Cardiopulmonary bypass for md anaesthesia exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compile a thorough, exam-focused response.
Cardiopulmonary Bypass (CPB) — MD Anaesthesia Exam Notes
1. Definition & Purpose
CPB diverts venous blood away from the heart (via cannulae in the right atrium/vena cavae), oxygenates it, removes CO₂, and returns it via an arterial cannula (usually ascending aorta or femoral artery). It provides both artificial circulation and ventilation, allowing the surgeon a bloodless, motionless field.
Key non-physiological features:
- Mean arterial pressure lower than normal
- Flow is usually non-pulsatile
- Varying degrees of systemic hypothermia
- Hemodilution from circuit priming
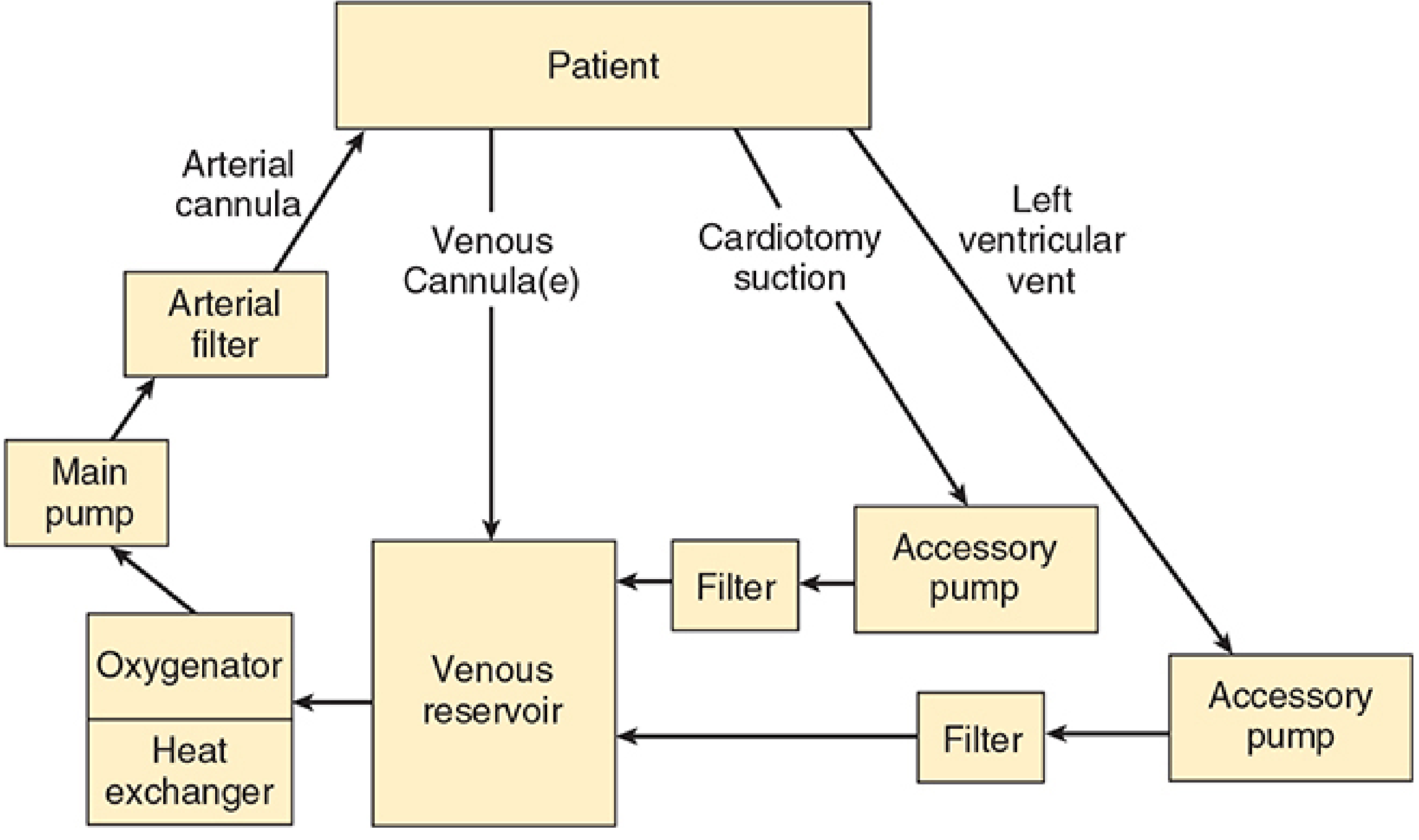
2. Components of the CPB Circuit
| Component | Function |
|---|---|
| Venous reservoir | Receives deoxygenated blood by gravity drainage from RA/IVC/SVC; acts as buffer |
| Oxygenator | Gas exchange via thin silicone gas-permeable membrane; volatile agent can be added |
| Heat exchanger | Cools/rewarems blood by water conduction; filter traps bubbles during rewarming |
| Main pump | Propels blood (roller or centrifugal) |
| Arterial line filter | Traps particulate/gaseous emboli before blood returns to patient |
| Accessory pumps | Cardiotomy suction, LV vent, cardioplegia delivery |
Pump Types — Key Exam Distinction
| Feature | Roller pump | Centrifugal pump |
|---|---|---|
| Mechanism | Positive displacement; compresses tubing | Spinning cones — centrifugal force |
