Hi I am preparing for neurosurgery and I want few things from you 1 all important neurosurgeons, few photos of them and their main contribution 2. First give me brief about all imp imaging types like ct t1 t2 mri etc also mr spectroscopy as much as types possible and then u will also give one by one image of specific findings imp in neurosurgery 2to3 pics of each with descriptions 3 instruments used in neurosurgery with pics and descriptions as much as possible and from simple to complex including endoscopes and microscopes also 4 all imp trials in neurosurgery with brief descriptions 5 neuropharmacology with antibiotics used in neurosurgery anti epileptics in neurosurgery anti edema agents , chemotherapy agents in neurosurgery and give me drug class, mechanism of action, side effects, special points and try to add as much as images overall and also use standard books
You are preparing a comprehensive neurosurgery study guide. Your task is to research and compile content for SECTIONS 1, 3, and 4 from medical textbooks and web sources. **SECTION 1: Important Neurosurgeons** Search the medical library database and web for the most important/famous neurosurgeons in history. For each surgeon, provide: - Full name - Era/dates - Country - Main contributions to neurosurgery - One memorable quote or fact - Search for a photo URL using web_search Key surgeons to cover: Harvey Cushing, Walter Dandy, Victor Horsley, Wilder Penfield, Charles Drake, M. Gazi Yaşargil, Henry Marsh, Atul Gawande, Alexi Marneffe, Franc Grigsby, Dorcas Osei, Peter Nakaji, Alfredo Quinones-Hinojosa, Bennie Oshowoyo, Julian Wu. Also include any other major figures. Use web_search to find photos - search "[surgeon name] neurosurgeon photo" and get image URLs. **SECTION 3: Neurosurgery Instruments** Search web_search and query_library_db for neurosurgery instruments. Cover ALL of these categories with descriptions: BASIC/SIMPLE: - Scalpel (No. 15, 22 blades), scissors (Metzenbaum, Mayo) - Retractors (Weitlaner, Cerebellar, Leyla bar/arm) - Forceps (Gerald, Cushing, Bayonet bipolar) - Needle holders, hemostats - Periosteal