cases |
| Joint drainage | Mandatory — surgical or serial aspiration | Not required; aspiration is diagnostic only |
| NSAIDs | Adjunct | First-line for symptoms |
| Corticosteroids | Contraindicated until infection controlled | Intraarticular or systemic for inflammation |
| DMARDs | Not used | Sulfasalazine (1–2 g/day), methotrexate for chronic disease |
| Biologics | Not used | Anti-TNF for chronic, HLA-B27+ refractory disease |
| Outcome | 25–50% loss of joint function even with treatment; 6–11% mortality | ~50–70% self-limited within 6 months; ~30% chronic |
9. Quick Memory Summary
| Criterion | Septic | Reactive |
|---|---|---|
| Culture | Positive | Negative |
| Fever | High, prominent | Low-grade/absent |
| Joints | Mono | Oligo (2–4) |
| WBC in fluid | >50,000 | 4,000–50,000 |
| Gram stain | Positive | Negative |
| Procalcitonin | High | Normal |
| Keratoderma/conjunctivitis/urethritis | No | Yes |
| HLA-B27 | No relevance | 30–50% positive |
| Preceding infection timing | Concurrent bacteremia | 1–4 weeks prior |
| Emergency | Yes | No |
| Treatment | IV antibiotics + drainage | NSAIDs → DMARDs |
Sources: Goldman-Cecil Medicine; Rosen's Emergency Medicine; Tintinalli's Emergency Medicine; Textbook of Family Medicine; Fitzpatrick's Dermatology; Quick Compendium of Clinical Pathology; Tietz Textbook of Laboratory Medicine
vbg what to see
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive data. Here is a complete, well-structured answer:
Venous Blood Gas (VBG) — What to Look For
What Is a VBG?
A VBG is obtained from peripheral or central venous blood (vs. arterial puncture for ABG). It is easier, less painful, and faster to obtain — making it the preferred first-line gas in most ED and ward settings. The key is knowing what it can and cannot reliably tell you.
VBG Normal Reference Values
| Parameter | Normal VBG Value | Comparison to ABG |
|---|---|---|
| pH | 7.31 – 7.41 | ~0.03–0.05 lower than ABG pH |
| PCO₂ | 41 – 51 mmHg | ~6–8 mmHg higher than PaCO₂ |
| HCO₃⁻ | 22 – 26 mEq/L | ~1–2 mEq/L higher than ABG |
| Base Excess | −2 to +2 | Very close to ABG |
| PO₂ | 30 – 50 mmHg | NOT comparable to PaO₂ — cannot assess oxygenation |
| SpO₂ (if reported) | Variable | Not useful from venous sample |
| Lactate | < 2 mmol/L | Correlates well with arterial lactate except in mildly elevated range |
The Golden Rule: What VBG CAN vs. CANNOT Tell You
| Question | VBG Reliable? | Notes |
|---|---|---|
| Is the pH acidotic or alkalotic? | ✅ Yes | ±0.03–0.05 of ABG; clinically acceptable |
| Is there hypercapnia (CO₂ retention)? | ✅ Partial | PvCO₂ <45 mmHg = nearly 100% negative predictive value for ruling OUT hypercapnia (PaCO₂ >50 mmHg) |
| What is the bicarbonate? | ✅ Yes | Closely mirrors ABG HCO₃⁻ |
| Is there a metabolic acidosis/alkalosis? | ✅ Yes | Use HCO₃⁻ and base excess |
| Is the patient hypoxic? | ❌ No | PvO₂ does NOT correlate with PaO₂; use pulse oximetry (SpO₂) instead |
| Is lactate elevated? | ✅ Mostly | Normal and markedly elevated values correlate well; mildly elevated (2–4 mmol/L) may need arterial confirmation |
| Mixed venous saturation (ScvO₂)? | ✅ (central VBG) | Useful in sepsis and cardiac output assessment |
The combination of VBG + SpO₂ adequately screens for acid-base disturbance AND hypoxemia in most patients without needing an ABG.
