Explain portal hypertension, pathophysiology and causes of portal hypertension , investigation , clinical featurea and management of portal htn .
"portal hypertension" management
Portal Hypertension - Comprehensive Overview
Definition
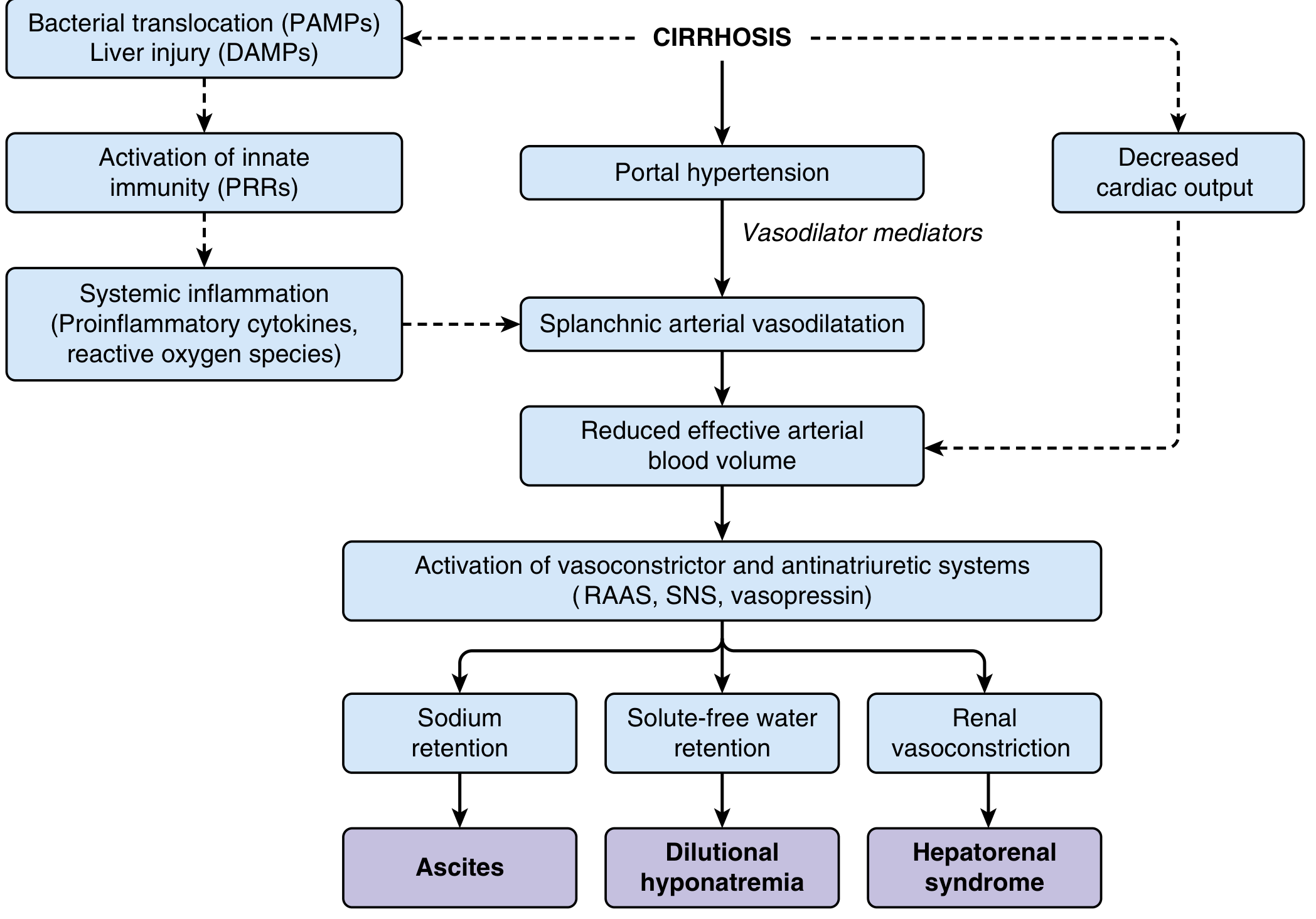
Pathophysiology
1. Increased Intrahepatic Resistance to Portal Flow
- Structural/passive component: Progressive collagen deposition and nodule formation cause architectural distortion of sinusoidal blood flow, increasing intrahepatic vascular resistance
- Dynamic/functional component: Contraction of hepatic stellate cells (HSCs) and vascular smooth muscle cells/myofibroblasts; disruption of blood flow by scarring
- Decreased nitric oxide (NO) production - reduces vasodilation
- Increased endothelin-1 release - causes vasoconstriction
- Increased angiotensinogen and eicosanoids - further vasoconstriction
- Sinusoidal remodeling creates anastomoses between arterial and portal systems in fibrous septa, imposing arterial pressures on the low-pressure portal system
2. Hyperdynamic Splanchnic Circulation (Increased Portal Inflow)
- Splanchnic arterial vasodilation (mediated primarily by NO overproduction, also prostacyclin and TNF-alpha) increases mesenteric blood flow
- This increased splanchnic blood flow leads to increased venous efflux into the portal system
- Effective arterial hypovolemia triggers RAAS and sympathetic nervous system activation - causing sodium retention, contributing to ascites formation
- The result is a high portal flow state that cannot be decompressed by the high-resistance intrahepatic circulation
Causes / Etiology
Pre-Sinusoidal
- Portal vein thrombosis (obstructive/compressive)
- Splenic vein thrombosis (pancreatitis, pancreatic tumor)
- Massive splenomegaly with increased splenic blood flow
- Tropical splenomegaly
- Arterioportal fistula
- Myelofibrosis / myeloproliferative disorders
- Schistosomiasis (periportal fibrosis - eggs lodge in portal tracts)
- Congenital hepatic fibrosis
- Nodular regenerative hyperplasia
- Idiopathic portal fibrosis
- Sarcoidosis / diffuse fibrosing granulomatous disease
- Primary biliary cholangitis (even before cirrhosis develops)
- Graft-versus-host disease
Sinusoidal (Intrahepatic)
- Cirrhosis from any cause - the most common cause overall (accounts for ~90% of cases)
- Alcohol abuse
- Chronic viral hepatitis (HBV, HCV)
- NAFLD/NASH
- Autoimmune hepatitis
- Primary sclerosing cholangitis
- Metabolic disorders (Wilson's, hemochromatosis, alpha-1 antitrypsin deficiency)
- Massive fatty change (steatosis)
- Infiltrative malignancy (primary or metastatic)
- Amyloidosis
Post-Sinusoidal
- Hepatic veno-occlusive disease (sinusoidal obstruction syndrome)
- Budd-Chiari syndrome (hepatic vein outflow obstruction)
- Severe right-sided heart failure
- Constrictive pericarditis
- Inferior vena caval web/membrane
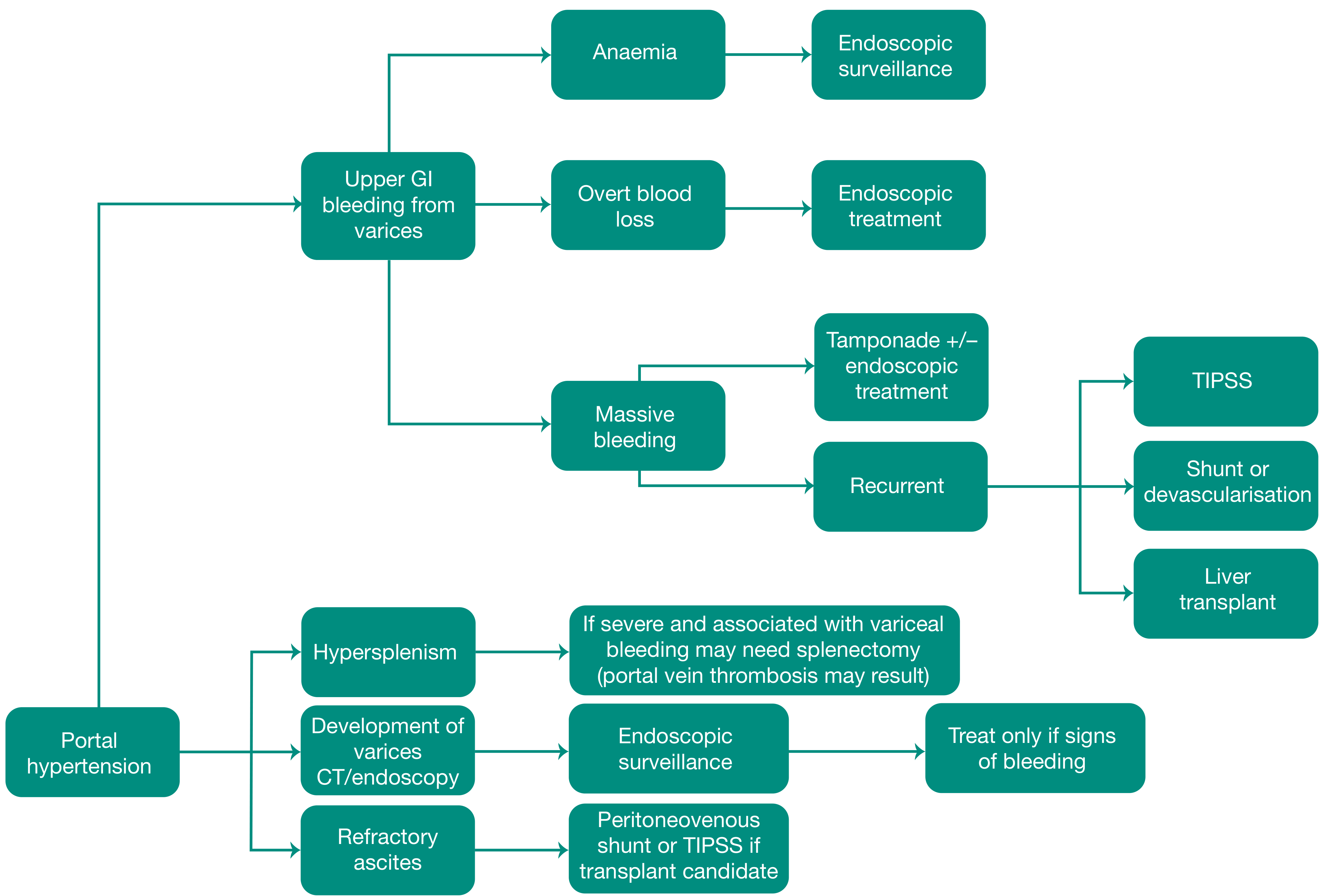
Clinical Features
1. Portosystemic Venous Shunts / Varices
| Site | Clinical Manifestation |
|---|---|
| Esophagogastric junction | Esophageal and gastric varices (most important) |
| Around/within rectum | Anorectal varices (present in ~45% of cirrhotics; distinguished from hemorrhoids) |
| Abdominal wall/falciform ligament | Caput medusae (dilated subcutaneous veins radiating from umbilicus) |
| Retroperitoneum | Retroperitoneal collaterals |
| Umbilical vein | Recanalized umbilical vein |
- Esophageal varices appear in ~40% of patients with advanced cirrhosis
- They cause massive hematemesis and death in about half of those affected
- Each bleeding episode carries approximately 20-30% mortality
- Failure to control variceal bleeding occurs in 10-20% of cases with current medical management
- 70% of survivors of an initial bleed experience recurrent hemorrhage within 2 years if untreated
2. Ascites
- Accumulation of fluid in the peritoneal cavity
- Results from a combination of portal hypertension AND hepatocyte dysfunction
- Mechanism: splanchnic vasodilation → effective arterial hypovolemia → RAAS + SNS activation → renal sodium/water retention
- Abdominal distension, dragging discomfort, shifting dullness, fluid thrill
- Serum-Ascites Albumin Gradient (SAAG) >1.1 g/dL indicates portal hypertension as the cause
3. Splenomegaly / Hypersplenism
- Congestive splenomegaly - splenic weight can reach up to 1000 g (5-6x normal)
- Hypersplenism causes sequestration of blood elements:
- Thrombocytopenia (most common)
- Leukopenia
- Anemia / pancytopenia
4. Hepatic Encephalopathy
- Due to portosystemic shunting - ammonia and other toxins bypass hepatic detoxification
- Ranges from subtle cognitive changes to coma
- Often precipitated by GI bleed, infection, electrolyte disturbance, or excessive protein intake
Additional Clinical Features
- Jaundice (in hepatic causes)
- Spider naevi, palmar erythema, gynecomastia (in cirrhosis)
- Fetor hepaticus
- Hepatopulmonary syndrome: intrapulmonary vascular dilation causing V/Q mismatch, hypoxemia worse in upright position (present in up to 30% of cirrhotics)
- Portopulmonary hypertension: pulmonary arterial hypertension with dyspnea on exertion and clubbing
Investigations
Blood Tests
| Investigation | Finding in Portal HTN |
|---|---|
| FBC | Thrombocytopenia, leukopenia (hypersplenism), anemia |
| LFTs | Raised bilirubin, low albumin, elevated transaminases |
| Coagulation | Prolonged PT/INR (reduced hepatic synthetic function) |
| Renal function | Hyponatremia, creatinine rise (hepatorenal syndrome risk) |
| Viral serology | HBsAg, anti-HCV (etiology) |
Imaging
- Abdominal Ultrasound (first line): Large portal vein (>13 mm) suggests portal hypertension. Detects cirrhotic nodular liver, splenomegaly, ascites, direction of portal flow
- Doppler Ultrasound: Outlines portal vein anatomy, excludes thrombosis, identifies direction of portal blood flow, evaluates flow through surgical shunts and TIPS
- CT Abdomen (with contrast): Confirms ascites etiology, demonstrates irregular shrunken cirrhotic liver, portal hypertension, splenomegaly, abdominal varices, and portal vein patency. Portal vein occlusion is a common finding
- MR Angiography: Non-invasive portal vein anatomy and patency
- Visceral Angiography / Portal Venography: Reserved for cases where non-invasive methods are insufficient; needed for shunt planning
Endoscopy
- Upper GI Endoscopy (OGD): Gold standard for diagnosis and grading of esophageal and gastric varices; ~30% of patients suspected of variceal bleeding have a non-variceal source, so endoscopy is essential
Measurement of Portal Pressure - HVPG
- Hepatic venography with a balloon catheter placed in the hepatic vein
- WHVP (Wedged Hepatic Venous Pressure) measured with balloon inflated
- FHVP (Free Hepatic Venous Pressure) measured with balloon deflated
- HVPG = WHVP - FHVP
- HVPG >10 mmHg = clinically significant portal hypertension
- HVPG >12 mmHg = risk of variceal bleeding
Ascitic Fluid Analysis (Diagnostic Paracentesis)
- SAAG >1.1 g/dL = portal hypertension (sensitivity ~97%)
- Protein content (exclude cardiac/exudative causes)
- Culture & microscopy (exclude SBP)
- Cytology (exclude malignancy)
- Amylase (exclude pancreatic ascites)
Management
A. Prevention of First Variceal Bleed (Primary Prophylaxis)
- Non-selective beta-blockers (propranolol, nadolol, carvedilol):
- Reduce index variceal bleed by ~45% and bleeding mortality by ~50%
- ~20% of patients don't respond; another ~20% cannot tolerate
- Endoscopic Variceal Band Ligation (EVBL):
- Recommended for medium to large varices
- Performed every 1-2 weeks until obliteration
- Then OGD 1-3 months later, followed by surveillance OGD every 6 months
B. Management of Acute Variceal Hemorrhage
Resuscitation (immediate)
- ICU admission
- Two large-bore IV cannulae; blood resuscitation to Hb ~8 g/dL (avoid hypervolemia - raises portal pressure)
- Terlipressin (splanchnic vasoconstrictor) - first-line pharmacological agent; also octreotide or somatostatin
- Prophylactic antibiotics (norfloxacin or IV ceftriaxone) - reduce risk of bacterial infection and improve survival
- 10 mg IV Vitamin K; FFP and platelets if severe coagulopathy; platelets if <50 x 10⁹/L