elevators (Penfield elevators #1-5, Langenbeck) BONE INSTRUMENTS: - Craniotome/Midas Rex drill - Kerrison rongeurs, Leksell rongeurs - Gigli saw, bone curettes - Hudson brace SPECIALTY NEUROSURGICAL: - Bipolar forceps (Malis, Rhoton) - Cottonoid patties, hemostatic agents (Gelfoam, Surgicel) - Brain retractors (Taylor, Greenberg system) - Aneurysm clips (Yasargil, Sugita types) - Clip applier ENDOSCOPES: - Rigid endoscope (0°, 30°, 70° scopes) - Neuroendoscope for EVD/ETV - Endoscopic third ventriculostomy instruments MICROSCOPES: - Operating microscope (Zeiss OPMI, Leica OH6) - Exoscope (ORBEYE, KINEVO) For each instrument, provide name, description, use in neurosurgery, and search for image URL via web_search. **SECTION 4: Important Clinical Trials in Neurosurgery** Search query_library_db using: SELECT book_title, section_heading, '/textbooks/' || block_file_path AS file_path, line_start, line_end, snippet(paragraphs_fts, 0, '>>>', '<<<', '...', 40) as snippet FROM paragraphs_fts WHERE paragraphs_fts MATCH 'clinical trial neurosurgery' ORDER BY rank LIMIT 10 Also use web_search for "important clinical trials neurosurgery" and cover: 1. ISAT trial (aneurysm clipping vs coiling) 2. STICH trial (intracerebral hemorrhage surgery) 3. STICH II trial 4. DESTINY trial (decompressive craniectomy stroke) 5. DECIMAL trial 6. RESCUEicp trial (decompressive craniectomy TBI) 7. CRASH trial (steroids TBI) 8. IMPACT trial (TBI prognostication) 9. RTOG 9402 / EORTC 26951 (oligodendroglioma) 10. MGMT methylation and temozolomide trials (Stupp protocol) 11. SPRINT trial / EVT trials (thrombectomy - DAWN, DEFUSE 3) 12. SPORT trial (spine surgery) 13. ACST trial (carotid endarterectomy) 14. CREST trial 15. SANTE trial (DBS for epilepsy) 16. NEJM trials on IDH glioma For each trial: full name, year, design, key finding, clinical impact. Return a well-structured markdown document with all three sections fully populated. Include any image URLs you found for instruments and surgeons.
Harvey Cushing neurosurgeon photo portrait
Walter Dandy neurosurgeon photo portrait
M. Gazi Yasargil neurosurgeon photo portrait
