Inj. Atropine with picture in MD Anaesthesia
Reading File
Finding Sources
Finding Sources
Searching Images
atropine injection pharmacology anaesthesia
Reading File
Reading File
Finding Sources
Searching Images
atropine structure mechanism action anticholinergic muscarinic
Finding Sources
Finding Sources
Searching Images
atropine chemical structure tertiary amine pharmacology drug
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive answer. Here is the full pharmacology of Injection Atropine as covered in MD Anaesthesia textbooks:
Injection Atropine — MD Anaesthesia
Source: Morgan & Mikhail's Clinical Anesthesiology, 7e, Chapter 13: Anticholinergic Drugs
Physical Structure
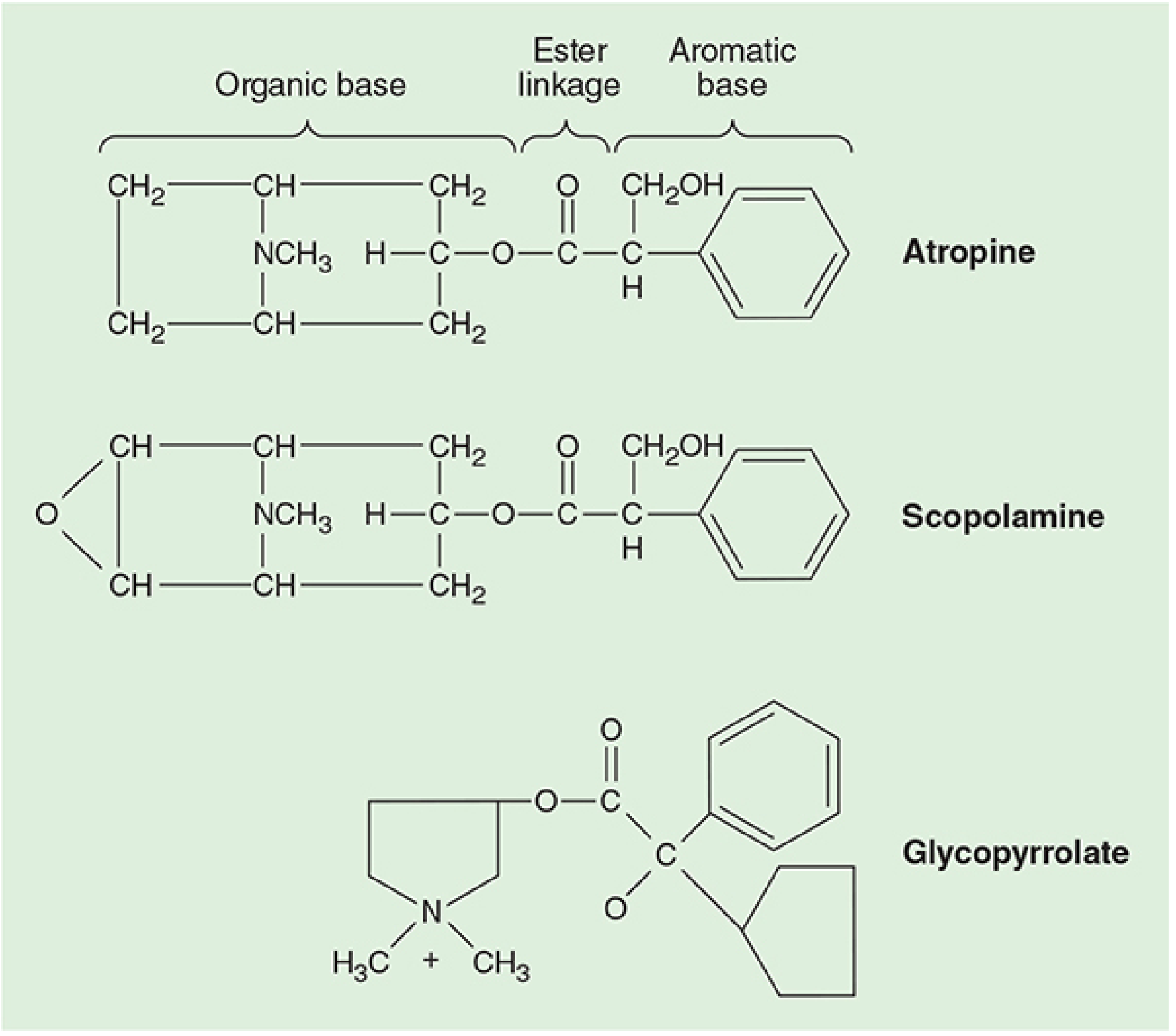
FIGURE 13–1 Physical structures of anticholinergic drugs (Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 431)
Atropine is a tertiary amine — an ester of an aromatic acid combined with an organic base. The ester linkage is essential for effective binding to acetylcholine (muscarinic) receptors. The levorotatory form is pharmacologically active, but the commercial product is a racemic mixture. Because it is a tertiary amine, atropine is lipid-soluble and can cross the blood-brain barrier.