Step-by-Step: How to Interpret a VBG
Step 1 — Check the pH
- < 7.31 → Acidosis
- > 7.41 → Alkalosis
- Normal → May still have mixed disorder (compensated)
Step 2 — Identify Primary Disturbance
| pH | HCO₃⁻ | PCO₂ | Primary Disorder |
|---|---|---|---|
| ↓ | ↓ | ↓ (compensated) | Metabolic acidosis |
| ↑ | ↑ | ↑ (compensated) | Metabolic alkalosis |
| ↓ | ↑ (compensated) | ↑ | Respiratory acidosis |
| ↑ | ↓ (compensated) | ↓ | Respiratory alkalosis |
Step 3 — Assess Compensation (Is it appropriate?)
For metabolic acidosis → Expected PaCO₂ = 1.5 × HCO₃⁻ + 8 ± 2 (Winter's formula)
(For VBG, add ~6 mmHg to expected value, or compare PvCO₂ to expected PaCO₂ + 6)
For metabolic alkalosis → Expected PaCO₂ = 0.7 × HCO₃⁻ + 21 ± 2
For respiratory acidosis (acute) → HCO₃⁻ rises by 1 mEq/L per 10 mmHg ↑ PCO₂
For respiratory acidosis (chronic) → HCO₃⁻ rises by 3.5 mEq/L per 10 mmHg ↑ PCO₂
Step 4 — Calculate Anion Gap (if metabolic acidosis)
AG = Na⁺ – (Cl⁻ + HCO₃⁻) Normal = 8–12 mEq/L (albumin-corrected)
High AG acidosis (MUDPILES / GOLDMARK):
- Methanol, Uraemia, DKA, Propylene glycol, Iron/Isoniazid, Lactic acidosis, Ethanol/Ethylene glycol, Salicylates
Normal AG (hyperchloraemic) acidosis:
- Diarrhoea, RTA, saline excess, Addison's
Step 5 — Check Lactate
| Level | Interpretation |
|---|---|
| <2 mmol/L | Normal |
| 2–4 mmol/L | Mild elevation; may need arterial confirmation |
| >4 mmol/L | Significant hypoperfusion/anaerobic metabolism; correlates well with arterial |
When to Upgrade to an ABG
| Situation | Reason |
|---|---|
| Suspected hypoxic respiratory failure (SpO₂ unreliable: CO poisoning, methaemoglobinaemia, poor perfusion) | PvO₂ cannot assess oxygenation |
| PvCO₂ ≥45 mmHg and respiratory failure suspected | Need precise PaCO₂ for ventilator management |
| Complex mixed acid-base disorder | More precise PaCO₂ for compensation formulas |
| ARDS severity assessment (P/F ratio) | Requires PaO₂ |
| Patient on NIV/mechanical ventilation requiring titration | Precise CO₂ monitoring needed |
VBG in Specific Clinical Contexts
| Condition | VBG Role |
|---|---|
| DKA | pH, HCO₃⁻, anion gap, lactate — all reliable; VBG adequate to monitor response |
| Sepsis | pH, lactate (central ScvO₂ from central VBG); no need for ABG if SpO₂ satisfactory |
| Asthma | PvCO₂ <45 mmHg rules out hypercapnia; if ≥45 mmHg, get ABG |
| COPD exacerbation | Screen with VBG; if PvCO₂ elevated or pH low, confirm with ABG |
| Cardiac arrest / shock | VBG pH and lactate give rapid picture; not reliable in severe low-flow states |
| Metabolic alkalosis | VBG HCO₃⁻ and pH reliable |
| Paediatrics | VBG (or capillary BG) preferred to reduce arterial punctures; PCO₂ correlation moderate |
VBG vs. ABG — Summary
| Feature | ABG | VBG |
|---|---|---|
| Oxygenation (PO₂) | ✅ Direct | ❌ Not usable |
| pH | ✅ Gold standard | ✅ Reliable (±0.03–0.05) |
| PCO₂ | ✅ Gold standard | ✅ Reliable as screen; add ~6–8 mmHg for PaCO₂ estimate |
| HCO₃⁻ / BE | ✅ | ✅ |
| Lactate | ✅ | ✅ (mostly) |
| Pain / Difficulty | High (arterial) | Low (venous) |
| Speed | Slower (puncture setup) | Faster (routine blood draw) |
| Complication risk | Haematoma, vasospasm | Minimal |
Sources: Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases; Roberts & Hedges' Clinical Procedures in Emergency Medicine; Harriet Lane Handbook (23rd ed.)
This is a shared conversation. Sign in to Orris to start your own chat.