| Flow | Fixed per RPM (non-pulsatile) | Pressure-sensitive; needs flowmeter |
| Air embolism risk | Can pump air — dangerous if reservoir empty | Cannot pump air — safer |
| Haemolysis | More trauma to RBCs | Less traumatic |
| Position in circuit | After oxygenator | Between reservoir and oxygenator |
3. Circuit Priming
- Volume: 1200–1800 mL for adults (crystalloid — usually lactated Ringer's)
- Common additives: colloid (albumin/starch), mannitol (diuresis), heparin (500–5000 units), bicarbonate
- Causes hemodilution → haematocrit falls to 22–27% at onset of bypass
- Blood added to prime for: neonates, infants, severely anaemic adults
4. Anticoagulation for CPB
Heparin
- Required to prevent clotting in the extracorporeal circuit
- Dose: 300–400 units/kg IV (target ACT > 400–480 seconds before bypass)
- Mechanism: potentiates antithrombin III → inhibits factors IIa (thrombin), Xa, IXa, XIa, XIIa
- Monitoring: Activated Clotting Time (ACT)
- Normal ACT: < 130 s
- Target on CPB: > 400–480 s (most centres use > 480 s)
Protamine Reversal
- Dose: ~1 mg per 100 units of heparin given (typically 3–4 mg/kg)
- Adverse reactions:
- Hypotension (most common) — from histamine release or complement activation
- Anaphylaxis (especially in patients with fish allergy or prior protamine exposure, e.g. NPH insulin users)
- Pulmonary hypertension (catastrophic — complement-mediated thromboxane release)
- If heparin not adequately reversed → coagulopathy post-bypass
5. Myocardial Protection
Goal: provide bloodless, motionless field while minimising ischaemic injury.
