Hypospadis and epispadias
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Hypospadias and Epispadias
HYPOSPADIAS
Definition and Incidence
Hypospadias is a congenital anomaly in which the external urethral meatus opens on the ventral (under) surface of the penis, proximal to its normal position at the tip of the glans. It is the most common congenital abnormality of the urethra, occurring in approximately 1 in 125-300 male live births.
(The Developing Human - Clinically Oriented Embryology; Schwartz's Principles of Surgery 11e; Bailey & Love 28e)
The Classic Triad of Features
- Ectopic ventral urethral meatus - the hallmark
- Ventral penile curvature (chordee) - more pronounced in severe types
- Incomplete dorsal hood prepuce - foreskin is deficient ventrally, giving a "hooded" appearance
Classification (by meatal position)
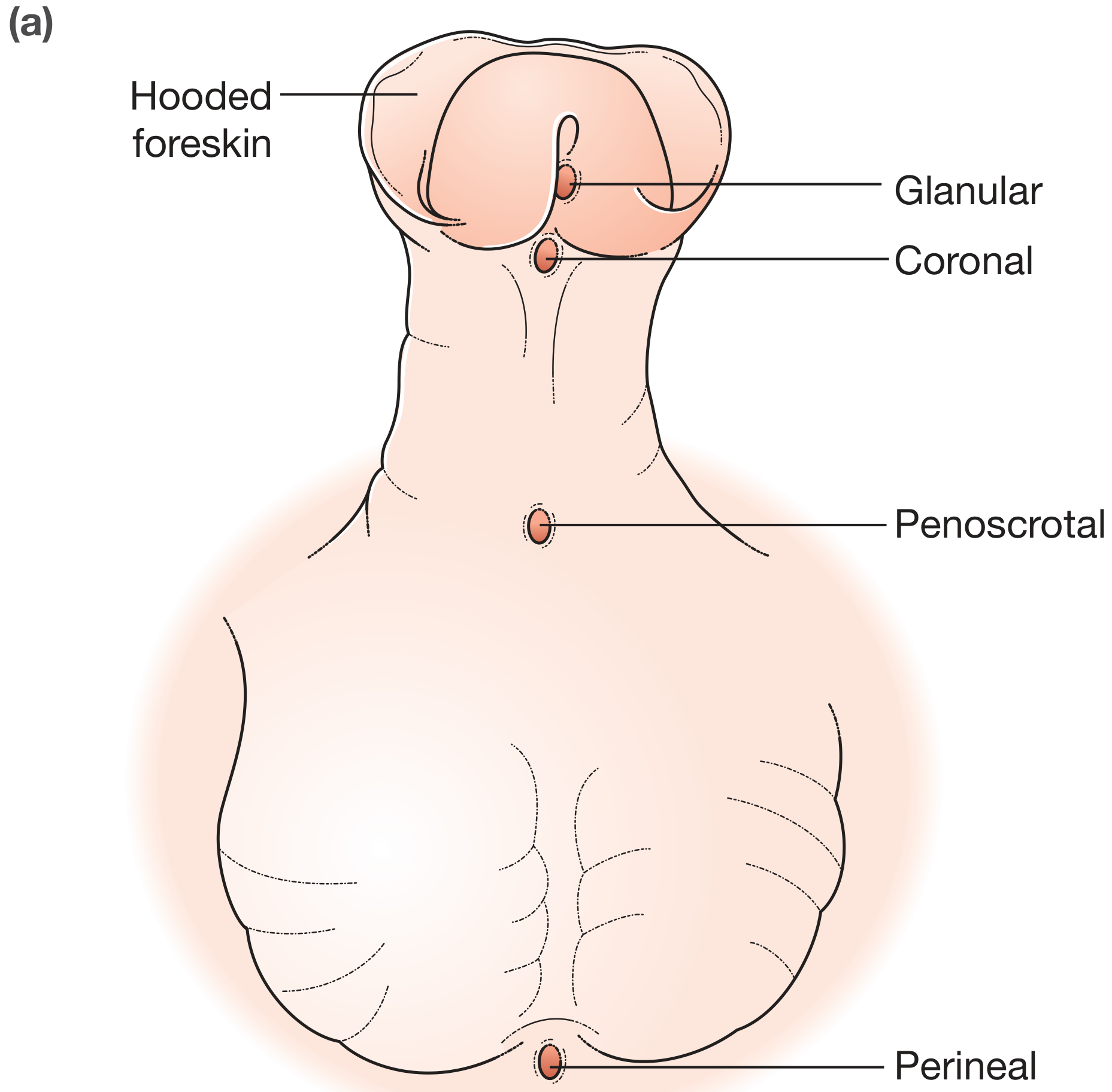
| Type | Meatal position | Notes |
|---|---|---|
| Glanular | On the ventral surface of the glans, proximal to the blind pit at the normal meatus | Most common type; a blind pit marks where the meatus should be |
| Coronal | At the level of the coronal sulcus | - |
| Penile (shaft) | On the ventral surface of the penile shaft | - |
| Penoscrotal | At the penoscrotal junction | - |
| Perineal | Between the unfused halves of a bifid scrotum | Rarest and most severe |
Distal types (glanular + coronal + distal penile) account for ~70-80% of all cases.