- Consider endotracheal intubation to protect airway (risk of aspiration, especially if encephalopathic)
Endoscopic Treatment
- Urgent OGD once haemodynamically stable (confirms source - 30% non-variceal)
- Esophageal varices: Sclerotherapy or Band Ligation (preferred)
- Gastric/fundal varices: Cyanoacrylate (tissue adhesive glue) injection; thrombin
Balloon Tamponade
- Sengstaken-Blakemore tube (gastric + esophageal balloon) or Minnesota tube (additional aspiration port)
- Reserved for massive/refractory bleeding as a "bridge" to definitive treatment
- Self-expanding covered metal esophageal stents are emerging as an alternative
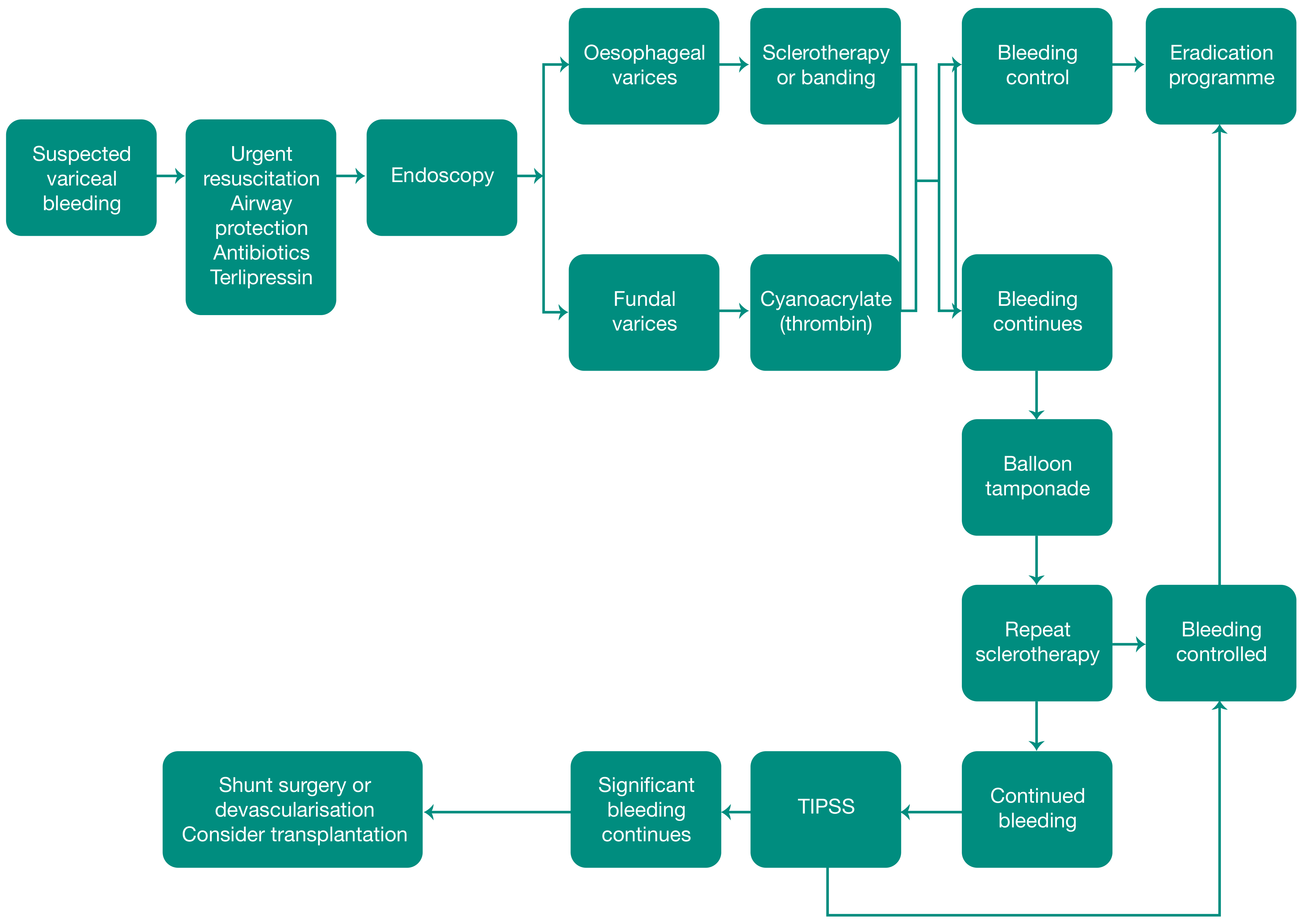
TIPS / TIPSS (Transjugular Intrahepatic Portosystemic Shunt/Stent)
- Indicated when endoscopic treatment fails (10-20% of cases) or for refractory/recurrent bleeding
- Transjugular catheter passed through hepatic parenchyma into a portal vein branch; metallic stent creates a portovenous channel
- Effectively decompresses portal system
- Main early complication: liver capsule perforation with intraperitoneal hemorrhage
- Stent occlusion occurs in 50% at 1 year
- Post-TIPS encephalopathy rate ~40% (portal blood bypasses hepatic detoxification)
- Contraindicated in portal vein occlusion
C. Secondary Prophylaxis (Prevention of Rebleed)
- Combination of non-selective beta-blockers + repeat endoscopic band ligation is standard
- TIPS if medical/endoscopic therapy fails
- Liver transplantation for eligible patients
D. Management of Ascites
| Step | Treatment |
|---|---|
| 1st line | Salt restriction + Spironolactone (aldosterone antagonist) ± Furosemide |
| Monitoring | Regular biochemical monitoring on diuretics |
| Refractory ascites | Large-volume paracentesis (with albumin replacement) |
| Bridge/rescue | TIPS or peritoneovenous shunts |
| Definitive | Liver transplantation |
E. Surgical Portosystemic Shunts
- Total shunts: Portocaval, mesocaval
- Selective shunts: Distal splenorenal (Warren) shunt - decompresses varices while preserving hepatic perfusion
- Devascularisation procedures: Sugiura procedure (esophageal transection + devascularization)
F. Splenectomy
- Considered if hypersplenism is severe and associated with variceal bleeding
- Risk: portal vein thrombosis may result post-splenectomy
G. Liver Transplantation
- Definitive treatment for portal hypertension secondary to cirrhosis
- Addresses both the portal hypertension and the underlying liver disease
- Indicated for refractory/recurrent variceal bleeding, refractory ascites, and end-stage liver disease
Summary Table: Key Numbers to Remember
| Parameter | Value |
|---|---|
| Normal portal pressure | 5-10 mmHg |
| Clinically significant portal HTN (HVPG) | >10 mmHg |
| Risk of variceal bleeding (HVPG) | >12 mmHg |
| Esophageal varices in advanced cirrhosis | ~40% |
| Mortality per variceal bleed episode | 20-30% |
| Rebleed rate if untreated at 2 years | ~70% |
| Failure to control variceal bleeding | 10-20% |
| Post-TIPS encephalopathy | ~40% |
| TIPS stent occlusion at 1 year | ~50% |
| SAAG threshold for portal HTN ascites | >1.1 g/dL |
Gastrinoma
"gastrinoma" AND "Zollinger-Ellison"
Gastrinoma (Zollinger-Ellison Syndrome)
Definition
Pathophysiology
- The tumor does not respond to normal physiological stimuli (amino acids, gastric distension) and is not subject to feedback inhibition by low luminal pH
- Critically, gastrinoma is stimulated (rather than inhibited) by secretin - the basis of the secretin stimulation test
- Unregulated, massive gastrin secretion leads to:
- Continuous maximal parietal cell stimulation → profound acid hypersecretion
- Parietal cell hyperplasia (increased parietal cell mass) - this can persist for months after resection
- Acid overwhelms the duodenal and jejunal mucosa → multiple ulcers in atypical locations
- High duodenal acid inactivates pancreatic lipase and precipitates bile salts → steatorrhea and diarrhea
- Large gastric rugal folds (hypertrophy from trophic effect of gastrin)
Location - The Gastrinoma Triangle (Passaro's Triangle)
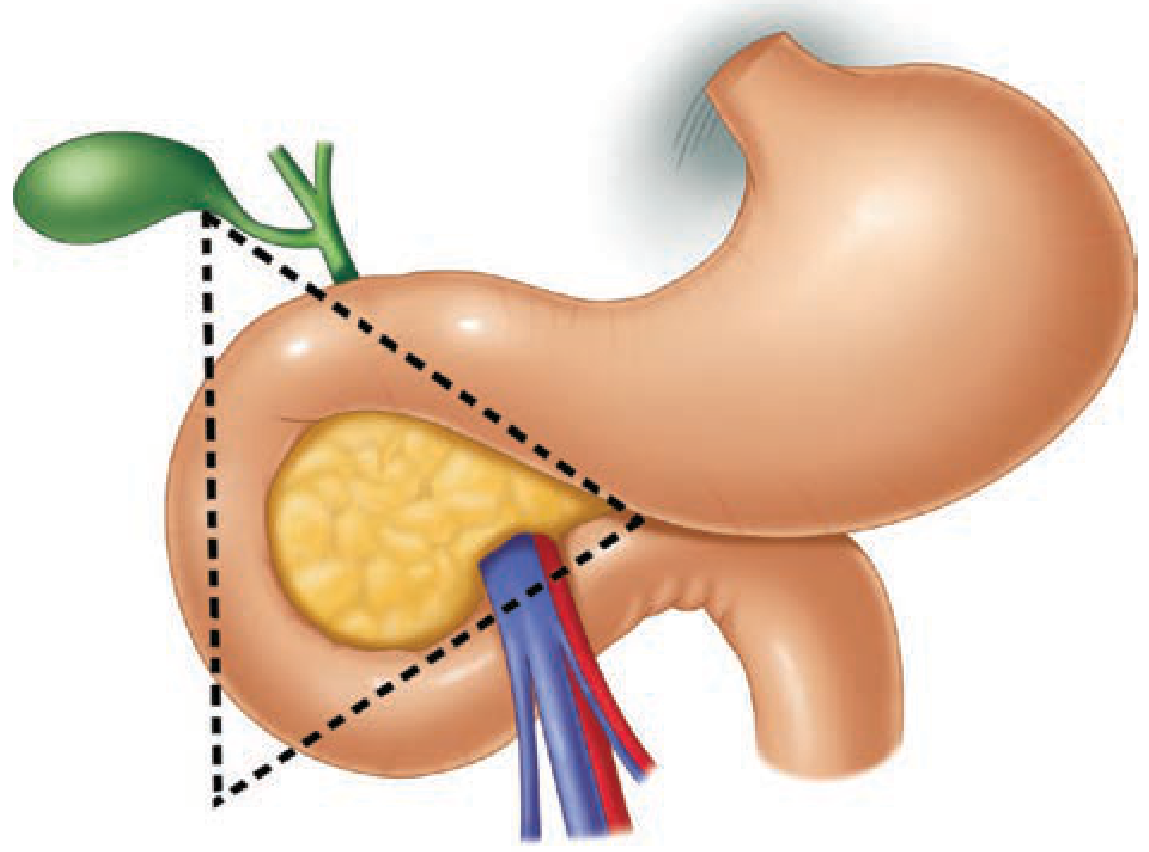
- Superiorly - junction of the cystic duct and common bile duct
- Inferiorly - junction of the 2nd and 3rd portions of the duodenum
- Medially - junction of the neck and body of the pancreas
- Duodenum: 50-90% of sporadic ZES gastrinomas (particularly the proximal duodenum); typically small (<1 cm) and rarely metastasize
- Pancreas: Usually right of the superior mesenteric vessels; typically larger and more often metastasize
- Rare ectopic sites: stomach, liver, gallbladder, mesentery, ovary
Association with MEN-1
- 20-25% of ZES cases are associated with MEN-1 (Multiple Endocrine Neoplasia Type 1)
- MEN-1 = parathyroid hyperplasia + pituitary tumors + pancreatic NETs
- In MEN-1, gastrinomas are usually multiple, small, and extrapancreatic (mainly duodenal)
- Hyperparathyroidism (first manifestation of MEN-1) must be treated first - hypercalcemia stimulates ectopic gastrin secretion and worsens ZES
- All ZES patients should be screened for MEN-1 (serum calcium, PTH, family history); genetic testing if hypercalcemia, concurrent MEN-1 tumor, or family history
Clinical Features
Symptoms
| Feature | Details |
|---|---|
| Abdominal pain | Most common; due to peptic ulceration |
| Peptic ulcer disease | 90% of ZES patients have peptic ulcers; most in duodenal bulb, with synchronous ulcers in distal duodenum or proximal jejunum - a classic "atypical location" |
| Diarrhea | In 21-40% at diagnosis; watery, large volume; caused by high acid inactivating pancreatic enzymes; relieved by nasogastric suction (distinguishing feature) |
| GERD / esophagitis | Common; severe, sometimes with stricture |
| Steatorrhea | Acid inactivates lipase, precipitates bile salts |
| GI bleeding | Hematemesis, melena, or hematochezia |
| Nausea and vomiting | |
| Weight loss |
Endoscopic Findings
- Multiple ulcers (especially in unusual locations - distal duodenum, jejunum)
- Large, thickened gastric rugal folds (from gastrin's trophic effect)
- Edema of duodenal mucosa
- Jejunal hypermotility
When to Suspect ZES
- Ulcers refractory to standard therapy
- Ulcers in atypical locations (distal duodenum, jejunum)
- Multiple simultaneous ulcers
- Peptic ulcer + diarrhea
- Strong family history of peptic ulcer disease or MEN-1
- Recurrence of ulcers after acid-reducing surgery
Investigations
Step 1: Biochemical Diagnosis
Fasting Serum Gastrin (FSG) - Key Test
- Must stop PPIs (3 weeks before) and H2 blockers (1 week before) before testing - these cause spurious elevation
- Normal: <100 pg/mL
- Suspicious: >300 pg/mL
- >1000 pg/mL with gastric pH <2 = DIAGNOSTIC for gastrinoma
- Usual range in ZES: 200-1000 pg/mL
Causes of Hypergastrinemia (Differential Diagnosis)
| High Gastric Acid Output | Low Gastric Acid Output |
|---|---|
| Gastrinoma (ZES) | PPI / H2 blocker therapy |
| Gastric outlet obstruction | Atrophic gastritis |
| G-cell hyperplasia | Pernicious anemia |
| Retained gastric antrum | Achlorhydria |
| Chronic renal failure | |
| Previous vagotomy |
Secretin Stimulation Test - Confirmatory (equivocal gastrin levels)
- Administer IV secretin 2 IU/kg
- In ZES: paradoxical rise in serum gastrin >200 pg/mL (since gastrinoma is stimulated by secretin, not inhibited)
- In normal physiology and other causes: secretin suppresses gastrin
- Sensitivity ~85%, specificity >95%
Basal Acid Output (BAO)
- ZES: BAO typically >15 mEq/h (normal ~5 mEq/h; patients without stomach acid or previous vagotomy have near-zero BAO)
Step 2: Tumor Localization
| Modality | Key Points |
|---|---|
| ⁶⁸Ga-DOTATATE PET/CT | First-line; best sensitivity for primary and metastatic disease; particularly useful as somatostatin receptor expression is high |
| Octreotide (SSTR) scintigraphy | Detects ~85% of gastrinomas; can detect tumors <1 cm; combined with CT detects most gastrinomas |
| CT/MRI (cross-sectional imaging) | Standard staging; detects liver metastases; CT less sensitive for small duodenal tumors |
| Endoscopic Ultrasound (EUS) | Most sensitive for pancreatic head and duodenal wall tumors (often <1 cm); highly useful pre-operatively |
| Combination octreotide scan + EUS | Detects >90% of gastrinomas |