Cardioplegia
- Chemical solution that arrests myocardial electrical activity
- Delivered antegrade (into aortic root/coronary ostia) or retrograde (via coronary sinus)
- Composition:
- High potassium (20–40 mEq/L) → depolarises and arrests the heart in diastole
- Cold temperature (4°C) reduces metabolic demand
- Other additives: blood, bicarbonate, magnesium, glutamate, aspartate
| Cardioplegia Type | Contents | Notes |
|---|---|---|
| Cold crystalloid | Saline + K⁺ | Standard; arrest + hypothermia |
| Cold blood | 4:1 blood:crystalloid | Better oxygen delivery |
| Warm blood (Buckberg) | Normothermic blood + K⁺ | Continuous delivery; induction/terminal warm shot |
| Del Nido | Crystalloid-based | Popular in paeds/adults; single dose lasts ~60 min |
Topical hypothermia
- Ice slush around the heart provides additional protection against rewarming
6. Temperature Management
| Phase | Core Temp | Purpose |
|---|---|---|
| Mild hypothermia | 32–35°C | Reduces metabolic demand |
| Moderate hypothermia | 25–32°C | Most CABG/valve surgery |
| Deep hypothermia (DHCA) | ≤18°C | Allows circulatory arrest (complex congenital, aortic arch) |
- DHCA at 15–18°C allows up to 60 minutes of safe circulatory arrest
- Brain protection during DHCA: ice packing around head, methylprednisolone 30 mg/kg, mannitol 0.5 g/kg
pH Management During Hypothermia
| Strategy | Principle | Use |
|---|---|---|
| Alpha-stat | Maintain pH 7.40 at 37°C uncorrected; allows cerebral autoregulation | Adults; most CABG |
| pH-stat | Add CO₂ to maintain pH 7.40 corrected for actual temperature; causes cerebral vasodilation | Better neurological outcomes in paediatric DHCA |
7. Conduct of CPB — Phases
Pre-bypass
- Heparinisation (confirm ACT > 400–480 s before cannulation)
- Arterial cannula inserted first (ascending aorta), then venous (RA or bicaval)
- TEE inserted; lines zeroed; baseline ACT, ABG, K⁺, glucose
Initiation of Bypass
- Surgeon: "Going on bypass"
- Anesthesiologist: stops ventilation (lungs collapse), turns off volatile agent (will be delivered via oxygenator)
- Perfusionist: gradually increases pump flow to 2.2–2.4 L/min/m² (full flow)
- Monitor: arterial line pressure, venous reservoir level, SvO₂, urine output, temperature
On Bypass
- Maintain MAP 50–80 mmHg — use phenylephrine (vasoconstriction) or sodium nitroprusside (vasodilation)
- Acceptable haematocrit: ≥21–25% (lower targets may be acceptable with hypothermia)
- Glucose: maintain < 180 mg/dL (hyperglycaemia worsens neurological outcome)
- K⁺ must be monitored frequently (cardioplegia loads potassium → hyperkalaemia risk)
- Cross-clamp applied to ascending aorta before cardioplegia delivery
- Pulmonary artery catheter must be withdrawn 2–3 cm (migrates distally during CPB → risk of PA rupture)
- Volatile agent delivery via oxygenator vaporiser (prevent awareness on CPB)
- Cooling → surgery → rewarming
Weaning from Bypass
Sequence:
- Rewarm to ≥37°C nasopharyngeal (bladder/rectal ≥35°C)
- Resume ventilation (confirm bilateral air entry, ETCO₂, good lung compliance)
- Defibrillate if needed (most hearts restart spontaneously or with defibrillation at 20 J)
- Ensure: sinus rhythm (or pace at 80–90 bpm), adequate filling, acceptable ABG/electrolytes
- Gradually reduce pump flow while heart takes over
- Decannulate → protamine administration (slow IV over 10–15 min; surgeon should be warned as it can cause pulmonary hypertension)
Failure to wean — causes: inadequate surgical repair, poor myocardial protection, metabolic derangement, tamponade. Management: inotropes, IABP, LVAD.
