Cns physiology upto tract 1st year mbbs
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Here is a complete, structured CNS physiology guide for 1st year MBBS, covering up to spinal cord tracts, sourced from Gray's Anatomy for Students and Principles of Neural Science.
CNS Physiology - 1st Year MBBS (Up to Tracts)
1. Organization of the Nervous System
The nervous system is divided into two main structural divisions:
- Central Nervous System (CNS): Brain + Spinal cord
- Peripheral Nervous System (PNS): Cranial nerves, spinal nerves, and their ganglia
Functionally, it is divided into:
- Somatic nervous system: Voluntary control of skeletal muscle; conscious sensory input
- Autonomic nervous system (ANS): Involuntary control of visceral organs (sympathetic and parasympathetic)
2. The Neuron - Basic Unit of the CNS
Structure
A neuron has four main parts:
- Dendrites - receive incoming signals
- Cell body (soma) - contains nucleus, metabolic center
- Axon (nerve fiber) - conducts impulses away from the soma
- Axon terminals (synaptic boutons) - transmit signals to the next cell
Types of Neurons (by function)
| Type | Function |
|---|---|
| Sensory (afferent) | Carry impulses toward CNS |
| Motor (efferent) | Carry impulses away from CNS |
| Interneurons | Relay between sensory and motor neurons (most common in CNS) |
Glia (Supporting Cells)
| Cell | Location | Function |
|---|---|---|
| Astrocytes | CNS | Blood-brain barrier, metabolic support |
| Oligodendrocytes | CNS | Myelin sheath formation |
| Schwann cells | PNS | Myelin sheath formation |
| Microglia | CNS | Immune defense |
| Ependymal cells | CNS | Line ventricles, CSF production |
3. Resting Membrane Potential (RMP)
- Value: -70 mV (inside negative relative to outside)
- Maintained by:
- High intracellular K+ (maintained by Na+/K+ ATPase pump - 3 Na+ out, 2 K+ in)
- High extracellular Na+
- Negatively charged intracellular proteins
- Selective permeability (resting membrane more permeable to K+ than Na+)
Key ions and their equilibrium potentials:
- K+: -90 mV (favors hyperpolarization)
- Na+: +60 mV (favors depolarization)
4. Action Potential (AP)
The action potential is an all-or-none electrical signal transmitted along an axon.
Phases
- Resting (-70 mV): Voltage-gated Na+ and K+ channels are closed
- Depolarization: Stimulus reaches threshold (~-55 mV), Na+ channels open rapidly → Na+ rushes in → membrane potential rises to ~+30 mV