Mechanism of Action
Atropine competitively blocks muscarinic acetylcholine receptors, preventing receptor activation and inhibiting the cellular effects of ACh (mediated through second messengers). Muscarinic receptor subtypes differ in location and affinity:
| Subtype | Location |
|---|---|
| M1 | CNS, autonomic ganglia, gastric parietal cells |
| M2 | Cardiac tissue |
| M3 | Smooth muscle, glands |
The clinical response depends on baseline vagal tone.
Dosage & Packaging
| Indication | Dose |
|---|---|
| Premedication (IM/IV) | 0.01–0.02 mg/kg (adult: 0.4–0.6 mg) |
| Antisialogogue (IM) | 0.01–0.02 mg/kg |
| Severe bradycardia (IV) | Up to 2 mg |
| Pediatric (vagal/bradycardia) | 20 mcg/kg |
Available in multiple concentrations. A 1% solution = 10 mg/mL; one eye drop (~0.05 mL) ≈ 0.5 mg.
Comparative Pharmacology (Table 13–1)
| Effect | Atropine | Scopolamine | Glycopyrrolate |
|---|---|---|---|
| Tachycardia | +++ | + | ++ |
| Bronchodilatation | ++ | + | ++ |
| Sedation | + | +++ | 0 |
| Antisialagogue | ++ | +++ | +++ |
| Crosses BBB | Yes (tertiary) | Yes (tertiary) | No (quaternary) |
0 = no effect; + = minimal; ++ = moderate; +++ = marked
Clinical Pharmacology: Organ System Effects
A. Cardiovascular
- Blockade of M2 receptors at the sinoatrial node → tachycardia
- Most efficacious anticholinergic for treating bradyarrhythmia
- Promotes conduction through the AV node → shortens P-R interval; antagonizes vagal heart block
- ⚠️ Paradoxical bradycardia can occur with small IV doses (<0.4 mg) — mechanism unclear
- Atropine flush: cutaneous vasodilation with large doses
- Caution in coronary artery disease — tachycardia increases myocardial O₂ demand and decreases supply
B. Respiratory
- Inhibits secretions from nose to bronchi → useful during airway procedures
- Relaxes bronchial smooth muscle → reduces airway resistance, increases dead space
- Particularly useful in COPD and asthma patients
- Ipratropium bromide (quaternary derivative) — available as MDI/nebulizer for bronchospasm
C. CNS
- Minimal CNS effects at usual doses despite crossing the BBB
- May cause mild postoperative memory deficits
- Toxic doses: excitatory reactions (agitation, hallucinations, delirium)
- Central anticholinergic syndrome: unconsciousness to hallucinations
D. Gastrointestinal
- Markedly reduces salivation (antisialogogue effect)
- Decreases gastric secretions (larger doses)
- Decreases intestinal motility → prolongs gastric emptying time
- Reduces lower esophageal sphincter pressure
- ⚠️ Does NOT prevent aspiration pneumonia
E. Ophthalmic
- Mydriasis (pupil dilation) and cycloplegia (loss of accommodation)
- ⚠️ Contraindicated/used cautiously in narrow-angle (closed-angle) glaucoma
F. Genitourinary
- May cause urinary retention
- ⚠️ Use cautiously in prostatic hypertrophy or bladder-neck obstruction
Indications in Anaesthesia
- Premedication — antisialogogue before airway procedures or awake intubation
- Bradycardia — most potent anticholinergic for vagal-induced bradycardia (oculocardiac reflex, peritoneal traction, baroreceptor reflex)
- Prevention of succinylcholine-induced bradycardia (especially in children — 20 mcg/kg)
- Strabismus surgery — prevents oculocardiac reflex
- Organophosphate / nerve gas poisoning — reverses muscarinic effects (bronchorrhea, bradycardia); does NOT reverse nicotinic (muscle weakness) effects. Pralidoxime (1–2 g IV) to reactivate AChE.
- Reversal of neuromuscular blockade — given with neostigmine to blunt muscarinic side effects
Overdose / Toxicity
Mnemonic: "Dry as a bone, blind as a bat, red as a beet, hot as a hare, mad as a hatter"
- Dry mouth, tachycardia, atropine flush (red skin), atropine fever, dilated pupils, hallucinations/delirium
- Potentiated by: tricyclic antidepressants, antihistamines, antipsychotics
Antidote: Physostigmine 0.01–0.03 mg/kg IV (tertiary amine → crosses BBB; reverses central anticholinergic toxicity). Neostigmine/pyridostigmine cannot cross BBB and only reverse peripheral effects.
Renal Considerations
Up to 50% of atropine and its active metabolites are excreted in urine. In renal impairment, accumulation is possible with repeated doses.