8. Monitoring During CPB
| Monitor | Purpose |
|---|---|
| Arterial line (radial/femoral) | Continuous MAP (radial may underread post-bypass) |
| CVP | Trend; also venous cannula function |
| PAC (if used) | LV filling, CO, SvO₂ |
| TEE | Ventricular function, de-airing, surgical result, valves |
| ACT | Adequacy of heparinisation |
| ABG, electrolytes | Acid-base, K⁺, Ca²⁺, glucose |
| Urinary output | Renal perfusion (target > 0.5 mL/kg/h) |
| Temperature | ≥2 sites: core (nasopharyngeal/bladder) + peripheral |
| Cerebral oximetry (NIRS) | Brain O₂ delivery; especially for aortic arch/carotid disease |
| Transcranial Doppler | Emboli detection; associated with neurocognitive decline |
9. Physiological Consequences of CPB
| System | Effect | Mechanism |
|---|---|---|
| Inflammatory | SIRS — activation of complement, cytokines, neutrophils | Blood–artificial surface contact |
| Haematological | Dilutional coagulopathy; platelet dysfunction; ↓ clotting factors | Hemodilution + activation/consumption |
| Renal | AKI — oliguria, ATN | Low flow, emboli, inflammatory mediators |
| Neurological | Stroke, cognitive dysfunction ("pumphead") | Macroembolism, microemboli, hypoperfusion |
| Pulmonary | Post-pump lung — ↑ interstitial fluid, atelectasis, ↑ A-a gradient | Inflammatory mediators, ischaemia-reperfusion |
| Endocrine | Hyperglycaemia, ↑ cortisol, ↑ catecholamines | Surgical stress response |
| GI | Gut ischaemia, pancreatitis | Non-pulsatile flow, emboli |
10. Complications of CPB
| Complication | Key Points |
|---|---|
| Air embolism | Roller pump + empty reservoir; deairing manoeuvres (Trendelenburg, needle aspiration) |
| Massive gas embolism | Oxygenator failure; immediate circulatory arrest, retrograde perfusion |
| Neurological injury | Stroke (~1–3% CABG), cognitive dysfunction (20–40%) |
| Coagulopathy | Dilution + platelet dysfunction + residual heparin; treat with FFP, platelets, cryoprecipitate, protamine |
| Protamine reaction | Hypotension, anaphylaxis, pulmonary HTN |
| Haemolysis | Red urine — excessive suction, prolonged bypass, roller pump |
| Vasoplegic syndrome | Severe vasoplegia post-CPB — treat with noradrenaline ± vasopressin ± methylene blue |
| Aortic dissection | Aortic cannulation complication |
| Low cardiac output | Poor myocardial protection, MI, inadequate repair |
11. Anesthetic Agents During CPB
- Induction: Etomidate (haemodynamic stability), ketamine (in compromised patients), midazolam, fentanyl/sufentanil, propofol
- Maintenance on CPB: Volatile agent via oxygenator (isoflurane, sevoflurane) + fentanyl infusion
- Awareness risk on CPB is real — BIS monitoring and volatile agent monitoring in gas outflow line are useful
- Volatile agent preconditioning: isoflurane/sevoflurane protect against ischaemia-reperfusion injury (reduce infarct size)
- Muscle relaxants: non-depolarising (pancuronium, rocuronium); avoid succinylcholine after CPB (hyperkalaemia risk with rhabdomyolysis)
12. Special Populations
Paediatric CPB
- Circuit volume is ~3× infant's blood volume → blood priming required
- Higher flow rates: up to 200 mL/kg/min
- MAP lower: 20–50 mmHg acceptable
- DHCA used for complex congenital repairs
- pH-stat preferred for neurological protection during DHCA
- Modified ultrafiltration (MUF) post-bypass: removes inflammatory cytokines, reduces oedema
- Intense inflammatory response → corticosteroids given prophylactically
- Ca²⁺ replacement more important (impaired calcium homeostasis in young children)
HIT (Heparin-Induced Thrombocytopaenia)
- Absolute contraindication to heparin
- Alternatives: bivalirudin (direct thrombin inhibitor; preferred for CPB), argatroban
- Monitor: ACT or ecarin clotting time
13. High-Yield Exam Facts
| Fact | Value |
|---|---|
| ACT target before CPB | > 400–480 s |
| Normal ACT | < 130 s |
| Heparin dose | 300–400 units/kg |
| Protamine dose | ~1 mg/100 units heparin |
| Circuit prime volume (adult) | 1200–1800 mL |
| Hct after prime | 22–27% |
| Target pump flow | 2.2–2.4 L/min/m² |
| MAP target on CPB | 50–80 mmHg |
| Safe DHCA time at 15°C | up to 60 minutes |
| PA catheter: withdraw by | 2–3 cm during CPB |
| Cardioplegia K⁺ | 20–40 mEq/L |
Sources:
- Morgan and Mikhail's Clinical Anesthesiology, 7e, Chapter 22 (pp. 811–860)
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e, Chapter 39 (pp. 3281–3360)
- Miller's Anesthesia, 10e, relevant CPB sections
This is a shared conversation. Sign in to Orris to start your own chat.