| Selective angiography / portal venous sampling | Reserved for cases where other modalities fail; technically demanding |
| Intraoperative ultrasound (IOUS) | Used during surgery to identify occult tumors |
Malignancy
- Over 60% of gastrinomas are malignant (defined by presence of lymph node or distant metastases)
- 50% metastasize to lymph nodes or liver at diagnosis
- 70-80% of malignant gastrinomas have metastases (liver or lymph nodes) at time of diagnosis
- Metastatic sites: liver (most common), peripancreatic lymph nodes, lung, bone
- Serum gastrin levels mirror disease extent - highest in locally advanced or metastatic disease
- Pancreatic gastrinomas are larger and more often have lymph node metastases than duodenal ones
- Liver metastases reduce survival; lymph node metastases alone do NOT adversely affect survival
Management
1. Medical Management - Control of Acid Hypersecretion
- Omeprazole, lansoprazole, pantoprazole
- Goal: Reduce Basal Acid Output (BAO) to <10 mEq/h (or <5 mEq/h in patients with prior acid-reducing surgery or severe GERD)
- PPIs are highly effective and are the initial treatment of choice
- Somatostatin analogues (octreotide/lanreotide) may help control symptoms in refractory cases
- H2 receptor antagonists (cimetidine, ranitidine) may be added in some patients
2. Surgical Management
Preoperative Assessment
- Rule out MEN-1 (check serum calcium, PTH) - gastrinoma resection in MEN-1 rarely normalizes serum gastrin; parathyroidectomy should precede or accompany gastrinoma surgery in MEN-1
- Full tumor localization with imaging
- Achieve acid control with PPIs prior to surgery
Intraoperative Steps
- Thorough exploration of Passaro's triangle
- Intraoperative ultrasound (IOUS) to locate occult tumors
- Duodenotomy - mandatory; palpation alone misses small submucous duodenal tumors; full-thickness excision of duodenal wall for duodenal gastrinomas
- Lymph node dissection - all lymph nodes in Passaro's triangle excised for pathological analysis
- Enucleation for pancreatic gastrinomas not involving the main pancreatic duct
- Formal pancreatectomy (pancreaticoduodenectomy or distal pancreatectomy) for solitary pancreatic gastrinomas with no metastases
- Highly selective vagotomy if unresectable disease is found or tumor cannot be localized (reduces PPI requirement)
MEN-1 and Surgery
- Tumors are typically multiple and small; surgery rarely achieves biochemical cure (~5% disease-free at 5 years vs. 40% in sporadic)
- Most specialists recommend non-surgical management for MEN-1 gastrinomas, except:
- Duodenal gastrinomas (respond better to surgery)
- Tumors >2-2.5 cm (higher metastasis risk, surgery improves survival)
- In MEN-1: treat hyperparathyroidism first (parathyroidectomy + forearm implant)
Hepatic Metastases
- Resection is justified if primary is controlled AND metastases can be safely, completely removed
- Debulking of multiple hepatic metastases is generally not helpful (especially in MEN-1)
- Other liver-directed therapies: radiofrequency ablation, hepatic artery embolization/chemoembolization, SIRT (selective internal radiation therapy)
3. Treatment of Metastatic / Unresectable Disease
| Treatment | Use |
|---|---|
| Somatostatin analogues (octreotide, lanreotide) | Symptom control; antiproliferative effect |
| Peptide receptor radionuclide therapy (PRRT) | e.g., ⁱ⁷⁷Lu-DOTATATE; growing role |
| Chemotherapy | Streptozotocin + 5-FU ± doxorubicin |
| mTOR inhibitors / tyrosine kinase inhibitors | Everolimus, sunitinib |
| Interferon-alpha | Some success |
| Hepatic artery embolization | Liver-dominant disease |
Prognosis
| Scenario | Survival |
|---|---|
| No liver metastases | 15-year survival ~80% |
| Liver metastases present | 5-year survival 20-50% |
| MEN-1 with gastrinoma <2.5 cm (no metastases) | 100% at 15 years |
| MEN-1 with metastatic disease | 52% at 15 years |
| Biochemical cure after surgery (sporadic) | ~30-40% |
| Biochemical cure after surgery (MEN-1) | ~5-15% (short-term); ~5% at 5 years |
- Best prognosis: Complete excision of small, sporadic, duodenal tumors
- Worst prognosis: Large tumors with liver metastases outside Passaro's triangle
- Lymph node metastases alone do not reduce long-term survival
Key Summary Points
| Feature | Detail |
|---|---|
| Tumor type | Gastrin-secreting NET |
| Syndrome produced | Zollinger-Ellison Syndrome (ZES) |
| Most common location | Proximal duodenum (50-90% in sporadic ZES) |
| Location rule | 80-90% in Passaro's (gastrinoma) triangle |
| MEN-1 association | 20-25% of ZES cases |
| Malignancy rate | >60% |
| Diagnostic gastrin level | >1000 pg/mL with pH <2 |
| Confirmatory test | Secretin stimulation test (paradoxical gastrin rise >200 pg/mL) |
| Best imaging | ⁶⁸Ga-DOTATATE PET/CT + EUS |
| Drug of choice | PPI (omeprazole/lansoprazole) |
| Curative treatment | Surgery (for sporadic, resectable disease) |
| Secretin response | Stimulates gastrin (paradoxical - not inhibited) |
Gastrinoma
Gastrinoma (Zollinger-Ellison Syndrome) - Quick Reference
What It Is
- Gastrin-secreting neuroendocrine tumor (NET) of duodenum/pancreas
- Causes Zollinger-Ellison Syndrome (ZES) - severe acid hypersecretion + peptic ulceration
- 2nd most common functional pancreatic NET; incidence ~1/2.5 million
Key Facts at a Glance
| Feature | Value |
|---|---|
| Most common site | Proximal duodenum (50-90% in sporadic ZES) |
| Location rule | 80-90% within Passaro's (gastrinoma) triangle |
| MEN-1 association | 20-25% of cases |
| Malignancy rate | >60% |
| Metastasis at diagnosis | 50-80% (liver, lymph nodes) |
| Diagnostic gastrin level | >1000 pg/mL with gastric pH <2 |
| Confirmatory test | Secretin stimulation (paradoxical rise >200 pg/mL) |
| Drug of choice | PPI (omeprazole/lansoprazole) |
| Best imaging | ⁶⁸Ga-DOTATATE PET/CT + EUS (>90% detection combined) |
Passaro's Triangle
- Junction of cystic duct + common bile duct (superior)
- Junction of 2nd and 3rd portions of duodenum (inferior)
- Junction of neck and body of pancreas (medial)
Clinical Features
- Abdominal pain + refractory/atypical peptic ulcers (duodenum, jejunum)
- Diarrhea - relieved by nasogastric suction (acid inactivates pancreatic enzymes)
- GERD / severe esophagitis
- Steatorrhea
- GI bleeding, weight loss
- Large gastric rugal folds on endoscopy
Diagnosis
- Stop PPIs 3 weeks before testing (they falsely elevate gastrin)
- Fasting serum gastrin + gastric pH together
- If equivocal (100-1000 pg/mL): Secretin stimulation test
- Tumor localization: ⁶⁸Ga-DOTATATE PET/CT → EUS → CT/MRI
Differential of Hypergastrinemia
- High acid: Gastrinoma, G-cell hyperplasia, gastric outlet obstruction, retained antrum
- Low acid: PPI/H2 blocker use, atrophic gastritis, pernicious anemia, renal failure, achlorhydria
Management
- Duodenal tumor → duodenotomy + full-thickness excision
- Pancreatic tumor → enucleation or formal pancreatectomy + lymph node clearance in Passaro's triangle
- Highly selective vagotomy if unresectable
Prognosis
- No liver metastases: ~80% 15-year survival
- Liver metastases: 20-50% 5-year survival
- Biochemical cure post-surgery (sporadic): ~30-40%
- Lymph node metastases alone do not worsen survival; liver metastases do
Generate a summary document on pancreatic neuroendocrine tumors
ls /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or not found"
mkdir -p /home/daytona/workspace/pnet-summary && ls /home/daytona/workspace/pnet-summary
~/pnet-summary/generate_pnet.js
const {
Document, Packer, Paragraph, TextRun, Table, TableRow, TableCell,
HeadingLevel, AlignmentType, BorderStyle, WidthType, ShadingType,
VerticalAlign, PageNumber, Header, Footer, TableOfContents,
PageBreak, UnderlineType
} = require('docx');
const fs = require('fs');
// ─── Color palette ───────────────────────────────────────────────────────────
const BLUE_DARK = "1A3A5C"; // Deep navy – main headings
const BLUE_MID = "2E6DA4"; // Mid blue – sub-headings, table headers
const BLUE_LIGHT = "D6E4F0"; // Pale blue – table header shading
const TEAL = "0E7C7B"; // Teal – h3 / callout labels
const GREY_BG = "F4F6F9"; // Very light grey – alternating table rows
const WHITE = "FFFFFF";
const TEXT_DARK = "1A1A1A";
// ─── Helpers ─────────────────────────────────────────────────────────────────