Morgan & Mikhail's Clinical Anesthesiology, 7e, pp. 430–437 | Barash, Cullen & Stoelting's Clinical Anesthesia, 9e, p. 3724
Make a ppt
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Make a ppt
Reading File
Reading File
Reading File
Running Command
Writing File
Running Command
Your presentation is ready:
Atropine Anaesthesia
Presentation · PPTX
10 slides included:
| # | Slide |
|---|---|
| 1 | Title Slide |
| 2 | Overview & Key Concepts |
| 3 | Physical Structure (with Figure 13-1 chemical diagram) |
| 4 | Dosage & Administration (all clinical doses) |
| 5 | Comparison Table — Atropine vs Scopolamine vs Glycopyrrolate |
| 6 | CVS & Respiratory Effects |
| 7 | CNS, GI, Ophthalmic & GU Effects |
| 8 | Clinical Uses in Anaesthesia (6 key indications) |
| 9 | Contraindications, Toxidrome Mnemonic & Antidote |
| 10 | Summary (8 key takeaways) |
Design uses a navy/teal/gold palette suitable for academic medical presentations, sourced from Morgan & Mikhail's Clinical Anesthesiology, 7e.
Make a comparison poster: Atropine vs Glycopyrrolate
Reading File
Finding Sources
Finding Sources
Reading File
Writing File
Running Command
Your comparison poster is ready:
Atropine vs Glycopyrrolate Poster
Presentation · PPTX
Single wide-format poster slide with a dark navy / blue-green dual-column layout:
| Parameter | Atropine (Blue) | Glycopyrrolate (Green) |
|---|---|---|
| Drug Class | Natural alkaloid | Synthetic quaternary |
| Chemical Structure | Tertiary amine | Quaternary ammonium |
| Crosses BBB | YES ⚠️ | NO ✓ |
| Premedication Dose | 0.01–0.02 mg/kg | 0.005–0.01 mg/kg |
| Duration (IV) | 30 min | 2–4 hours ✓ |
| Tachycardia | +++ | ++ |
| Antisialogogue | ++ | +++ (preferred) |
| Sedation/CNS | + (memory deficits, toxic excitation) | 0 (none) |
| Ophthalmic | Mydriasis + Cycloplegia ⚠️ | Minimal/None ✓ |
| NMB Reversal | With edrophonium | Preferred with neostigmine |
| Key Advantage | Acute vagal bradycardia / OP poisoning | Premedication / safer in elderly & paeds |
Highlighted rows (gold borders) mark the clinically decisive differences. Source: Morgan & Mikhail's Clinical Anesthesiology, 7e, Ch. 13.
Inj.Glycopyrrolate in MD anesthesia..make a ppt
Finding Sources
Finding Sources
Reading File
Reading File
Running Command
Writing File
Running Command
Your presentation is ready:
Glycopyrrolate Anaesthesia
Presentation · PPTX
10 slides — teal/green/gold dark theme:
| # | Slide |
|---|---|
| 1 | Title Slide |
| 2 | Overview & Key Concepts |
| 3 | Physical Structure (with Figure 13-1, Morgan & Mikhail) |
| 4 | Dosage & Administration (6 clinical scenarios) |
| 5 | Comparative Table — Barash Table 14-6 (Atropine vs Scopolamine vs Glycopyrrolate) |
| 6 | Organ System Effects (CVS, Respiratory, CNS, GI/GU) |
| 7 | Clinical Uses in Anaesthesia (6 indications) |
| 8 | Advantages, Special Situations & Drug Pairings |
| 9 | Structural Formulae (Figure 14-15, Barash 9e) |
| 10 | Summary — 10 Key Points |
Key clinical highlights covered:
- Cannot cross BBB — zero CNS/ophthalmic effects (chief advantage)
- Longest acting: 2–4 h IV; 6–8 h IM
- Preferred with neostigmine for NMB reversal
- Spinal bradycardia refractory — atropine/ephedrine preferred
- Dose = ½ atropine (0.005–0.01 mg/kg)
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7e · Barash, Cullen & Stoelting's Clinical Anesthesia, 9e
IV cannula in MD Anaesthesia..make a ppt
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching Images
IV cannula intravenous catheter sizes gauge peripheral venous access
Reading File
Finding Sources
Finding Sources
Running Command
Writing File
Running Command
Your presentation is ready:
IV Cannula Anaesthesia
Presentation · PPTX
10 slides — navy/blue/gold theme:
| # | Slide |
|---|---|
| 1 | Title Slide |
| 2 | Overview & Definition (Poiseuille's Law, indications) |
| 3 | Gauge Sizes & Colour Coding Table (14G–24G, flow rates, clinical use, patient groups) |
| 4 | Parts of a Cannula + Equipment Needed |
| 5 | Site Selection (6 sites: pros, cons, preferred use) |
| 6 | Insertion Technique — Step by Step (6 steps) |
| 7 | Difficult IV Access & Ultrasound Guidance (with US image) |
| 8 | Complications (9 complications with management) |
| 9 | Anaesthesia-Specific Considerations (gauge by case type, intraoperative care, documentation) |
| 10 | Summary — 10 Key Points |
Key highlights:
- Colour-coded gauge table with flow rates (14G orange → 24G yellow)
- Poiseuille's Law explained clinically
- Mandatory IV access before induction rule
- Gauge selection guide by surgery type
- All 9 complications covered with management
Scopolamoine and hyosine in MD Anaesthesia...short and sweet ppt
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.