Victor Horsley neurosurgeon photo portrait history
Wilder Penfield neurosurgeon photo portrait
Alfredo Quinones-Hinojosa neurosurgeon photo
Henry Marsh neurosurgeon photo portrait
Charles Drake neurosurgeon photo portrait aneurysm
Atul Gawande neurosurgeon surgeon photo portrait
neurosurgery bipolar forceps Malis Rhoton photo instrument
Kerrison rongeur neurosurgery instrument photo
Yasargil aneurysm clip neurosurgery instrument photo
Zeiss OPMI operating microscope neurosurgery photo
craniotome Midas Rex drill neurosurgery instrument photo
important clinical trials neurosurgery DESTINY DECIMAL RESCUEicp CRASH
Peter Nakaji neurosurgeon Arizona photo
neuroendoscope rigid endoscope 0 degree 30 degree neurosurgery photo
Penfield dissector elevator neurosurgery instruments set photo
ISAT trial 2002 results aneurysm coiling clipping key findings summary
MGMT methylation Stupp protocol temozolomide glioblastoma EORTC NCIC trial 2005 key findings
ORBEYE exoscope neurosurgery photo 3D 4K
DESTINY DECIMAL trial decompressive craniectomy malignant MCA infarction results findings
SANTE trial deep brain stimulation anterior nucleus thalamus epilepsy results
ACST trial asymptomatic carotid stenosis endarterectomy results 2004
Greenberg brain retractor system neurosurgery instrument photo
cottonoid patties Gelfoam Surgicel hemostatic neurosurgery operating room photo
Gigli saw Hudson brace neurosurgery craniotomy instrument photo
Leksell rongeur neurosurgery spine instrument photo
CREST trial carotid endarterectomy stenting results 2010 key findings
RTOG 9402 EORTC 26951 oligodendroglioma PCV chemotherapy 1p19q codeletion results
IMPACT trial TBI traumatic brain injury prognostication outcomes model results
Weitlaner self-retaining retractor cerebellar retractor neurosurgery instrument photo
bayonet bipolar forceps Gerald forceps Cushing forceps neurosurgery photo
famous neurosurgeons history contributions Harvey Cushing Walter Dandy Yaşargil comprehensive
STICH trial 2005 intracerebral haemorrhage surgery conservative results Mendelow