function h1(text) {
return new Paragraph({
heading: HeadingLevel.HEADING_1,
spacing: { before: 360, after: 120 },
children: [new TextRun({ text, color: BLUE_DARK, size: 36, bold: true, font: "Calibri" })]
});
}
function h2(text) {
return new Paragraph({
heading: HeadingLevel.HEADING_2,
spacing: { before: 280, after: 100 },
children: [new TextRun({ text, color: BLUE_MID, size: 28, bold: true, font: "Calibri" })]
});
}
function h3(text) {
return new Paragraph({
heading: HeadingLevel.HEADING_3,
spacing: { before: 200, after: 80 },
children: [new TextRun({ text, color: TEAL, size: 24, bold: true, font: "Calibri" })]
});
}
function body(text) {
return new Paragraph({
spacing: { before: 60, after: 60 },
children: [new TextRun({ text, size: 22, color: TEXT_DARK, font: "Calibri" })]
});
}
function bullet(text, bold_prefix = "") {
return new Paragraph({
bullet: { level: 0 },
spacing: { before: 40, after: 40 },
children: bold_prefix
? [
new TextRun({ text: bold_prefix, bold: true, size: 22, color: TEXT_DARK, font: "Calibri" }),
new TextRun({ text, size: 22, color: TEXT_DARK, font: "Calibri" })
]
: [new TextRun({ text, size: 22, color: TEXT_DARK, font: "Calibri" })]
});
}
function subbullet(text, bold_prefix = "") {
return new Paragraph({
bullet: { level: 1 },
spacing: { before: 30, after: 30 },
children: bold_prefix
? [
new TextRun({ text: bold_prefix, bold: true, size: 20, color: TEXT_DARK, font: "Calibri" }),
new TextRun({ text, size: 20, color: TEXT_DARK, font: "Calibri" })
]
: [new TextRun({ text, size: 20, color: TEXT_DARK, font: "Calibri" })]
});
}
function divider() {
return new Paragraph({
spacing: { before: 120, after: 120 },
border: { bottom: { style: BorderStyle.SINGLE, size: 1, color: BLUE_MID } },
children: []
});
}
function spacer() {
return new Paragraph({ children: [new TextRun({ text: "" })] });
}
// ─── Table helpers ────────────────────────────────────────────────────────────
function makeTableRow(cells, isHeader = false, shade = WHITE) {
return new TableRow({
tableHeader: isHeader,
children: cells.map(cell =>
new TableCell({
shading: isHeader
? { fill: BLUE_LIGHT, type: ShadingType.CLEAR, color: "auto" }
: { fill: shade, type: ShadingType.CLEAR, color: "auto" },
verticalAlign: VerticalAlign.CENTER,
margins: { top: 80, bottom: 80, left: 120, right: 120 },
children: [new Paragraph({
alignment: AlignmentType.LEFT,
children: [new TextRun({
text: cell,
bold: isHeader,
size: isHeader ? 20 : 19,
color: isHeader ? BLUE_DARK : TEXT_DARK,
font: "Calibri"
})]
})]
})
)
});
}
function makeTable(headers, rows, colWidths) {
const headerRow = makeTableRow(headers, true);
const dataRows = rows.map((row, i) =>
makeTableRow(row, false, i % 2 === 0 ? WHITE : GREY_BG)
);
return new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
columnWidths: colWidths,
rows: [headerRow, ...dataRows],
borders: {
top: { style: BorderStyle.SINGLE, size: 4, color: BLUE_MID },
bottom: { style: BorderStyle.SINGLE, size: 4, color: BLUE_MID },
left: { style: BorderStyle.SINGLE, size: 4, color: BLUE_MID },
right: { style: BorderStyle.SINGLE, size: 4, color: BLUE_MID },
insideH:{ style: BorderStyle.SINGLE, size: 2, color: "CCCCCC" },
insideV:{ style: BorderStyle.SINGLE, size: 2, color: "CCCCCC" },
}
});
}
// ─── Title page elements ──────────────────────────────────────────────────────
function titleBlock() {
return [
new Paragraph({ spacing: { before: 800, after: 200 }, children: [] }),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 0, after: 160 },
children: [new TextRun({ text: "PANCREATIC NEUROENDOCRINE TUMORS", bold: true, size: 52, color: BLUE_DARK, font: "Calibri" })]
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 0, after: 120 },
children: [new TextRun({ text: "A Comprehensive Clinical Summary", size: 36, color: BLUE_MID, italics: true, font: "Calibri" })]
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 0, after: 60 },
children: [new TextRun({ text: "PNETs / panNENs", size: 28, color: TEAL, bold: true, font: "Calibri" })]
}),
divider(),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 60, after: 60 },
children: [new TextRun({ text: "Sources: Harrison's Principles of Internal Medicine 22e (2025) | Schwartz's Principles of Surgery 11e", size: 18, color: "666666", italics: true, font: "Calibri" })]
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 0, after: 60 },
children: [new TextRun({ text: "Fischer's Mastery of Surgery 8e | Maingot's Abdominal Operations | Current Surgical Therapy 14e", size: 18, color: "666666", italics: true, font: "Calibri" })]
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 0, after: 60 },
children: [new TextRun({ text: `Date: ${new Date().toLocaleDateString('en-GB', {day:'2-digit',month:'long',year:'numeric'})}`, size: 18, color: "666666", font: "Calibri" })]
}),
new Paragraph({ children: [new PageBreak()] })
];
}
// ─── Document content ─────────────────────────────────────────────────────────
const content = [
...titleBlock(),
// ═══════════════════════════════════════════════════════════════════
h1("1. Overview & Epidemiology"),
body("Pancreatic neuroendocrine tumors (PNETs), also called panNETs or islet cell tumors, are a heterogeneous group of neoplasms arising from precursor cells of the endocrine pancreas. They were first described in 1869 and account for approximately 7% of all neuroendocrine tumors and only 1-3% of all pancreatic neoplasms."),
spacer(),
bullet("Incidence: ~0.5 per 100,000 persons per year (rising due to improved cross-sectional imaging)"),
bullet("The incidence of gastroenteropancreatic NETs increased 6.4-fold in the US between 1973-2012 (SEER data)"),
bullet("Mean age at diagnosis: 50 years; slight male predominance for some subtypes"),
bullet("80-90% are sporadic; 10-20% are associated with familial syndromes"),
bullet("60-90% are nonfunctional (NF-PNETs) - found incidentally on imaging"),
spacer(),
h3("Hereditary Syndromes Associated with PNETs"),
makeTable(
["Syndrome", "Gene / Locus", "Associated Features"],
[
["MEN-1 (most common)", "MEN1 / 11q13 (menin)", "Parathyroid hyperplasia, pituitary adenoma, pancreatic NETs"],
["Von Hippel-Lindau (VHL)", "VHL / 3p25", "Cerebellar hemangioblastoma, renal cell carcinoma, pheochromocytoma"],
["Neurofibromatosis type 1", "NF1 (neurofibromin)", "Café au lait spots, neurofibromas, pancreatic & extrapancreatic NETs"],
["Tuberous sclerosis", "TSC1 (hamartin) / TSC2 (tuberin)", "Hamartomas, renal angiomyolipomas, cortical tubers"]
],
[2500, 2000, 3500]
),
spacer(),
divider(),
// ═══════════════════════════════════════════════════════════════════
h1("2. Classification (WHO 2017)"),
body("The 2017 WHO classification relies on histopathologic criteria — Ki-67 proliferative index and mitotic count — to predict tumor grade and biologic behavior. Two broad categories exist: well-differentiated panNETs and poorly differentiated panNECs."),
spacer(),
makeTable(
["Classification / Grade", "Differentiation", "Ki-67 Index (%)", "Mitotic Count / 10 HPF"],
[
["panNET Grade 1 (Low)", "Well-differentiated", "< 3%", "< 2"],
["panNET Grade 2 (Intermediate)", "Well-differentiated", "3 – 20%", "2 – 20"],
["panNET Grade 3 (High)", "Well-differentiated", "> 20%", "> 20"],
["panNEC Grade 3 (Small cell / Large cell)", "Poorly differentiated", "> 20%", "> 20"]
],
[2500, 2000, 2000, 2000]
),
spacer(),
body("Key terminological distinction:"),
bullet("panNEN (pancreatic neuroendocrine neoplasm) = entire heterogeneous group"),
bullet("panNET = well-differentiated tumors; generally lower malignant potential"),
bullet("panNEC = poorly differentiated carcinoma; behaves aggressively like SCLC"),
body("Immunohistochemistry: Staining for chromogranin A and synaptophysin confirms neuroendocrine differentiation. Grade 3 tumors show marked pleomorphism and abundant mitoses."),
spacer(),
h3("Molecular Features"),
bullet("MEN1 gene mutations: 44% of sporadic PNETs (most common)"),
bullet("DAXX / ATRX mutations: 43% of sporadic PNETs (chromatin remodeling complex)"),
bullet("mTOR pathway mutations: 15% of PNETs"),
divider(),
// ═══════════════════════════════════════════════════════════════════
h1("3. Classification: Functional vs. Nonfunctional"),