- Repolarization: Na+ channels inactivate; K+ channels open → K+ flows out → membrane returns toward -70 mV
- Hyperpolarization (after-potential): K+ channels briefly over-correct → membrane dips below -70 mV
- Return to resting: Na+/K+ pump restores ionic balance
Key Concepts
- Threshold: ~-55 mV; below this, AP will not fire
- All-or-none law: Either fires fully or not at all
- Absolute refractory period: No AP possible (Na+ channels inactivated)
- Relative refractory period: AP possible with suprathreshold stimulus
- Saltatory conduction: In myelinated fibers, AP "jumps" between Nodes of Ranvier → faster conduction
Conduction velocity depends on:
- Myelination (increases speed greatly)
- Axon diameter (larger = faster)
5. Synapse and Synaptic Transmission
Structure
- Presynaptic terminal: Contains synaptic vesicles filled with neurotransmitters
- Synaptic cleft: ~20-40 nm gap
- Postsynaptic membrane: Contains receptors
Mechanism (Chemical Synapse)
- AP arrives at presynaptic terminal
- Voltage-gated Ca2+ channels open → Ca2+ flows in
- Synaptic vesicles fuse with membrane (exocytosis) → neurotransmitter released
- NT binds to postsynaptic receptors → ion channels open
- Generates either EPSP or IPSP
- NT removed by reuptake, enzymatic degradation, or diffusion
EPSP vs IPSP
| EPSP | IPSP | |
|---|---|---|
| Full form | Excitatory postsynaptic potential | Inhibitory postsynaptic potential |
| Effect | Depolarization (makes AP more likely) | Hyperpolarization (makes AP less likely) |
| Example NT | Glutamate, acetylcholine | GABA, glycine |
Summation
- Temporal summation: Repeated stimuli from same neuron add up over time
- Spatial summation: Multiple synapses fire simultaneously → effects add up
6. Neurotransmitters (Key ones for 1st year)
| Neurotransmitter | Location | Effect |
|---|---|---|
| Acetylcholine (ACh) | NMJ, ANS, basal forebrain | Excitatory (NMJ); variable in CNS |
| Glutamate | CNS (widespread) | Major excitatory NT |
| GABA | CNS (widespread) | Major inhibitory NT |
| Glycine | Spinal cord | Inhibitory |
| Dopamine | Basal ganglia, limbic system | Modulator (reward, movement) |
| Serotonin | Raphe nuclei | Modulator (mood, sleep) |
| Norepinephrine | Locus coeruleus, ANS | Excitatory/modulatory |
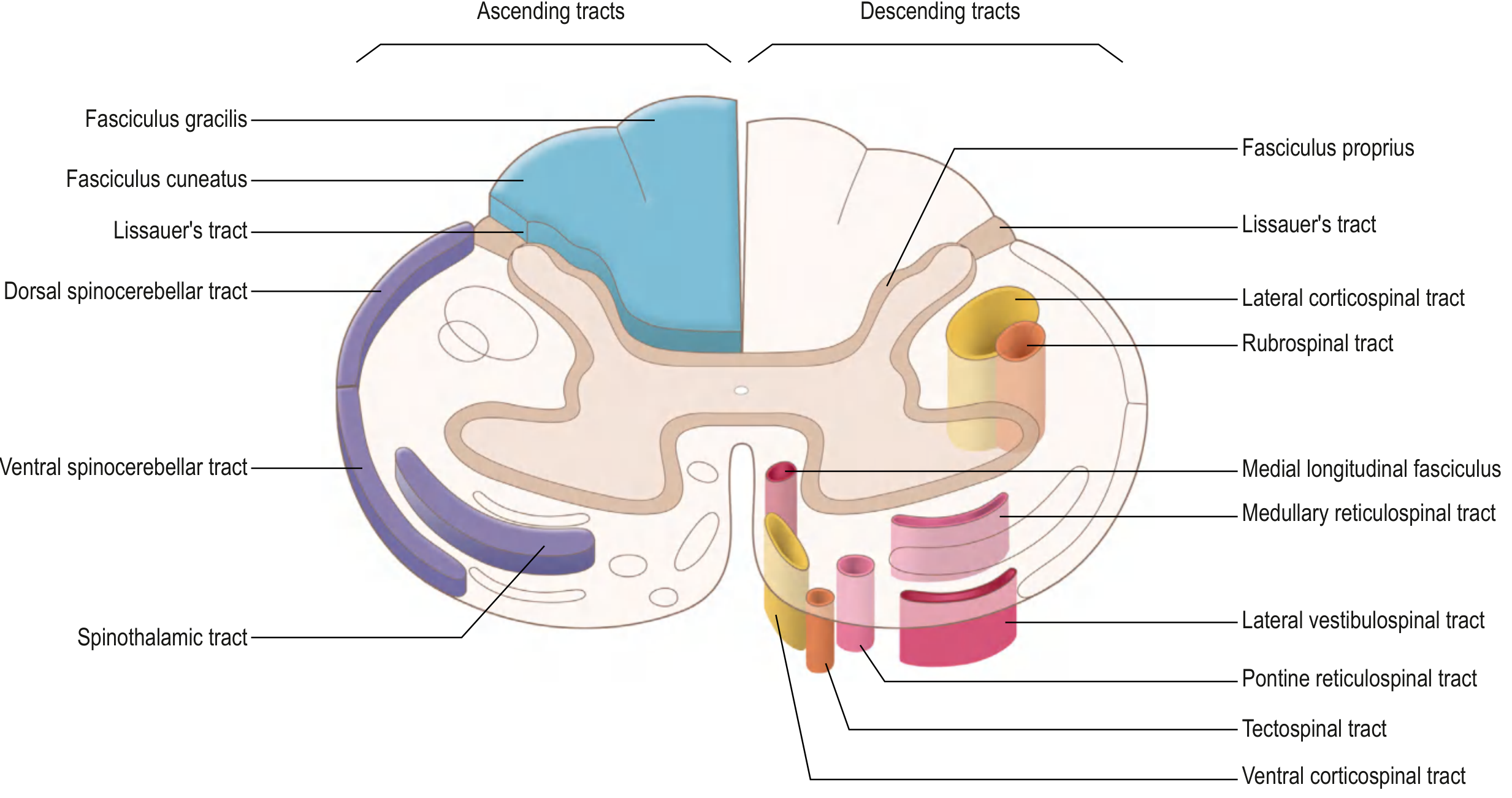
7. The Spinal Cord - Structure
The spinal cord extends from the foramen magnum to the conus medullaris at ~L1/L2 vertebral level.