In perineal hypospadias, the external genitalia can appear ambiguous; when combined with cryptorchidism, it can be mistaken for XY gonadal dysgenesis.
Embryology and Pathogenesis
Hypospadias results from incomplete formation of the spongy urethra due to:
- Failure of canalization of the ectodermal cord in the glans penis
- Failure of fusion of the urethral folds on the ventral penile shaft
- Root cause: inadequate androgen production by the fetal testes and/or inadequate androgen receptor function
- Both genomic and environmental factors are implicated; expression of testosterone-related genes is affected
(The Developing Human - Clinically Oriented Embryology)
Clinical photo - Glanular hypospadias in an infant

Associated Anomalies
- Cryptorchidism (undescended testes) - particularly relevant with proximal hypospadias
- When proximal hypospadias coexists with a nonpalpable testis, Disorder of Sexual Development (DSD) must be excluded (requires hormonal studies, karyotype, pelvic ultrasound)
- Micropenis
No increased risk of renal or bladder anomalies in isolated distal hypospadias, so upper tract imaging is not routinely needed.
Management
Avoid circumcision - the prepuce is potentially needed for future reconstructive surgery.
Timing: Surgery is best performed before 18 months of age.
| Severity | Approach |
|---|---|
| Distal hypospadias | Single-stage repair; Tubularized Incised Plate (TIP/Snodgrass) urethroplasty is the standard; success rate >95% |
| Proximal hypospadias with chordee | Usually a two-stage repair: Stage 1 corrects penile curvature (chordee excision); Stage 2 reconstructs the urethra |
Surgery should be performed by experts in hypospadias surgery.
Complication of failed repair: Urethrocutaneous fistula is the most common.
(Bailey & Love 28e; Schwartz's Principles of Surgery 11e; Campbell-Walsh-Wein Urology)
Long-term Outcomes
- Postvoid dribbling: 20-40%
- Urinary stream spraying: 40-50%
- Erectile dysfunction: ~25%
- Ejaculatory dysfunction: ~37%
- Infertility (isolated hypospadias): ~13%
- Adults with corrected hypospadias generally have normal sexual function and fertility
(Campbell-Walsh-Wein Urology)
EPISPADIAS
Definition and Incidence
Epispadias is a congenital anomaly in which the urethra opens on the dorsal (upper) surface of the penis - the opposite of hypospadias. It is far rarer: 1 in 30,000 male infants and 1 in 450,000 females.
(Smith & Tanagho's General Urology 19e; The Developing Human)
Embryology and Pathogenesis
Epispadias results from inadequate ectodermal-mesenchymal interactions during development of the genital tubercle. The genital tubercle develops more dorsally than normal, so when the urogenital membrane ruptures, the urogenital sinus opens on the dorsal surface rather than the tip. Urine is consequently expelled at the root of the malformed penis.
Epispadias is considered a mild form of bladder exstrophy and frequently coexists with it.
(The Developing Human - Clinically Oriented Embryology)
Classification in Males (by meatal position)
| Type | Location | Incontinence |
|---|---|---|
| Glandular | Dorsal aspect of the glans (broad, flattened); distal groove extends to the glans | Rarely incontinent |
| Penile | Between pubic symphysis and coronal sulcus; meatus broad and gaping | ~75% incontinent |
| Penopubic | At the penopubic junction; entire dorsum has a groove through the glans | ~95% incontinent |
In Females
- Bifid clitoris and separation of the labia
- Most females with epispadias are incontinent
Key Features
- Dorsal chordee - upward curvature of the erect penis (opposite to hypospadias where it is ventral)
- Separation of the pubic bones - as in exstrophy of the bladder
- Urinary incontinence - due to maldevelopment of urinary sphincters; common in penile and penopubic types
- Strong association with bladder exstrophy (the exstrophy-epispadias complex)
Management
Surgery is required to:
- Correct incontinence (repair urinary sphincter - though this has not been very successful; bladder augmentation + artificial sphincter may be required)
- Excise dorsal chordee to straighten the penis
- Extend the urethra out onto the glans (urethroplasty with meatal advancement)
(Smith & Tanagho's General Urology 19e; Bailey & Love 28e)
Quick Comparison Table
| Feature | Hypospadias | Epispadias |
|---|---|---|
| Meatal position | Ventral surface | Dorsal surface |
| Chordee type | Ventral (downward) curve | Dorsal (upward) curve |
| Incidence (males) | 1 in 125-300 | 1 in 30,000 |
| Common association | Cryptorchidism, DSD | Bladder exstrophy |
| Incontinence | Rare (unless perineal) | Common (penile/penopubic) |
| Prepuce | Hooded (deficient ventrally) | Deficient dorsally |
| Embryological failure | Urethral fold fusion + ectodermal canalization | Genital tubercle develops too dorsally |
| Key surgery | TIP urethroplasty (Snodgrass) | Chordee excision + urethroplasty + sphincter repair |
Sources: Bailey & Love's Short Practice of Surgery 28e | Smith & Tanagho's General Urology 19e | The Developing Human - Clinically Oriented Embryology | Schwartz's Principles of Surgery 11e | Campbell-Walsh-Wein Urology
This is a shared conversation. Sign in to Orris to start your own chat.