h2("3A. Nonfunctional PNETs (NF-PNETs)"),
body("NF-PNETs comprise 60-90% of all PNETs. They do not produce clinically significant hormonal syndromes. Most are discovered incidentally on cross-sectional imaging done for other purposes (trauma, abdominal pain workup, etc.)."),
spacer(),
bullet("Presentation: Abdominal pain, weight loss, early satiety (mass effect), biliary obstruction with jaundice (head tumors), or incidental finding"),
bullet("Often larger at diagnosis due to absence of hormone-related symptoms"),
bullet("In rare cases: fulminant hepatic failure from liver replacement by poorly differentiated PNETs"),
bullet("Equally distributed across head, body, and tail of pancreas"),
spacer(),
h2("3B. Functional PNETs (F-PNETs) — Overview"),
body("F-PNETs produce excess hormones causing well-defined clinical syndromes. Because of the recognizable syndromes, they are typically detected earlier and at smaller sizes."),
spacer(),
makeTable(
["Tumor Type", "Hormone", "Incidence / 10⁶ / year", "% Malignant", "% MEN-1", "Classic Syndrome"],
[
["Insulinoma", "Insulin", "1 – 3", "10%", "10%", "Whipple's triad: fasting hypoglycemia, glucose <50 mg/dL, relief with glucose"],
["Gastrinoma", "Gastrin", "0.5 – 1.5", "> 60%", "20-25%", "Zollinger-Ellison syndrome: peptic ulcers, diarrhea, acid hypersecretion"],
["Glucagonoma", "Glucagon", "0.01 – 0.1", "50-80%", "Rare", "Necrolytic migratory erythema, diabetes, weight loss, DVT"],
["VIPoma", "VIP", "0.05 – 0.2", "40-70%", "6%", "WDHA: watery diarrhea (>3 L/day), hypokalemia, achlorhydria"],
["Somatostatinoma", "Somatostatin", "Rare", "> 70%", "45%", "Diabetes, steatorrhea, cholelithiasis, diarrhea (inhibitory triad)"],
["PPoma / Non-functional", "PP / none", "Common", "Variable", "18%", "Mass effect symptoms only"]
],
[1800, 1200, 1500, 1200, 1000, 3200]
),
spacer(),
divider(),
// ═══════════════════════════════════════════════════════════════════
h1("4. Individual Functional Tumors"),
h2("4A. Insulinoma"),
body("Insulinomas are the most common functional pancreatic endocrine neoplasm. They are uniformly distributed throughout the head, body, and tail of the pancreas."),
bullet("Clinical: Whipple's Triad — (1) symptoms of hypoglycemia, (2) blood glucose <50 mg/dL during symptoms, (3) relief of symptoms with glucose administration"),
bullet("Symptoms: Palpitations, trembling, diaphoresis, confusion, seizures, obtundation, personality change"),
bullet("90% are benign and solitary; 10% are malignant"),
bullet("10% are associated with MEN-1 (more likely to be multifocal, higher recurrence)"),
spacer(),
h3("Diagnosis"),
subbullet("72-hour supervised fast: sample glucose, insulin, C-peptide, proinsulin, and sulfonylurea every 4-6 hours and when symptomatic"),
subbullet("Elevated insulin + low glucose during fast = diagnostic"),
subbullet("Elevated C-peptide confirms endogenous origin (rules out exogenous insulin injection)"),
subbullet("Check sulfonylurea levels to rule out drug-induced hypoglycemia"),
spacer(),
h3("Localization & Surgery"),
subbullet("CT + EUS: identifies >90% of insulinomas preoperatively"),
subbullet("Intraoperative ultrasound (IOUS) confirms tumor location and relationship to main pancreatic duct"),
subbullet("Treatment: Simple enucleation for most; distal pancreatectomy or pancreaticoduodenectomy for tumors >2 cm or those close to the main duct"),
subbullet("Nearly 100% cure rate for benign solitary insulinomas"),
spacer(),
h2("4B. Gastrinoma (Zollinger-Ellison Syndrome)"),
body("Gastrinomas are the second most common functional pancreatic NET. They arise predominantly in the 'gastrinoma triangle' (Passaro's triangle)."),
bullet("Location: 80-90% within Passaro's triangle (cystic duct confluence → D2/D3 junction → neck/body of pancreas); 50-90% of sporadic cases arise in the duodenum"),
bullet("Clinical (ZES): Severe refractory peptic ulcers (90%), diarrhea (21-40% at diagnosis), GERD, steatorrhea, large gastric rugal folds"),
bullet("Malignancy: >60% are malignant; 50-80% have metastases at diagnosis (liver, lymph nodes)"),
bullet("Key physiology: Not suppressed by low luminal pH; paradoxically stimulated by secretin"),
spacer(),
h3("Diagnosis"),
subbullet("Fasting serum gastrin >1000 pg/mL + gastric pH <2 = diagnostic"),
subbullet("Secretin stimulation test: paradoxical rise in gastrin >200 pg/mL (>85% sensitivity, >95% specificity)"),
subbullet("Stop PPIs 3 weeks before testing to avoid false elevation"),
subbullet("Basal acid output (BAO) >15 mEq/h in ZES"),
spacer(),
h3("Management"),
subbullet("PPIs: Drug of choice; target BAO <10 mEq/h"),
subbullet("Localization: 68Ga-DOTATATE PET/CT + EUS (>90% detection combined)"),
subbullet("Surgery: Recommended for all sporadic resectable gastrinomas; duodenotomy + node clearance of Passaro's triangle"),
subbullet("MEN-1: Treat hyperparathyroidism first; surgery for tumors >2-2.5 cm"),
subbullet("Prognosis: 15-year survival ~80% without liver metastases; 20-50% 5-year survival with liver metastases"),
spacer(),
h2("4C. Glucagonoma"),
body("Glucagonomas are rare tumors producing excess glucagon. Most arise in the body and tail of the pancreas and are large (>5 cm) at diagnosis."),
bullet("Classic presentation: 4 D's — Dermatitis (necrolytic migratory erythema), Diabetes mellitus, DVT (deep vein thrombosis), Depression"),
bullet("Necrolytic migratory erythema (NME): Pathognomonic rash — migratory, crusting, blistering eruption predominantly on lower extremities, perineum, and perioral areas"),
bullet("Other features: Weight loss, anemia, hypoaminoacidemia, glossitis, stomatitis"),
bullet("50-80% are malignant at diagnosis; majority have liver or lymph node metastases"),
spacer(),
h3("Diagnosis & Management"),
subbullet("Elevated fasting plasma glucagon (>500 pg/mL; normal <150 pg/mL)"),
subbullet("CT/MRI for localization and staging; usually large and easily identified"),
subbullet("Somatostatin analogues: Control symptoms (especially NME and diarrhea) preoperatively"),
subbullet("Surgical resection: Distal pancreatectomy for body/tail tumors; curative in ~30%"),
subbullet("Correct hypoaminoacidemia with IV amino acids (improves NME before surgery)"),
spacer(),
h2("4D. VIPoma (WDHA Syndrome / Verner-Morrison Syndrome)"),
body("VIPomas secrete vasoactive intestinal peptide (VIP). First described by Verner and Morrison in 1958. Also called pancreatic cholera or WDHA syndrome."),
bullet("WDHA: Watery Diarrhea (>3 L/day, episodic, secretory — persists with fasting), Hypokalemia, Achlorhydria"),
bullet("Life-threatening hypovolemia and electrolyte disturbance; can present with tetany"),
bullet("60-75% arise in the pancreatic body/tail; 40-70% malignant"),
spacer(),
h3("Diagnosis & Management"),
subbullet("Serum VIP level >200 pg/mL (measure multiple times — episodic secretion)"),
subbullet("Aggressive IV fluid and electrolyte replacement preoperatively"),
subbullet("Somatostatin analogues (octreotide/lanreotide): Dramatically reduce diarrhea and allow fluid replacement"),
subbullet("CT: Usually localizes tumor (most have already spread outside pancreas at diagnosis)"),
subbullet("Surgery: Distal pancreatectomy; debulking for palliation in advanced disease"),
spacer(),
h2("4E. Somatostatinoma"),
body("Somatostatinomas are the rarest functional PNETs. They produce excess somatostatin which inhibits multiple GI functions."),
bullet("Inhibitory triad: Diabetes mellitus (inhibition of insulin), Steatorrhea/malabsorption (inhibition of pancreatic enzymes), Cholelithiasis (inhibition of CCK → bile stasis)"),
bullet("Diarrhea, hypochlorhydria, weight loss"),
bullet(">70% are malignant at diagnosis"),
bullet("45% associated with MEN-1 or NF-1"),
bullet("Most arise in the pancreatic head or periampullary duodenum"),
spacer(),
divider(),
// ═══════════════════════════════════════════════════════════════════
h1("5. Investigations & Staging"),
h2("5A. Biochemical Workup"),
body("All suspected PNETs should undergo a thorough hormonal and general biochemical evaluation:"),
makeTable(
["Test", "Significance"],
[
["Fasting serum gastrin", "Gastrinoma (>1000 pg/mL with pH <2 diagnostic)"],
["Fasting serum insulin + glucose + C-peptide", "Insulinoma (insulin:glucose ratio elevated)"],