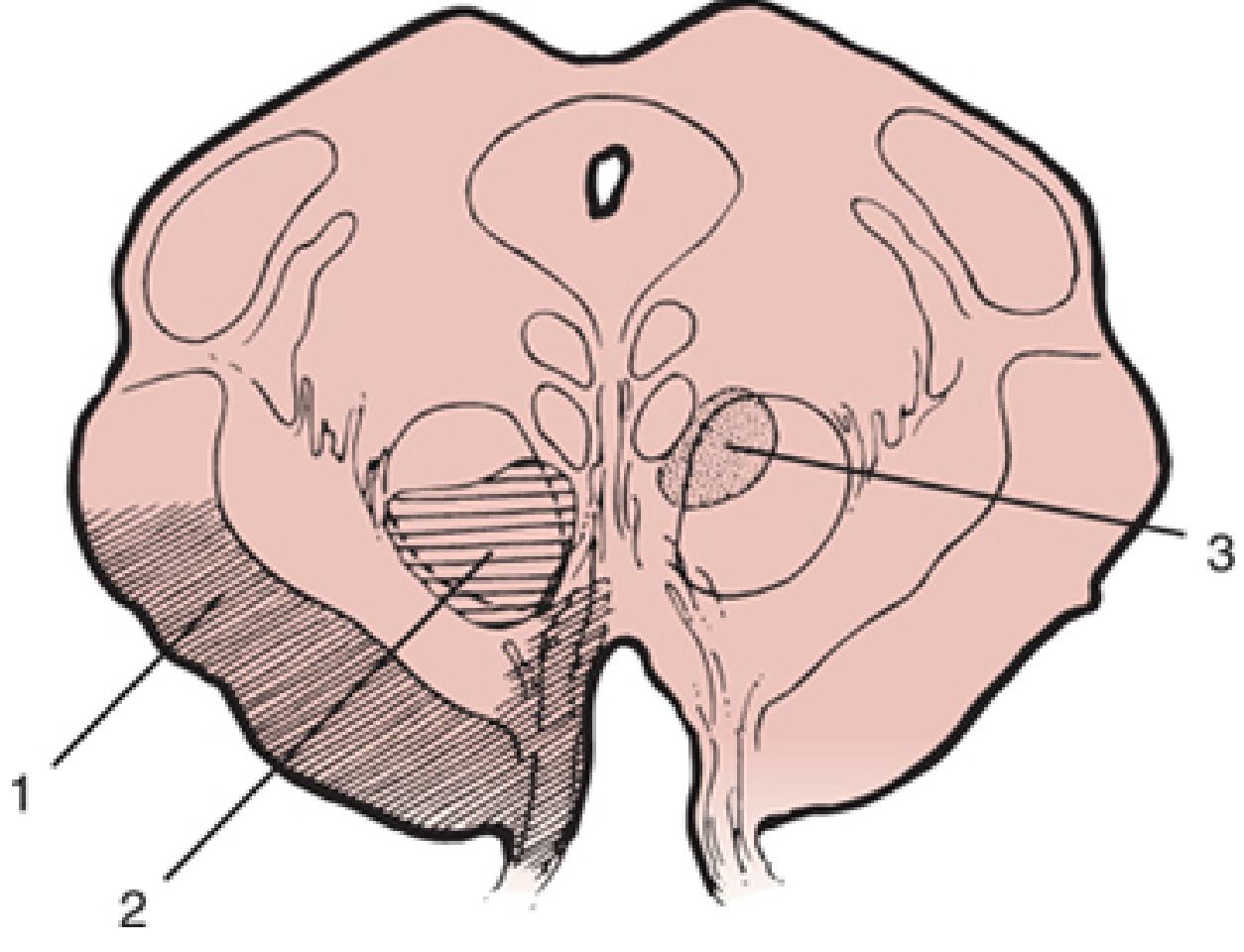
Cross-section anatomy
- Gray matter (H-shaped): Contains neuron cell bodies
- Anterior horn: Motor neurons (lower motor neurons - LMN)
- Posterior horn: Sensory relay neurons
- Lateral horn (T1-L2): Preganglionic sympathetic neurons; (S2-S4): Parasympathetic
- White matter: Contains myelinated axons organized into funiculi (columns)
- Posterior funiculus (dorsal column): Ascending sensory tracts
- Lateral funiculus: Mix of ascending and descending tracts
- Anterior funiculus: Mainly descending motor tracts
Rexed's Laminae
The gray matter is organized into 10 layers (laminae I-X). For 1st year, key ones:
- Laminae I, II (substantia gelatinosa): Pain and temperature processing
- Laminae III, IV: Touch, pressure
- Lamina V: Wide dynamic range neurons
- Lamina IX: Alpha and gamma motor neurons
- Lamina X: Surrounds the central canal
8. ASCENDING TRACTS (Sensory Pathways)
All conscious somatosensory pathways use a 3-neuron relay to reach the cortex.