Hi I am preparing for neurosurgery First give me brief about all imp imaging types like ct t1 t2 mri etc also mr spectroscopy as much as types possible and then u will also give one by one image of specific findings imp in neurosurgery 2to3 pics of each with descriptions
CT brain hemorrhage hyperdense neurosurgery
MRI T1 T2 brain tumor glioma
MR spectroscopy brain tumor choline NAA creatine peaks
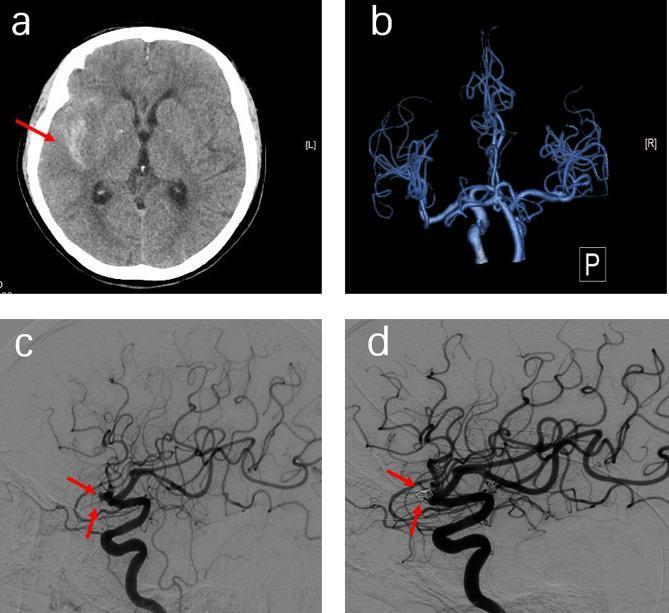
CT angiography cerebral aneurysm subarachnoid hemorrhage
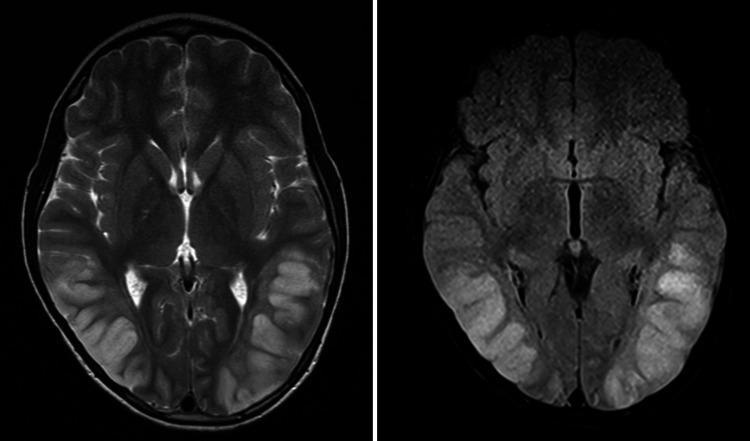
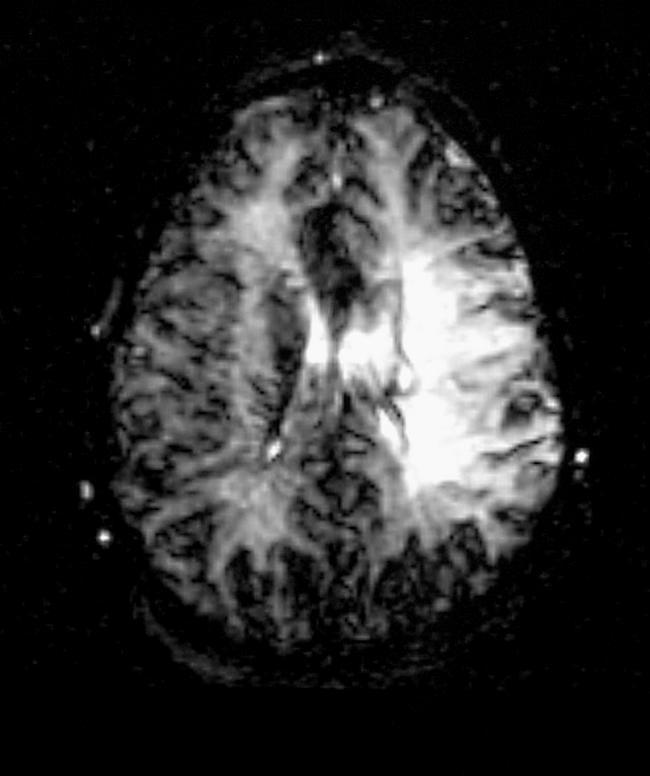
DWI diffusion weighted MRI acute stroke ischemic infarct bright ADC dark
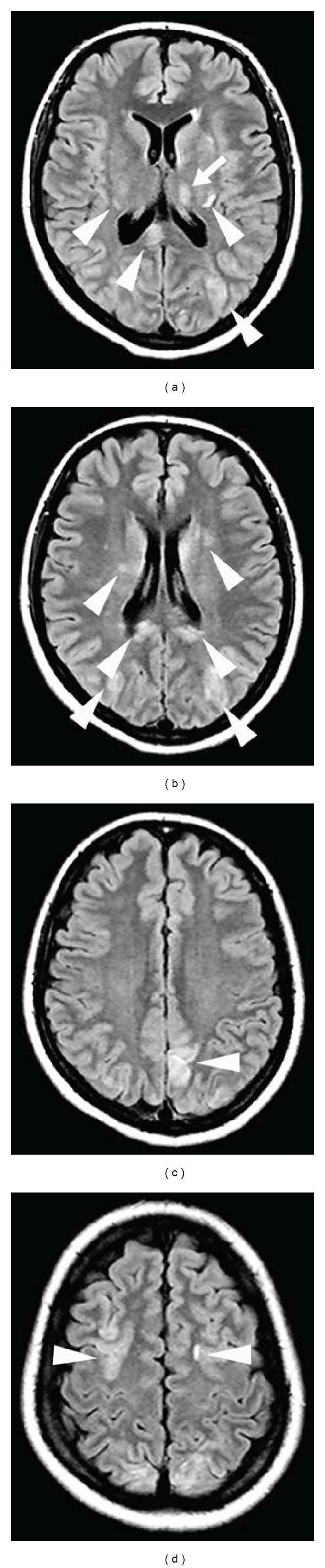
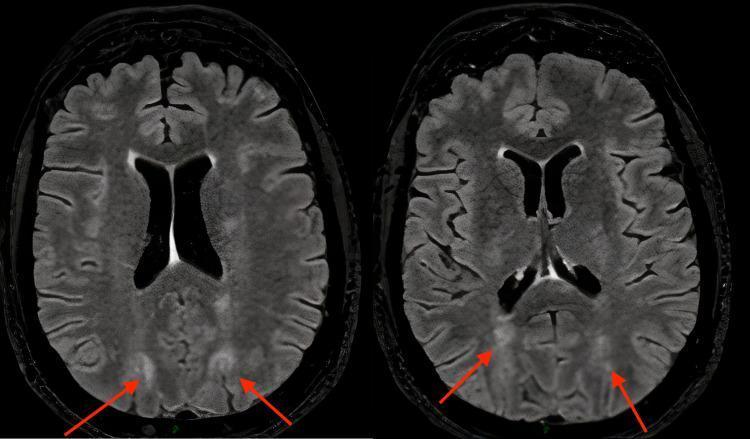
FLAIR MRI white matter hyperintensity edema brain
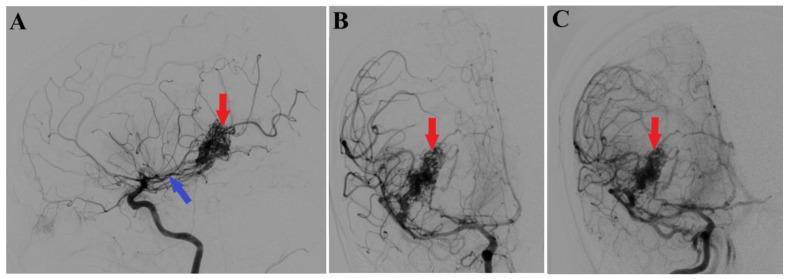
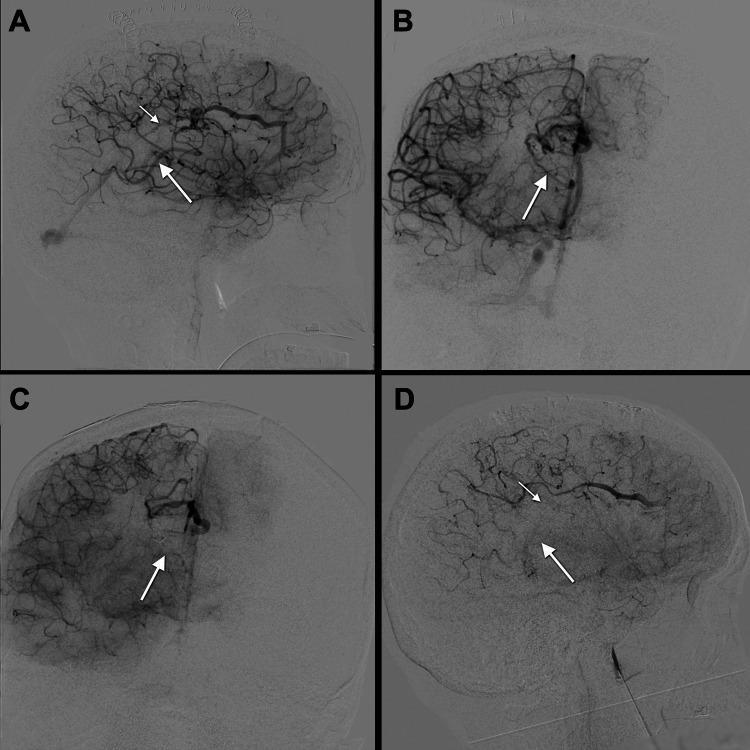
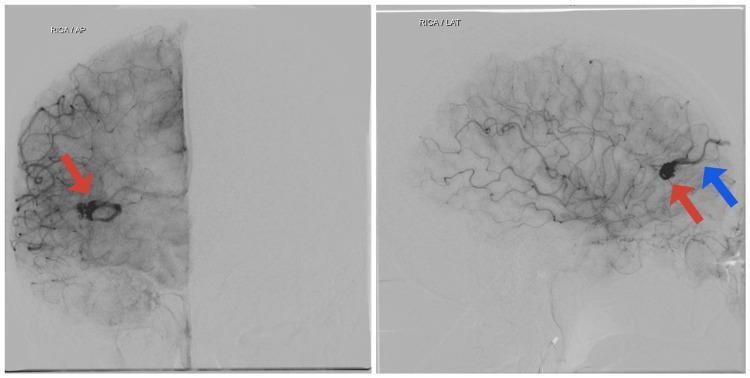
cerebral angiography DSA digital subtraction AVM arteriovenous malformation
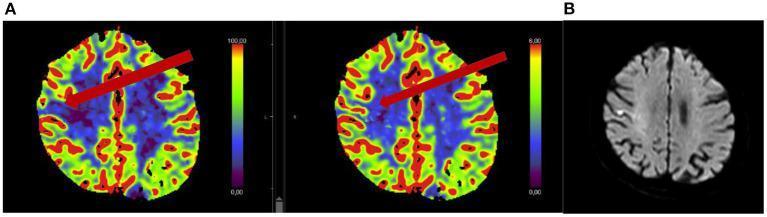
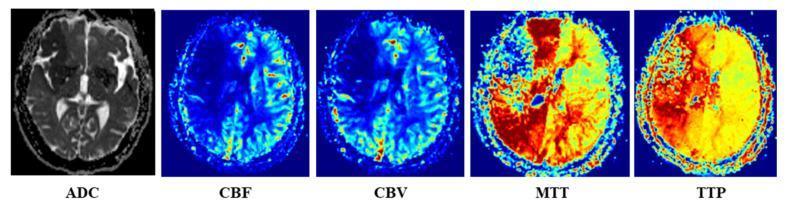
MRI perfusion PWI cerebral blood flow volume ischemia penumbra
subdural hematoma epidural hematoma CT crescent biconvex lens
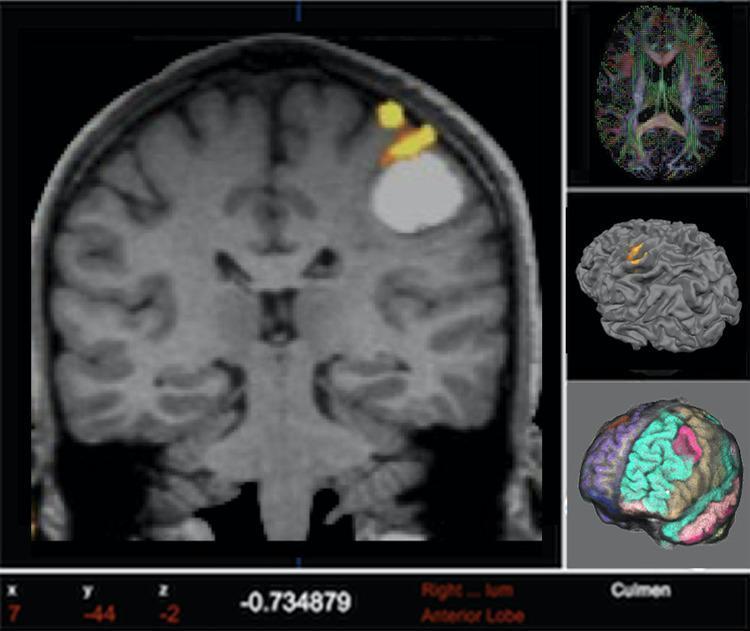
functional MRI fMRI DTI tractography brain neurosurgery planning
🧠 NEUROIMAGING FOR NEUROSURGERY — Complete Guide
PART 1: ALL IMPORTANT IMAGING MODALITIES
1. 🔬 COMPUTED TOMOGRAPHY (CT)
| Tissue | HU Value |
|---|---|
| Air | −1000 |
| Fat | −100 to −50 |
| Water/CSF | 0 |
| White matter | 20–30 |
| Grey matter | 35–45 |
| Acute blood | 50–80 (hyperdense) |
| Bone/calcification | 400–1000 |
| Type | Use |
|---|---|
| Non-contrast CT (NCCT) | First-line for trauma, hemorrhage, hydrocephalus |
| CT with IV contrast | Tumors, abscesses, vascular lesions |
| CT Angiography (CTA) | Aneurysms, AVM, vessel occlusion |
| CT Venography (CTV) | Dural sinus thrombosis, venous anomalies |
| CT Perfusion (CTP) | Stroke penumbra, vasospasm after SAH |
| CT Myelography | Spinal cord compression (when MRI contraindicated) |
| 3D CT reconstruction | Craniosynostosis, skull base planning |
Disadvantages: Radiation, inferior soft tissue contrast vs MRI, poor posterior fossa detail (beam hardening)