["Plasma glucagon", "Glucagonoma (>500 pg/mL)"],
["Serum VIP", "VIPoma (>200 pg/mL)"],
["Serum somatostatin", "Somatostatinoma"],
["Chromogranin A (CgA)", "Universal NET marker; elevated in 60-80% of all PNETs; mirrors tumor burden"],
["Pancreastatin", "Marker of NET activity; less affected by PPI use than CgA"],
["5-HIAA (urine)", "Carcinoid syndrome (serotonin-producing NETs)"],
["Serum calcium, PTH", "Screen for MEN-1 (hyperparathyroidism)"],
["Secretin stimulation test", "Confirms gastrinoma (paradoxical gastrin rise >200 pg/mL)"],
["72-hour supervised fast", "Gold standard for insulinoma"]
],
[3500, 5500]
),
spacer(),
h2("5B. Imaging & Localization"),
makeTable(
["Modality", "Sensitivity / Use", "Key Points"],
[
["Triple-phase CT (with/without contrast)", "~70-80% overall", "First-line; PNETs are hypervascular — enhance in arterial phase; staging of liver metastases"],
["MRI / MRCP", "~80-90%", "Superior for small lesions and liver metastases; no radiation"],
["Endoscopic Ultrasound (EUS)", ">90% for small pancreatic/duodenal tumors", "Best for lesions <1 cm in pancreatic head/duodenal wall; guides tissue biopsy"],
["68Ga-DOTATATE PET/CT", "Highest sensitivity (~90-95%)", "First-line functional imaging; somatostatin receptor scintigraphy; detects primary + all metastases"],
["Octreotide scintigraphy (OctreoScan)", "~80-85%", "Older modality; now largely replaced by 68Ga-DOTATATE PET/CT"],
["Intraoperative Ultrasound (IOUS)", "Very high", "Detects occult tumors missed on preoperative imaging; guides enucleation vs. resection decision"],
["Selective angiography / portal venous sampling", "Adjunct", "Reserved for cases unlocalized by other methods"],
["FDG-PET/CT", "For high-grade tumors", "Useful for poorly differentiated panNEC (grade 3); inverse relationship to somatostatin receptor expression"]
],
[2500, 2000, 4500]
),
spacer(),
h2("5C. Tissue Diagnosis & Histopathology"),
bullet("Core biopsy or FNA (EUS-guided) for tissue diagnosis when surgery is not immediately planned"),
bullet("Immunohistochemistry: Chromogranin A, Synaptophysin (neuroendocrine markers), Ki-67 staining (grade)"),
bullet("Electron microscopy: Dense-core neurosecretory granules"),
bullet("Specific hormone staining (insulin, glucagon, gastrin, VIP, somatostatin) for functional tumors"),
spacer(),
divider(),
// ═══════════════════════════════════════════════════════════════════
h1("6. Management"),
h2("6A. Surgical Management"),
body("Surgery is the only potentially curative treatment and should be considered in all patients with resectable disease. Approach varies by tumor type, size, location, and presence of MEN-1."),
spacer(),
makeTable(
["Tumor / Situation", "Surgical Approach"],
[
["Small NF-PNET (<2 cm, no malignant features)", "Active surveillance; surgery if growing or symptomatic"],
["NF-PNET >2 cm", "Resection: enucleation (if away from main duct) or formal pancreatectomy"],
["Insulinoma (benign, solitary)", "Enucleation; >90% cure rate"],
["Insulinoma (close to main duct, >2 cm)", "Distal pancreatectomy or pancreaticoduodenectomy"],
["Duodenal gastrinoma (sporadic)", "Duodenotomy + full-thickness excision + lymph node clearance of Passaro's triangle"],
["Pancreatic gastrinoma (sporadic)", "Enucleation or formal pancreatectomy; regional lymphadenectomy always"],
["Gastrinoma in MEN-1", "Surgery for tumors >2-2.5 cm only; parathyroidectomy first"],
["Glucagonoma", "Distal pancreatectomy (body/tail); correct hypoaminoacidemia first"],
["VIPoma", "Distal pancreatectomy; debulking for palliation"],
["Pancreatic head tumor with ductal involvement", "Pancreaticoduodenectomy (Whipple procedure)"],
["Resectable liver metastases", "Synchronous or staged hepatic resection if primary controlled and complete removal feasible"],
["Intraoperative occult tumor", "IOUS + duodenotomy for thorough exploration"]
],
[3500, 5500]
),
spacer(),
h3("Highly Selective Vagotomy"),
body("May be performed when gastrinoma cannot be localized or unresectable disease is found — reduces acid secretion and decreases PPI requirement without compromising gastric motility."),
spacer(),
h2("6B. Medical Management of Hormone Excess"),
makeTable(
["Condition", "Medical Treatment"],
[
["Gastrinoma (ZES)", "PPI (omeprazole/lansoprazole) — drug of choice; target BAO <10 mEq/h; add H2 blockers if needed"],
["Insulinoma (preop/inoperable)", "Diazoxide (inhibits insulin release); frequent small meals; IV dextrose for hypoglycemic crises"],
["Glucagonoma", "Somatostatin analogue (octreotide) — controls NME, diarrhea; IV amino acid infusion for NME"],
["VIPoma", "Octreotide/lanreotide — dramatically reduces diarrhea; IV fluid + electrolyte replacement"],
["Somatostatinoma", "Surgical resection; supportive management of diabetes, enzyme replacement for steatorrhea"],
["General hormonal control", "Somatostatin analogues (octreotide, lanreotide) — effective across multiple tumor types"]
],
[2500, 6500]
),
spacer(),
h2("6C. Management of Metastatic / Advanced PNETs"),
body("Treatment of metastatic PNETs requires a multidisciplinary approach. The selection of therapy depends on tumor grade, somatostatin receptor expression, extent of disease, and rate of progression."),
spacer(),
h3("Systemic Therapies"),
makeTable(
["Treatment", "Indication / Key Points"],
[
["Somatostatin analogues (octreotide, lanreotide)", "Symptom control AND antiproliferative; first-line for low/intermediate grade, receptor-positive tumors"],
["PRRT (177Lu-DOTATATE — Lutathera)", "Peptide receptor radionuclide therapy; high receptor expression; grade 1-2; significant OS improvement (NETTER-1 trial)"],
["Everolimus (mTOR inhibitor)", "Grade 1-2 pancreatic NETs; approved for progressive disease (RADIANT-3 trial)"],
["Sunitinib (tyrosine kinase inhibitor)", "Pancreatic NETs; targets VEGFR, PDGFR; approved for progressive well-differentiated pNETs"],
["Chemotherapy (streptozotocin + 5-FU ± doxorubicin)", "Poorly differentiated panNEC or rapidly progressive well-differentiated tumors; response rate ~40%"],
["Temozolomide ± capecitabine (TEMCAP)", "Pancreatic NETs with MGMT promoter methylation; response rate ~40-70%"],
["Interferon-alpha", "Adjunct antiproliferative; limited use due to side effects"]
],
[3000, 6000]
),
spacer(),
h3("Liver-Directed Therapies"),
bullet("Surgical hepatic resection: If primary controlled + complete removal feasible"),
bullet("Hepatic artery embolization (HAE) / chemoembolization (TACE): Liver-dominant disease"),
bullet("Radiofrequency ablation (RFA) / microwave ablation: Focal liver metastases"),
bullet("Selective internal radiation therapy (SIRT / Y-90 radioembolization): Unresectable liver metastases"),
bullet("Liver transplantation: Highly selected patients with unresectable liver-only metastases (5-year survival ~60% in selected cases)"),
spacer(),
divider(),
// ═══════════════════════════════════════════════════════════════════
h1("7. Surveillance & Follow-Up"),
body("Post-resection surveillance is essential given the potential for late recurrence. Strategy depends on grade and whether biochemical cure was achieved."),
spacer(),
bullet("Serum markers: Fasting serum gastrin, CgA, specific hormone levels (depending on tumor type)"),
bullet("Secretin stimulation test: For gastrinoma recurrence"),
bullet("Cross-sectional imaging (CT/MRI): Every 3-6 months initially, then annually"),
bullet("68Ga-DOTATATE PET/CT: For suspected recurrence or restaging"),
bullet("OGD surveillance: For gastrinoma patients"),
spacer(),
body("For NF-PNETs managed conservatively (<2 cm), annual imaging surveillance to detect growth is standard practice."),
divider(),
// ═══════════════════════════════════════════════════════════════════
h1("8. Prognosis"),
makeTable(
["Tumor Type / Situation", "Prognosis"],
[
["Benign insulinoma (sporadic, resected)", "Near 100% cure; excellent long-term survival"],
["Gastrinoma — no liver metastases", "~80% 15-year survival"],
["Gastrinoma — liver metastases", "20-50% 5-year survival"],
["MEN-1 gastrinoma <2.5 cm (no metastases)", "100% at 15 years"],
["MEN-1 gastrinoma with metastases", "52% at 15 years"],
["Glucagonoma (resected)", "~60% 5-year survival; high recurrence"],
["NF-PNET Grade 1 (resected)", "Excellent; >80% 5-year survival"],