A. Anterolateral System (Spinothalamic Tract)
Sensation carried: Pain, temperature, crude touch, pressure
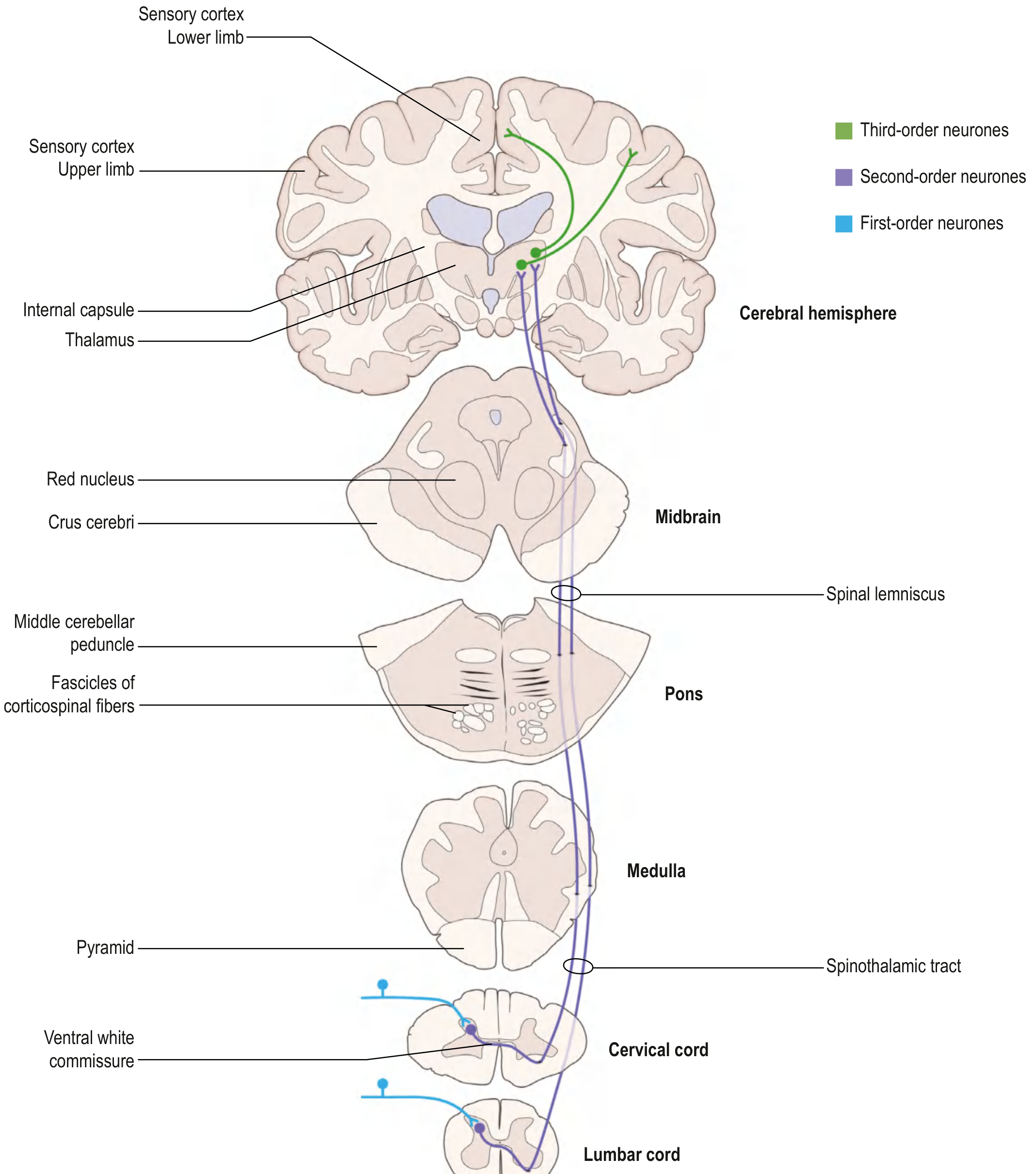
Pathway:
- 1st order neuron: Cell body in dorsal root ganglion (DRG) → enters spinal cord through posterior root → travels in Lissauer's tract (posterolateral fasciculus) for 1-2 segments → synapses in posterior horn (laminae I and V)
- 2nd order neuron: Axon crosses obliquely via anterior white commissure over 2-3 spinal segments to the contralateral side → ascends as the anterolateral (spinothalamic) tract → synapses in VPL nucleus of thalamus
- 3rd order neuron: From thalamus → through posterior limb of internal capsule → primary somatosensory cortex (postcentral gyrus)
Key point: Crosses at the spinal cord level (2-3 segments above entry) → contralateral cortex.