2. 🧲 MAGNETIC RESONANCE IMAGING (MRI)
2A. T1-WEIGHTED MRI
| Signal | Appears |
|---|---|
| Bright (hyperintense) | Fat, subacute blood (met-Hb), contrast-enhancing tissue, melanin, protein-rich fluid, calcification (sometimes) |
| Dark (hypointense) | Water, CSF, acute blood (deoxy-Hb), cortical bone, air |
- Anatomy delineation (grey-white differentiation)
- Post-contrast T1: tumor enhancement (BBB breakdown), abscesses, meningitis
- Pre-contrast T1: subacute hemorrhage (bright), lipoma, dermoid
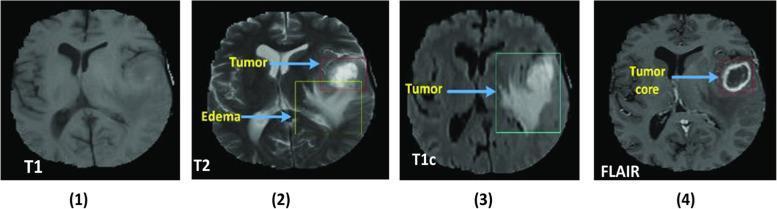
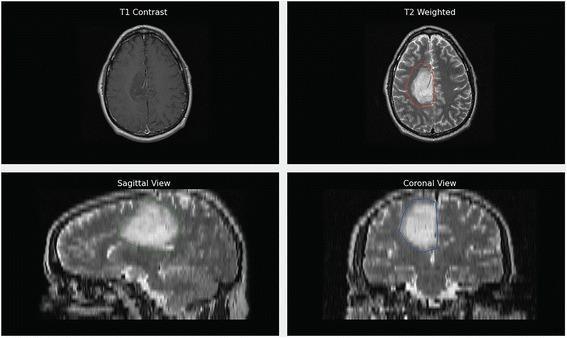
- High-grade glioma (ring enhancement)
- Metastases
- Meningioma (homogeneous enhancement + dural tail)
- Pituitary adenoma
2B. T2-WEIGHTED MRI
| Signal | Appears |
|---|---|
| Bright (hyperintense) | CSF, edema, tumor, inflammation, demyelination, chronic infarct |
| Dark (hypointense) | Cortical bone, air, calcification, acute/chronic blood (hemosiderin), flow voids |
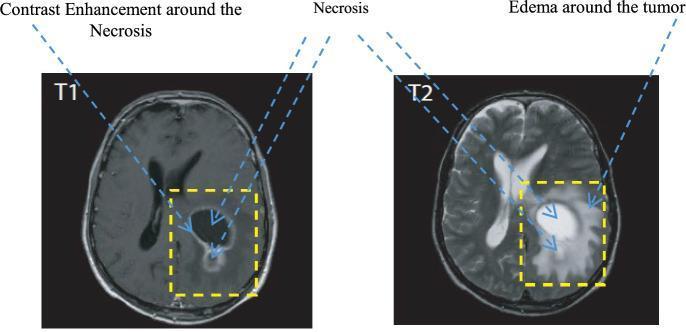
- Edema around tumors (bright halo)
- Low-grade glioma (diffusely bright, no enhancement)
- MS plaques
- Cord signal changes in myelopathy
2C. FLAIR (Fluid-Attenuated Inversion Recovery)
- Periventricular MS plaques (invisible on T2 due to adjacent CSF)
- SAH (blood in cisterns — hyperintense on FLAIR)
- Cortical/subcortical infarcts
- Meningeal carcinomatosis
- Encephalitis, PRES (Posterior Reversible Encephalopathy Syndrome)
2D. GRE / T2* (Gradient Echo)
| Finding | Appearance |
|---|---|
| Hemosiderin (old blood) | Very dark "blooming" artifact |
| Microbleeds | Small dark foci |
| Calcification | Dark |
2E. SWI (Susceptibility Weighted Imaging)
- Cavernous malformations
- Diffuse axonal injury (DAI) microhemorrhages
- Venous structures
- Tumor microvascularity / blood products
- Iron deposition in Parkinson's, Huntington's
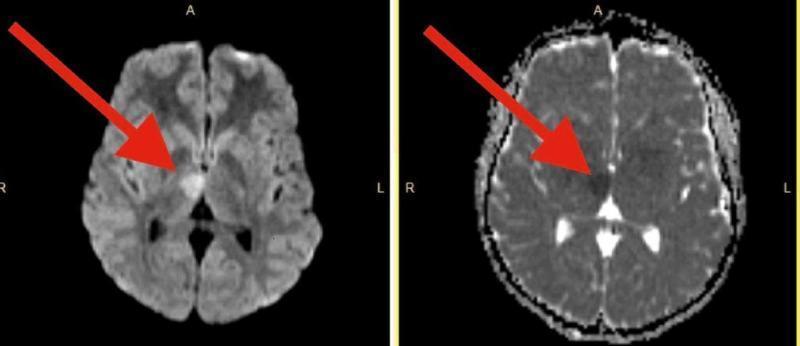
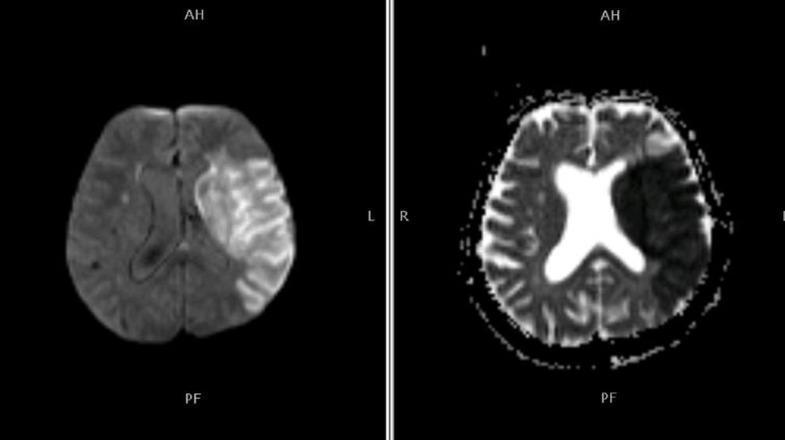
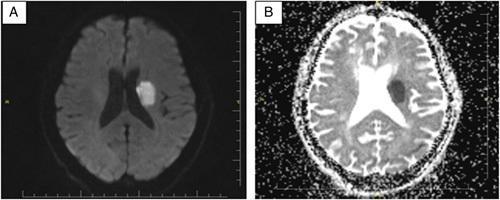
2F. DWI (Diffusion Weighted Imaging) + ADC Map
| Finding | DWI | ADC Map |
|---|---|---|