["NF-PNET Grade 2", "Good; 60-80% 5-year survival"],
["panNEC Grade 3 (poorly differentiated)", "Poor; median survival <2 years"],
["Biochemical cure after gastrinoma surgery (sporadic)", "~30-40%"],
["Biochemical cure (MEN-1)", "~5% at 5 years"]
],
[4000, 5000]
),
spacer(),
body("Key prognostic factors: Tumor grade (Ki-67 / mitotic index), presence of liver metastases, complete surgical resection, sporadic vs. MEN-1 context, and tumor size at diagnosis."),
body("Note: Lymph node metastases alone (without liver involvement) do NOT significantly reduce long-term survival in gastrinomas and many other PNETs."),
divider(),
// ═══════════════════════════════════════════════════════════════════
h1("9. Quick Reference Summary Tables"),
h2("Functional PNET Comparison"),
makeTable(
["Feature", "Insulinoma", "Gastrinoma", "Glucagonoma", "VIPoma", "Somatostatinoma"],
[
["Hormone", "Insulin", "Gastrin", "Glucagon", "VIP", "Somatostatin"],
["Syndrome", "Whipple's triad", "Zollinger-Ellison", "4 D's + NME", "WDHA", "Inhibitory triad"],
["Most common site", "Uniform pancreas", "Duodenum (sporadic)", "Body/tail", "Body/tail", "Head / duodenum"],
["Malignancy", "10%", ">60%", "50-80%", "40-70%", ">70%"],
["MEN-1", "10%", "20-25%", "Rare", "6%", "45%"],
["Key test", "72-h fast", "Fasting gastrin + secretin stimulation", "Plasma glucagon", "Serum VIP", "Plasma somatostatin"],
["Drug of choice", "Diazoxide / glucose", "PPI (omeprazole)", "Octreotide", "Octreotide + IVF", "Symptomatic"],
["Surgery", "Enucleation", "Duodenotomy / enucleation / resection", "Distal pancreatectomy", "Distal pancreatectomy", "Resection"]
],
[2200, 1800, 2000, 1700, 1600, 2200]
),
spacer(),
h2("WHO 2017 Grade Summary"),
makeTable(
["Grade", "Differentiation", "Ki-67 (%)", "Mitotic Rate", "Behavior"],
[
["Grade 1", "Well-differentiated", "<3%", "<2/10 HPF", "Slow-growing; excellent prognosis"],
["Grade 2", "Well-differentiated", "3-20%", "2-20/10 HPF", "Intermediate behavior"],
["Grade 3 (panNET)", "Well-differentiated", ">20%", ">20/10 HPF", "Aggressive but better than panNEC"],
["Grade 3 (panNEC)", "Poorly differentiated", ">20%", ">20/10 HPF", "Very aggressive; treat like SCLC"]
],
[1500, 2000, 1800, 2200, 3500]
),
spacer(),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 400, after: 100 },
children: [new TextRun({ text: "— End of Document —", size: 18, italics: true, color: "888888", font: "Calibri" })]
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 0, after: 60 },
children: [new TextRun({
text: "Sources: Harrison's 22e (2025) | Schwartz's Surgery 11e | Fischer's Mastery of Surgery 8e | Maingot's Abdominal Operations | Current Surgical Therapy 14e | Robbins & Cotran Pathology 10e",
size: 16, italics: true, color: "999999", font: "Calibri"
})]
})
];
// ─── Build document ───────────────────────────────────────────────────────────
const doc = new Document({
creator: "Orris Medical AI",
title: "Pancreatic Neuroendocrine Tumors – Summary Document",
description: "Comprehensive clinical summary of PNETs",
styles: {
paragraphStyles: [
{
id: "Normal",
name: "Normal",
run: { font: "Calibri", size: 22 }
}
]
},
sections: [{
properties: {
page: {
margin: { top: 1080, bottom: 1080, left: 1080, right: 1080 }
}
},
headers: {
default: new Header({
children: [new Paragraph({
alignment: AlignmentType.RIGHT,
border: { bottom: { style: BorderStyle.SINGLE, size: 1, color: BLUE_MID } },
children: [
new TextRun({ text: "Pancreatic Neuroendocrine Tumors (PNETs)", size: 18, color: BLUE_MID, font: "Calibri" })
]
})]
})
},
footers: {
default: new Footer({
children: [new Paragraph({
alignment: AlignmentType.CENTER,
border: { top: { style: BorderStyle.SINGLE, size: 1, color: "CCCCCC" } },
children: [
new TextRun({ text: "Page ", size: 16, color: "888888", font: "Calibri" }),
new TextRun({ children: [PageNumber.CURRENT], size: 16, color: "888888", font: "Calibri" }),
new TextRun({ text: " | Orris Medical AI | Compiled from authoritative surgical & medical textbooks", size: 16, color: "888888", font: "Calibri" })
]
})]
})
},
children: content
}]
});
Packer.toBuffer(doc).then(buffer => {
fs.writeFileSync('/home/daytona/workspace/pnet-summary/PNET_Summary.docx', buffer);
console.log('SUCCESS: Document written to /home/daytona/workspace/pnet-summary/PNET_Summary.docx');
}).catch(err => {
console.error('ERROR:', err);
process.exit(1);
});
cd /home/daytona/workspace/pnet-summary && node generate_pnet.js 2>&1
python3 /home/daytona/skills/docx/scripts/office/validate.py /home/daytona/workspace/pnet-summary/PNET_Summary.docx 2>&1
ls -lh /home/daytona/workspace/pnet-summary/PNET_Summary.docx && python3 -c "import zipfile; z=zipfile.ZipFile('/home/daytona/workspace/pnet-summary/PNET_Summary.docx'); print('Valid ZIP. Files:', len(z.namelist())); print(z.namelist()[:10])"
PNET Summary
Word Document · DOCX
What's inside the document
| Section | Content |
|---|---|
| 1. Overview & Epidemiology | Incidence trends, sporadic vs. hereditary (MEN-1, VHL, NF-1, TSC), hereditary syndrome table |
| 2. WHO 2017 Classification | WHO grading table (Grade 1-3, panNEC), Ki-67/mitotic criteria, molecular features (MEN1, DAXX/ATRX, mTOR mutations) |
| 3. Functional vs. Nonfunctional | Overview table comparing all functional PNETs (incidence, malignancy %, MEN-1 %, syndrome) |
| 4. Individual Functional Tumors | Insulinoma, Gastrinoma (ZES), Glucagonoma, VIPoma, Somatostatinoma - each with diagnosis and management |
| 5. Investigations & Staging | Biochemical workup table, imaging modality comparison table (CT, MRI, EUS, 68Ga-DOTATATE, IOUS), histopathology |
| 6. Management | Surgical approach table by tumor type, medical management table, metastatic disease (PRRT/Lutathera, everolimus, sunitinib, TACE, SIRT, liver transplant) |
| 7. Surveillance | Post-resection follow-up protocols |
| 8. Prognosis | Survival data by tumor type, grade, and metastatic status |
| 9. Quick Reference Tables | Side-by-side functional PNET comparison; WHO grade summary |
Generate a summary document on pancreatic neuroendocrine tumors
ls -lh /home/daytona/workspace/pnet-summary/PNET_Summary.docx
PNET Summary
Word Document · DOCX
- Overview & Epidemiology - Incidence, hereditary syndromes (MEN-1, VHL, NF-1, TSC)
- WHO 2017 Classification - Grade 1/2/3 panNET vs panNEC; Ki-67/mitotic thresholds; molecular features
- Functional vs. Nonfunctional PNETs - Comparative overview table of all F-PNET types
- Individual Functional Tumors - Insulinoma, Gastrinoma (ZES), Glucagonoma, VIPoma, Somatostatinoma
- Investigations & Staging - Biochemical workup, imaging modality comparison (CT, MRI, EUS, ⁶⁸Ga-DOTATATE PET/CT)
- Management - Surgical approaches by tumor type, medical therapy, metastatic disease (PRRT, everolimus, sunitinib, TACE/SIRT)
- Surveillance - Post-resection follow-up protocols
- Prognosis - Survival data by tumor type, grade, and metastasis status
- Quick Reference Tables - Side-by-side functional PNET comparison; WHO grade summary
Somatostatinoma
Somatostatinoma
Definition & Background
Epidemiology
- Presents most commonly between ages 40-70 years
- Equal male to female distribution
- 80-90% are sporadic; ~10-20% associated with hereditary syndromes
- 45% associated with MEN-1 in some series (though Harrison's notes only rare MEN-1 association)
- Strong association with NF-1 (neurofibromatosis type 1): duodenal tumors 43%; pancreatic tumors 6-21%
- Incidence is rising due to improved cross-sectional imaging
Location
| Site | Frequency |
|---|---|
| Pancreas (head/body/tail) | ~50% |
| Duodenum | ~50% (most common GI site) |
| Periampullary / ampulla | 20% of all cases; often aggressive course |
| Jejunum | Rare |
- Mean size of pancreatic tumors: 5-6 cm (large at diagnosis)
- Mean size of duodenal tumors: ~2 cm (smaller)
- Most common location overall: duodenum, followed by pancreatic head
- The ampulla and periampullary area account for ~60% of cases in some surgical series
- Tumors are almost always solitary; multiple tumors suggest MEN-1
Pathophysiology - Why the "Inhibitory Triad" Occurs
| Effect of Excess Somatostatin | Clinical Consequence |
|---|---|
| Inhibits insulin secretion | Diabetes mellitus / glucose intolerance |