Components of the anterolateral system:
| Tract | Target | Function |
|---|---|---|
| Spinothalamic | VPL thalamus | Conscious pain & temperature |
| Spinoreticular | Reticular formation (brainstem) | Emotional/arousal aspects of pain |
| Spinomesencephalic | Periaqueductal gray, superior colliculi | Central modulation of pain |
B. Posterior Column - Medial Lemniscal Pathway (PCML)
Sensation carried: Fine/discriminative touch, vibration, conscious proprioception, two-point discrimination
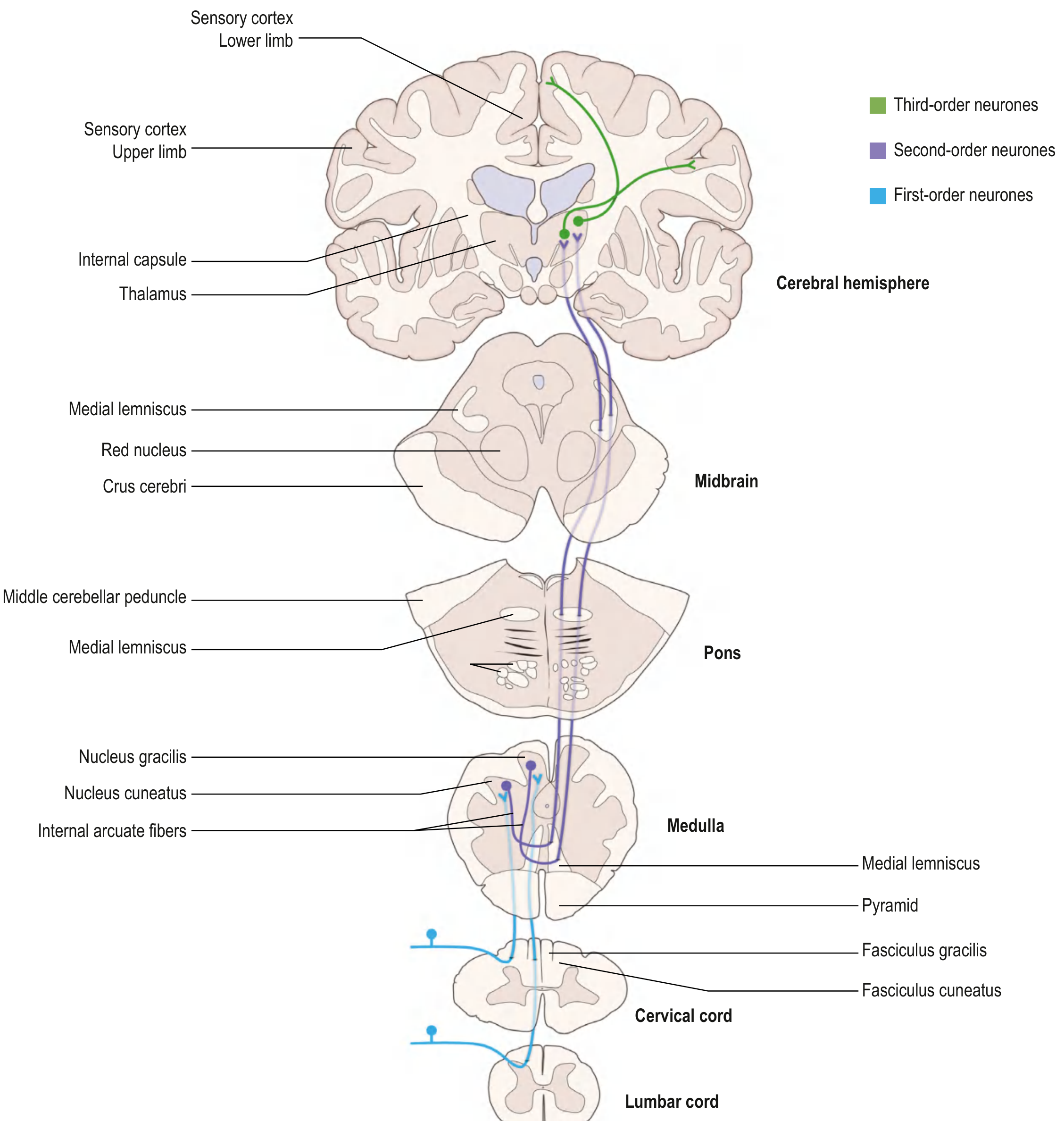
Pathway:
- 1st order neuron: Cell body in DRG → enters spinal cord → axon ascends IPSILATERALLY in the posterior funiculus (dorsal columns)
- Fibers from lower limb/trunk: Fasciculus gracilis (medial; T7 and below)
- Fibers from upper limb/neck: Fasciculus cuneatus (lateral; C2-T6)
- Synapses at nucleus gracilis / nucleus cuneatus in the caudal medulla
- 2nd order neuron: Axons cross as internal arcuate fibers → form the medial lemniscus → ascend to VPL nucleus of thalamus
- 3rd order neuron: VPL → through posterior limb of internal capsule → primary somatosensory cortex
Key point: Crosses at the medulla (not spinal cord) → contralateral cortex.
Comparison: Spinothalamic vs Posterior Column