| Acute infarct (cytotoxic edema) | Bright | Dark (restricted diffusion) |
| T2 shine-through | Bright | Normal/bright |
| Vasogenic edema/necrosis | Dark/normal | Bright (facilitated diffusion) |
| Abscess | Bright (pus is viscous) | Dark |
| Epidermoid cyst | Bright | Dark |
2G. PWI (Perfusion Weighted Imaging)
- CBF — Cerebral Blood Flow (mL/100g/min)
- CBV — Cerebral Blood Volume (mL/100g)
- MTT — Mean Transit Time
- TTP — Time to Peak
- Stroke: define core (dead) vs penumbra (salvageable)
- Tumor grading: high CBV → high-grade glioma
- Post-op vasospasm assessment after SAH
2H. MRA (MR Angiography)
| Type | Principle | Use |
|---|---|---|
| Time-of-Flight (TOF) MRA | Flowing blood gives signal without contrast | Intracranial arteries, Circle of Willis, aneurysm screening |
| Contrast-enhanced MRA | Gadolinium bolus | Neck vessels, AVM, fistula |
| Phase-contrast MRA | Velocity encoding | CSF flow, venous flow |
2I. MRV (MR Venography)
2J. DTI (Diffusion Tensor Imaging) & Tractography
- Corticospinal tract (CST) localization before motor area surgery
- Arcuate fasciculus — language pathway
- Optic radiation — before temporal lobe surgery (Meyer's loop)
- Relationship of tumor to eloquent tracts
2K. fMRI (Functional MRI) — BOLD
- Hand tapping → motor cortex
- Word generation → Broca's area
- Visual tasks → occipital cortex
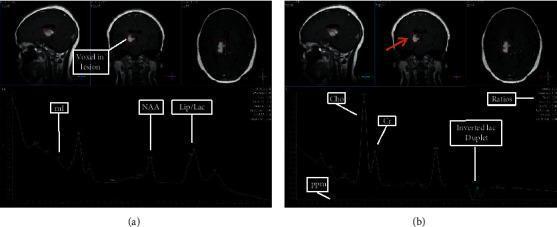
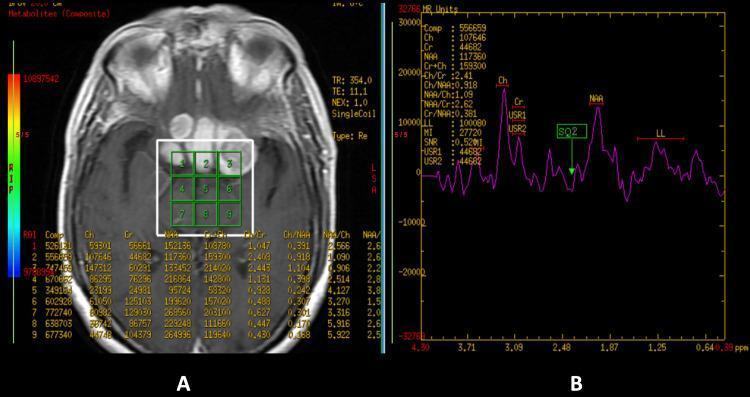
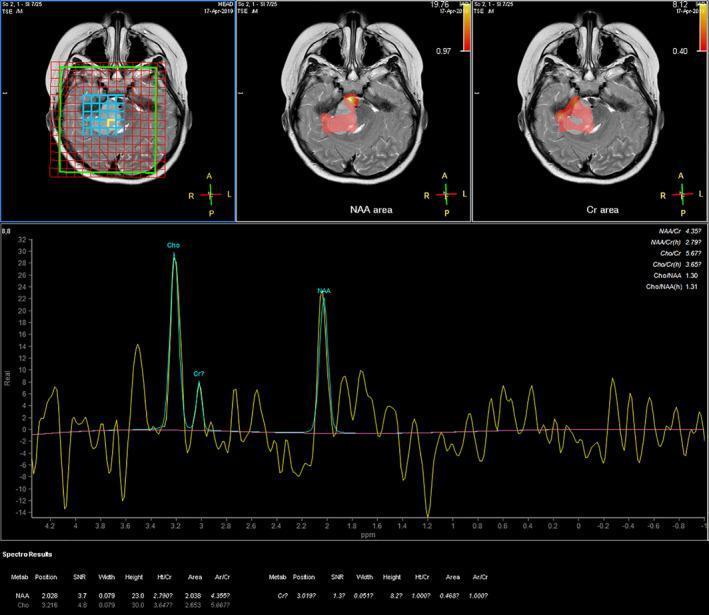
2L. MR SPECTROSCOPY (MRS)
| Metabolite | Chemical shift (ppm) | Normal role | Significance |
|---|---|---|---|
| NAA (N-acetylaspartate) | 2.0 ppm | Neuronal marker | ↓ in neuronal loss, tumor, infarct |
| Cho (Choline) | 3.2 ppm | Cell membrane turnover | ↑ in tumors, demyelination |
| Cr (Creatine) | 3.0 ppm | Energy metabolism (reference) | Relatively stable |
| Lac (Lactate) | 1.3 ppm (doublet) | Anaerobic glycolysis | ↑ in necrosis, high-grade tumor, infarct |
| Lip (Lipid) | 0.9, 1.3 ppm | Cell membrane breakdown | ↑ in necrosis |
| mI (Myo-inositol) | 3.5 ppm | Glial marker | ↑ low-grade glioma, ↑ Alzheimer's |
| Glu/Gln | 2.1–2.4 ppm | Neurotransmitters | ↑ hepatic encephalopathy |