| Inhibits CCK release → reduced gallbladder contraction | Cholelithiasis (gallstones) via bile stasis |
| Inhibits pancreatic exocrine secretion (enzymes + bicarbonate) | Steatorrhea / fat malabsorption |
| Inhibits bile secretion and gallbladder emptying | Worsens steatorrhea and cholelithiasis |
| Inhibits gastric acid secretion | Hypochlorhydria / achlorhydria |
| Inhibits intestinal absorption of amino acids, sugars, calcium | Malabsorption, weight loss |
| Inhibits gastrin, secretin, GIP | Altered upper GI function |
Clinical Features
The Classic "Inhibitory Triad" (Somatostatinoma Syndrome)
- Diabetes mellitus - most prominent; present in >30% of patients; ranges from mild (oral hypoglycemic-controlled) to severe (insulin-dependent)
- Steatorrhea / diarrhea - fat malabsorption from inhibited pancreatic enzymes and bile; watery, foul-smelling, fatty stools
- Cholelithiasis (gallstones) - present in 16-64% of patients; due to somatostatin inhibiting CCK and gallbladder contraction
Additional Clinical Features
| Feature | Notes |
|---|---|
| Abdominal pain | Most common presenting symptom (~25%); from tumor mass effect or cholelithiasis |
| Jaundice | ~25%; biliary obstruction from periampullary/pancreatic head tumor |
| Diarrhea | Secretory and malabsorptive components |
| Weight loss | 20-30% of patients; from malabsorption and anorexia |
| Hypochlorhydria | From gastric acid inhibition |
| Mild anemia | Common |
| GI bleeding | Especially duodenal tumors; from tumor ulceration or ampullary involvement |
| Pancreatitis | Periampullary duodenal tumors causing ductal obstruction |
Important Clinical Notes
- Because symptoms are insidious and nonspecific (diabetes, gallstones, diarrhea are all common conditions individually), most patients are diagnosed with locally advanced or metastatic disease
- Many NF-NETs stain for somatostatin on IHC but do not produce the clinical syndrome - true somatostatinoma syndrome requires both elevated serum somatostatin AND clinical symptoms
- Pancreatic tumors are far more likely to cause the full clinical syndrome (19%) vs. duodenal tumors (only 3% cause the full syndrome)
- Duodenal tumors more often cause symptoms from local tumor growth (biliary obstruction, bleeding, pancreatitis) rather than hormonal excess
Histological Clue
- Duodenal somatostatinomas characteristically display psammoma bodies (calcified concentric lamellated deposits) on histology - rare in pancreatic somatostatinomas and other GI NETs - a distinguishing pathological feature
Diagnosis
Biochemical Confirmation
- Elevated plasma somatostatin level is the key diagnostic test
- Normal fasting somatostatin: <25 pg/mL
- In somatostatinoma syndrome: typically >10 ng/mL (Schwartz's) - markedly elevated
- Must document both elevated somatostatin and compatible clinical symptoms (since many NETs stain immunohistochemically for somatostatin without causing the syndrome)
- Provocative testing (arginine or tolbutamide stimulation) does not aid diagnosis
- Check chromogranin A (CgA) - elevated in most PNETs; useful for monitoring
Other Investigations
| Test | Purpose |
|---|---|
| Fasting blood glucose, HbA1c | Assess degree of diabetes |
| Lipid profile, fecal fat (72-hour stool collection) | Confirm steatorrhea |
| LFTs, bilirubin, ALP | Biliary obstruction |
| Abdominal ultrasound | Gallstones, biliary dilation |
| Serum calcium, PTH | Screen for MEN-1 |
| Genetic testing (NF-1, MEN-1) | If hereditary syndrome suspected |
Tumor Localization & Staging
| Modality | Key Points |
|---|---|
| Triple-phase CT (arterial + venous) | First-line; PNETs are hypervascular (arterial enhancement); staging of liver metastases |
| MRI / MRCP | Superior for liver metastases and biliary anatomy; useful for periampullary tumors |
| EUS (Endoscopic Ultrasound) | Best for small pancreatic head and duodenal tumors; can biopsy |
| ⁶⁸Ga-DOTATATE PET/CT | Highest sensitivity (~90-95%); somatostatin receptor-based; detects primary + all metastases; paradoxically, somatostatinomas strongly express somatostatin receptors |
| OGD (upper endoscopy) | Visualize periampullary/duodenal tumor; assess for bleeding or obstruction |
| ERCP | For biliary decompression or duodenal tumor visualization |
Malignancy & Metastatic Potential
- >70% are malignant at diagnosis
- Metastatic disease to liver, lymph nodes, or bone: 37-90% (correlated with tumor size)
- Most patients are diagnosed with locally advanced and/or metastatic disease due to the nonspecific early symptoms
- Pancreatic somatostatinomas carry a worse prognosis than duodenal ones (larger size, higher metastatic rate)
- Periampullary tumors have a particularly aggressive course
- NF-1-associated tumors: tend to be smaller, more localized at presentation, with minimal hormonal syndrome - better prognosis
Management
1. Medical Management (Preoperative / Palliation)
- Somatostatin analogues (octreotide/lanreotide): Note the irony - while these are used to treat other functional NETs by mimicking somatostatin, their benefit in somatostatinoma is questionable since the tumor already overproduces somatostatin and receptor occupancy may already be near-maximal (Harrison's)
- Diabetes management: Oral hypoglycemics or insulin therapy; often easier to control than expected since glucagon is also inhibited
- Pancreatic enzyme replacement (PERT): For steatorrhea/malabsorption (lipase, protease, amylase supplements)
- Fat-soluble vitamin supplementation (A, D, E, K): Due to malabsorption
- Ursodeoxycholic acid: Consider for biliary management preoperatively
- Nutritional optimization prior to surgery
2. Surgical Management
| Location | Surgical Procedure |
|---|---|
| Pancreatic body/tail | Distal pancreatectomy (± splenectomy) |
| Pancreatic head | Pancreaticoduodenectomy (Whipple procedure) |
| Periampullary/duodenal | Local excision or Whipple if large/involving ampulla |
| All cases | Cholecystectomy (concurrent; cholelithiasis is near-universal and risk of recurrence is high) |
| Liver metastases (resectable) | Synchronous or staged hepatic resection if primary controlled and complete removal feasible |
- Intraoperative ultrasound to confirm tumor location and ductal anatomy
- Regional lymphadenectomy
- Thorough exploration for multifocal disease (suggests MEN-1)
3. Management of Metastatic / Unresectable Disease
| Treatment | Notes |
|---|---|
| Somatostatin analogues | Limited efficacy (tumor already producing excess somatostatin) but may provide antiproliferative benefit |
| PRRT (¹⁷⁷Lu-DOTATATE) | If somatostatin receptor positive (most are); increasingly used |
| Everolimus / Sunitinib | mTOR and VEGFR inhibition for progressive disease |
| Chemotherapy (streptozotocin + 5-FU ± doxorubicin) | For high-grade tumors |
| Hepatic artery embolization / TACE | Liver-dominant metastatic disease |
| RFA / SIRT | Focal or diffuse liver metastases |
| Debulking surgery | Symptomatic relief; may improve quality of life |
Prognosis
- Generally poor due to advanced disease at diagnosis
- 5-year survival for localized disease: ~75%
- 5-year survival with liver metastases: ~15-40%
- Duodenal/NF-1-associated tumors: Better prognosis (smaller, localized)
- Pancreatic/periampullary tumors: Worse prognosis (larger, more metastatic)
- Complete surgical resection offers the best chance of long-term survival
Key Summary
| Feature | Detail |
|---|---|
| Cell of origin | Delta (D) cells |
| Incidence | ~1 per 40 million; rarest functional PNET |
| Classic syndrome | Inhibitory triad: Diabetes + Steatorrhea + Cholelithiasis |
| Sites | Pancreas (~50%) and duodenum (~50%) |
| Mean tumor size | Pancreatic: 5-6 cm; Duodenal: ~2 cm |
| Histological clue | Psammoma bodies in duodenal tumors |
| Diagnostic test | Plasma somatostatin >10 ng/mL + clinical symptoms |
| Malignancy rate | >70% |
| Metastasis at diagnosis | 37-90% |
| MEN-1 association | Present (45% in some series) |
| NF-1 association | Strong (especially duodenal: 43%) |
| Drug of choice | Enzyme replacement + glucose control (somatostatin analogues of limited benefit) |
| Surgery | Resection + mandatory cholecystectomy |
| Somatostatin analogues | Questionable efficacy (tumor already overproduces somatostatin) |