| Feature | Spinothalamic (Anterolateral) | Posterior Column (PCML) |
|---|---|---|
| Sensation | Pain, temperature, crude touch | Fine touch, vibration, proprioception |
| Where it crosses | Spinal cord (anterior commissure) | Medulla (internal arcuate fibers) |
| Location in spinal cord | Anterolateral white matter | Posterior funiculus |
| 1st neuron synapse | Posterior horn (ipsilateral) | Dorsal column nuclei (medulla) |
| 2nd neuron synapse | VPL thalamus | VPL thalamus |
| End in cortex | Contralateral postcentral gyrus | Contralateral postcentral gyrus |
| Clinical test | Pin-prick, cold/warm | Tuning fork, joint position sense |
9. DESCENDING TRACTS (Motor Pathways)
Descending tracts control voluntary movement, posture, and balance. They consist of:
- Upper Motor Neuron (UMN): Cell body in cortex or brainstem
- Lower Motor Neuron (LMN): Cell body in anterior horn of spinal cord
A. Lateral Motor System
1. Lateral Corticospinal Tract (Most important)
Controls: Voluntary movements of upper and lower limbs
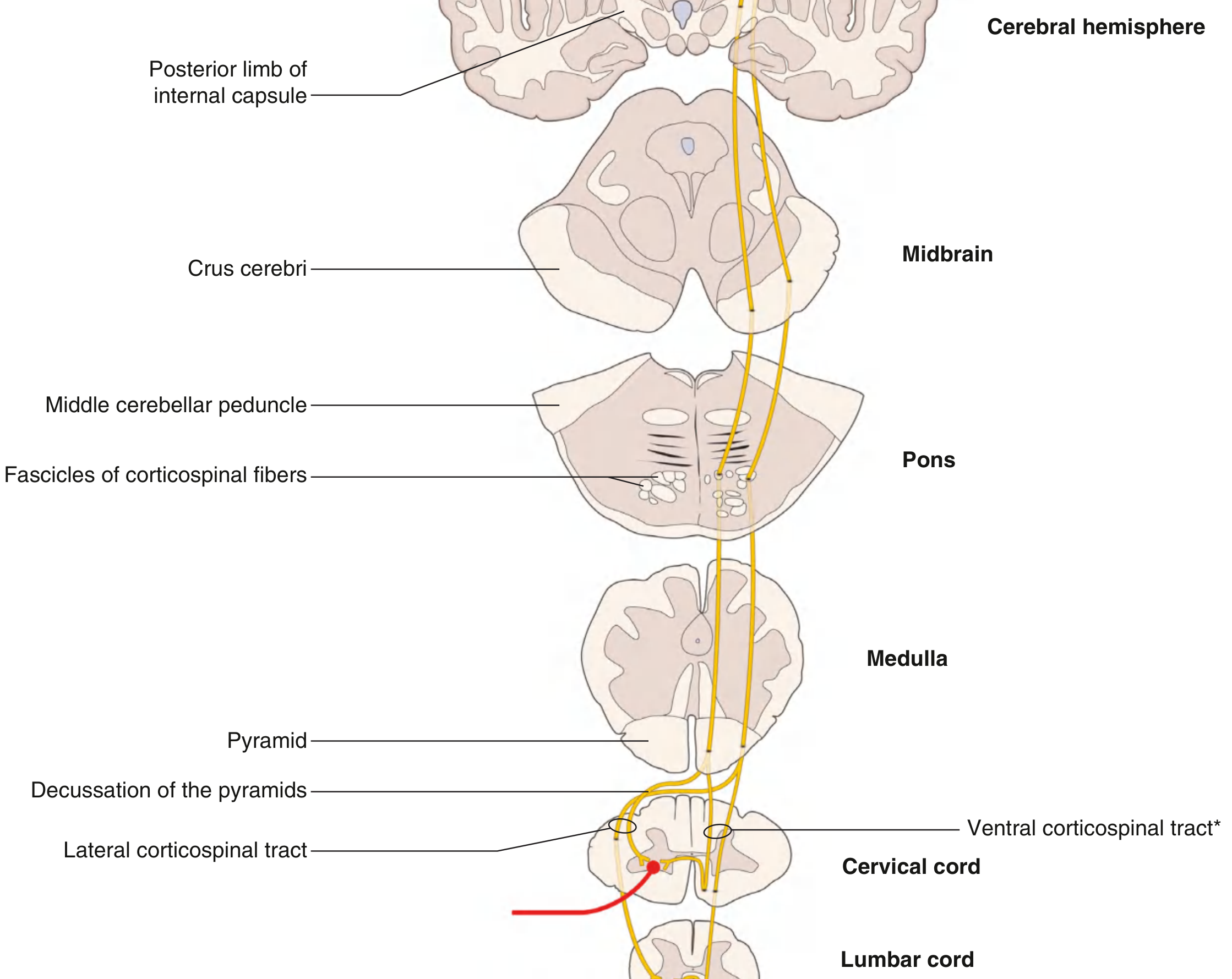
Pathway:
- UMN: Cell body in primary motor cortex (precentral gyrus)
- Axons converge in corona radiata → descend through posterior limb of internal capsule
- Continue through crus cerebri (midbrain) → descend as small fascicles through pons (separated by transverse pontocerebellar fibers)
- Fibers regroup in the medulla → form the pyramid (hence also called the pyramidal tract)
- At the caudal medulla: ~85% of fibers decussate at the pyramidal decussation (decussation of pyramids)
- Cross to contralateral side → descend as lateral corticospinal tract in the lateral funiculus
- Synapse on LMN cell bodies in the lateral anterior horn
- LMN axons exit through the anterior root → reach target muscles
Key point: Crosses in the medulla → therefore a lesion above the decussation causes contralateral limb weakness; a lesion below causes ipsilateral weakness.
2. Rubrospinal Tract
Controls: Flexor muscle activity and inhibits extensors (mainly upper limb)
Pathway:
- UMN: Red nucleus (midbrain tegmentum)
- Axons cross immediately as the ventral tegmental decussation
- Descend as rubrospinal tract in the lateral column
- Descend only to cervical spinal cord levels
- Synapse on interneurons → influence flexor muscles of the upper limb
B. Medial Motor System
Regulates axial (trunk) muscles for posture, balance, and gait. All four tracts project bilaterally.