| Alanine | 1.47 ppm (inverted doublet) | — | Characteristic of meningioma |
| Diagnosis | Pattern |
|---|---|
| High-grade glioma | ↑↑ Cho, ↓ NAA, ↑ Lip/Lac, ↑ Cho:NAA |
| Low-grade glioma | ↑ Cho, ↓ NAA, ↑ mI |
| Radiation necrosis | ↓ all metabolites (metabolic void) — distinguish from tumor recurrence |
| Meningioma | ↑ Cho, absent Cr, Alanine peak |
| Metastasis | ↑ Cho, ↓ NAA, ↑ Lip/Lac |
| Abscess | ↑ amino acids, succinate, acetate, lactate |
| Medulloblastoma | ↑ Cho, ↓ NAA, taurine peak |
- Short TE (20–35 ms): sees all metabolites including mI, Lip
- Intermediate TE (135–144 ms): lactate inverts (doublet pointing down), fewer metabolites
2M. MRI SPINE
| Sequence | Use |
|---|---|
| T1 sagittal | Normal anatomy, fat (bright), tumor signal |
| T2 sagittal | CSF (bright), cord signal changes |
| STIR | Suppresses fat — bone marrow edema, tumor |
| Post-contrast T1 | Enhancement in infection, tumor, cord lesion |
| Myelogram sequence (CISS/FIESTA) | CSF detail, nerve root compression |
2N. PET SCAN (Positron Emission Tomography)
| Tracer | Use |
|---|---|
| ¹⁸F-FDG | Glucose metabolism — tumor vs necrosis, epilepsy foci |
| ¹¹C-MET / ¹⁸F-FET | Amino acid — glioma grading, extent of infiltration |
| ¹¹C-PIB / ¹⁸F-AV45 | Amyloid — Alzheimer's workup |
| ¹⁸F-DOPA | Dopamine — Parkinson's, paraganglioma |
2O. Digital Subtraction Angiography (DSA)
- Aneurysm characterization (size, neck, orientation)
- AVM grading (Spetzler-Martin)
- Dural AV fistula
- Vasospasm after SAH (also therapeutic — papaverine, angioplasty)
- Pre-op embolization planning
- Post-op aneurysm clip/coil confirmation
2P. Intraoperative Imaging
| Modality | Use |
|---|---|
| Intraoperative ultrasound | Real-time tumor localization, hematoma |
| Intraoperative CT (O-arm, Airo) | Pedicle screw position, extent of resection |
| Intraoperative MRI (iMRI) | Maximize glioma resection, avoid eloquent cortex |
| 5-ALA fluorescence | Highlights high-grade glioma (pink/red under UV) |
| Sodium fluorescein | Enhancing tumor visualization (yellow-green) |
| ICG (indocyanine green) videoangiography | Vessel patency during aneurysm/AVM surgery |
PART 2: KEY NEUROSURGICAL IMAGING FINDINGS WITH IMAGES
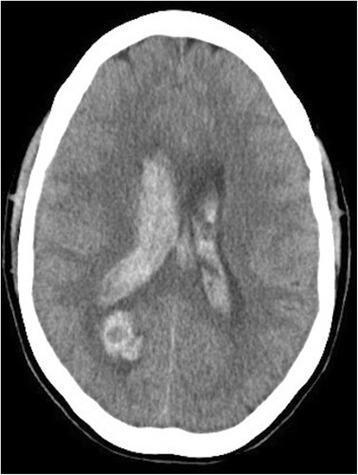
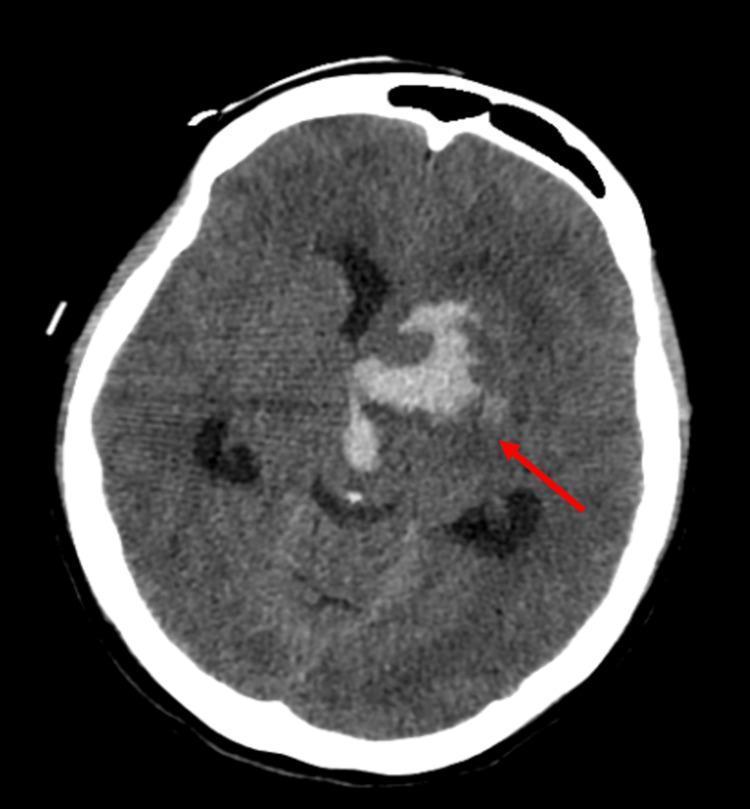
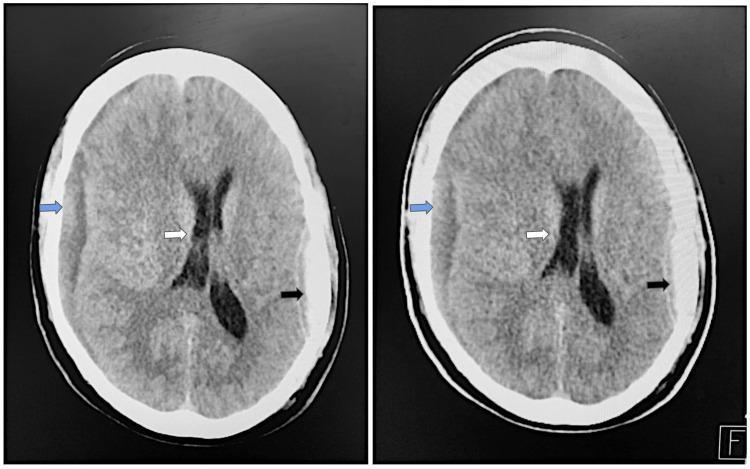
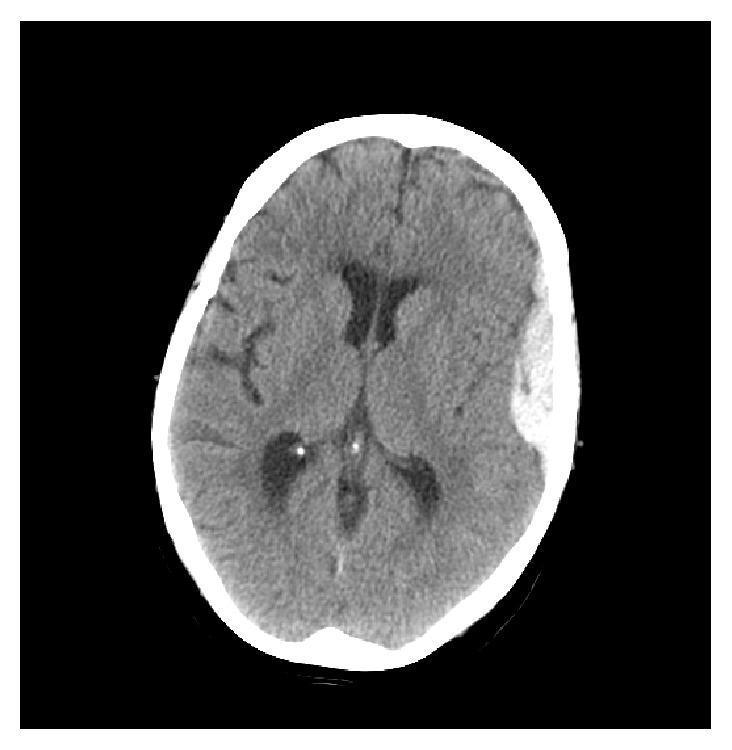
📸 FINDING 1: ACUTE INTRACRANIAL HEMORRHAGE (Non-contrast CT)
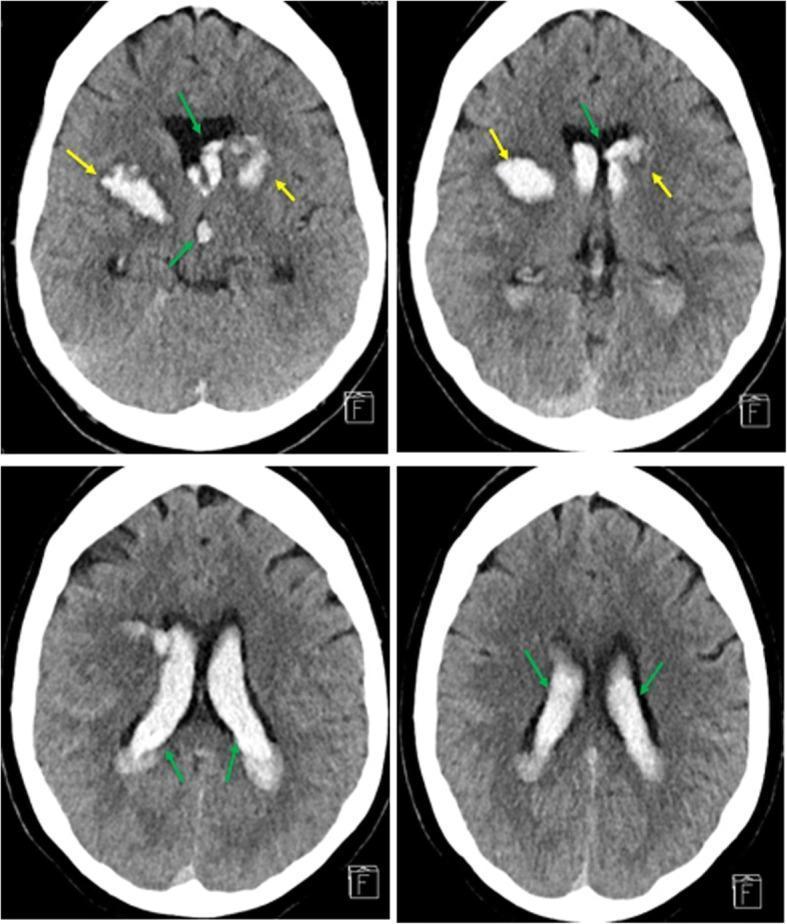
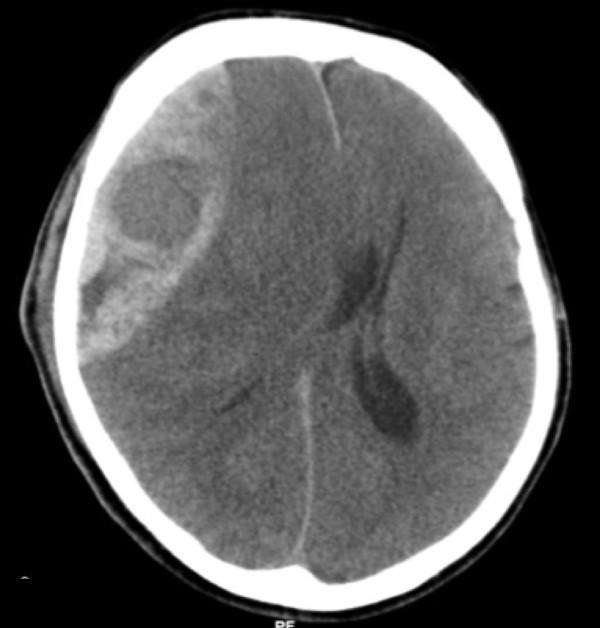
📸 FINDING 2: EPIDURAL vs SUBDURAL HEMATOMA (CT)
SDH: Crescent-shaped, crosses sutures, follows brain surface, venous (bridging veins), often elderly/anticoagulated
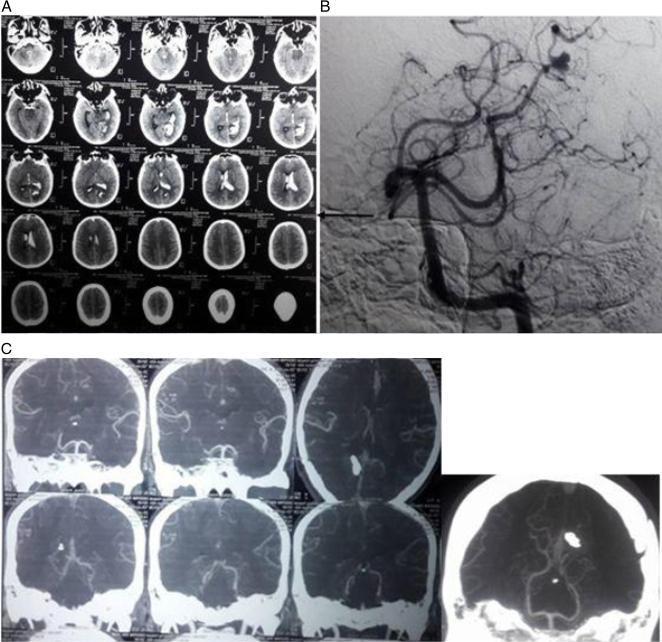
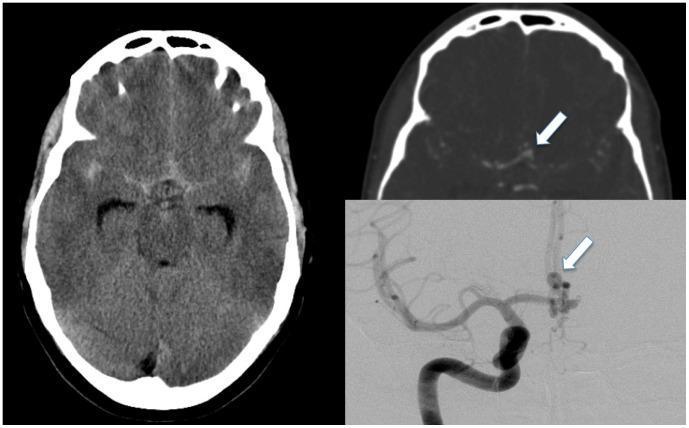
📸 FINDING 3: SUBARACHNOID HEMORRHAGE (SAH) + ANEURYSM
📸 FINDING 4: BRAIN TUMOR — MRI (T1, T2, FLAIR, T1+Gd)
Low-grade glioma: T2/FLAIR bright, NO enhancement, NO necrosis
📸 FINDING 5: DWI/ADC — ACUTE ISCHEMIC STROKE
📸 FINDING 6: MR SPECTROSCOPY — BRAIN TUMORS
📸 FINDING 7: DSA — CEREBRAL AVM (Arteriovenous Malformation)
📸 FINDING 8: FLAIR — POSTERIOR REVERSIBLE ENCEPHALOPATHY SYNDROME (PRES) + White Matter Disease
📸 FINDING 9: PERFUSION MRI / CT — STROKE PENUMBRA
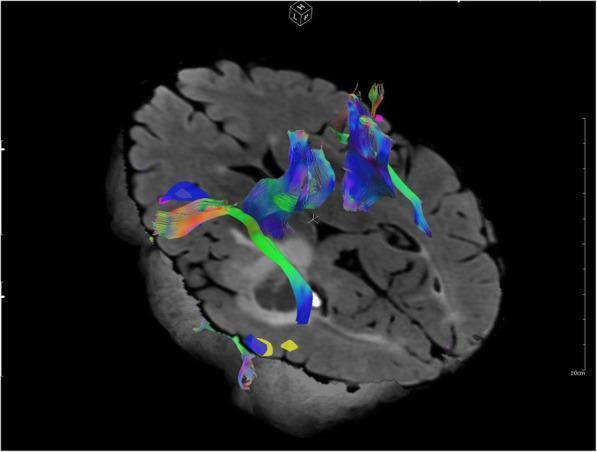
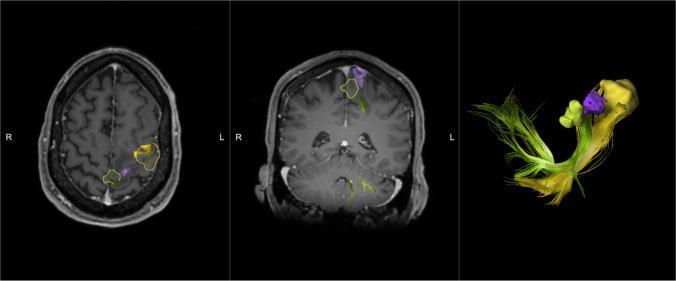
📸 FINDING 10: fMRI + DTI TRACTOGRAPHY — PRE-OPERATIVE PLANNING
QUICK REFERENCE: IMAGING FIRST-LINE CHOICE IN NEUROSURGERY
| Clinical Scenario | First-Line Imaging | Next Step |
|---|---|---|
| Acute head trauma | NCCT head | CTA if vascular injury suspected |
| Acute stroke <24h | NCCT + CT perfusion or DWI MRI | CTA for LVO, angiography for EVT |
| Suspected aneurysm/SAH | NCCT → CTA | DSA if CTA negative |
| Brain tumor evaluation | MRI T1/T2/FLAIR/T1+Gd | MRS, fMRI, DTI for planning |
| AVM characterization | MRI → DSA | 4D-DSA for flow dynamics |
| Tumor vs radiation necrosis | MRS + FDG-PET or MET-PET | Perfusion MRI (CBV) |
| Spinal cord compression | MRI T1/T2 spine | |
| Pre-op eloquent cortex | fMRI + DTI tractography | Awake craniotomy + IONM |
| Abscess vs necrotic tumor | DWI (abscess = bright DWI, dark ADC) | MRS (amino acids = abscess) |
| Cavernous malformation | SWI/GRE (blooming) | T2 "popcorn" lesion |