| Tract | Origin | Function |
|---|---|---|
| Anterior corticospinal tract | Primary motor cortex (fibers that did NOT decussate at medulla) | Controls trunk/axial muscles bilaterally; descends to upper thoracic level |
| Tectospinal tract | Superior colliculus (dorsal midbrain) | Reflex postural movements in response to visual stimuli; decussates as dorsal tegmental decussation; cervical cord only |
| Vestibulospinal tract | Vestibular nuclei (pons and medulla) | Lateral: ipsilateral, full cord length → excites extensors; Medial: bilateral, cervical/thoracic → postural adjustments to head movement |
| Reticulospinal tract | Reticular formation (pons and medulla) | Pontine (medial): excites extensors; Medullary (lateral): inhibits extensors; overall control of posture and muscle tone |
10. UMN vs LMN Lesion (Clinical Application)
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Site | Above anterior horn (brain/spinal cord) | Anterior horn, ventral root, peripheral nerve |
| Tone | Spasticity (increased) | Flaccidity (decreased) |
| Reflexes | Hyperreflexia | Hyporeflexia/areflexia |
| Plantarresponse | Extensor (Babinski +ve) | Flexor (normal) |
| Wasting | Minimal (disuse atrophy) | Severe (denervation atrophy) |
| Fasciculations | Absent | Present |
11. Reflex Arc
A reflex is an involuntary, stereotyped response to a stimulus. The basic reflex arc has 5 components:
- Receptor - detects stimulus
- Afferent (sensory) neuron - carries signal to spinal cord
- Integration center - spinal cord (interneurons)
- Efferent (motor) neuron - carries response signal
- Effector - muscle or gland
Monosynaptic Reflex (Stretch/Myotatic Reflex)
- Example: Knee jerk (patellar reflex - L3/L4)
- Tapping the tendon stretches the muscle → activates muscle spindles (Ia afferents) → directly synapse on alpha motor neurons → muscle contracts
- Only ONE synapse involved (monosynaptic)
Polysynaptic Reflex
- Example: Withdrawal (flexor) reflex
- Involves interneurons → can cross midline (crossed extensor reflex)
12. Quick Summary Table - Spinal Cord Tracts
| Tract | Type | Column | Sensation/Function | Crosses |
|---|---|---|---|---|
| Fasciculus gracilis | Ascending | Posterior | Fine touch/vibration/proprioception (T7-sacral) | Medulla |
| Fasciculus cuneatus | Ascending | Posterior | Fine touch/vibration/proprioception (C2-T6) | Medulla |
| Spinothalamic | Ascending | Anterolateral | Pain, temperature, crude touch | Spinal cord |
| Spinoreticular | Ascending | Anterolateral | Emotional/arousal aspects of pain | Spinal cord |
| Lateral corticospinal | Descending | Lateral | Voluntary limb movement | Medulla |
| Anterior corticospinal | Descending | Anterior | Axial muscle/postural control | Spinal cord (at level) |
| Rubrospinal | Descending | Lateral | Upper limb flexion | Midbrain |
| Vestibulospinal | Descending | Anterior | Postural balance | Varies |
| Reticulospinal | Descending | Anterior/lateral | Muscle tone, posture | Varies |
| Tectospinal | Descending | Anterior | Visual reflex postural movements | Midbrain |
Source: Gray's Anatomy for Students, Chapter 9 (Neuroanatomy); Principles of Neural Science, Kandel 6th ed.
Exam Tips for 1st Year MBBS
- The spinothalamic tract crosses in the spinal cord (2-3 segments above entry); the PCML crosses in the medulla - this explains different deficits in hemisection (Brown-Sequard syndrome)
- Lateral corticospinal tract carries ~85% of corticospinal fibers; it decussates at the pyramidal decussation in caudal medulla
- UMN = spastic paralysis; LMN = flaccid paralysis - remember BUSHY (Babinski, UMN features: hyperreflexia, spasticity; LMN: hyporeflexia, atrophy, fasciculations)
- All three conscious somatosensory and motor tracts end at the VPL thalamus (sensory) or VPL/VL thalamus (motor relay) before reaching the cortex
- The posterior column carries information ipsilaterally all the way to the medulla before crossing
Make a comparison table of all neuro syndromes (Brown-Séquard, Weber, etc.)
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have all the data needed from Bradley & Daroff's Neurology, Localization in Clinical Neurology, Guyton & Hall, and other sources. Here is the complete comparison table:
Neurological Syndromes - Complete Comparison Table
PART 1: Spinal Cord Syndromes
| Syndrome | Level | Lesion Site | Motor (UMN) | Sensation Lost | Sensation Preserved | Cause | Prognosis |
|---|---|---|---|---|---|---|---|
| Complete Transection | Any spinal level | Entire cord cross-section | Bilateral spastic paralysis below | ALL modalities bilaterally below | None below level | Trauma, tumor | Poor |
| Brown-Séquard (Hemisection) | Any spinal level | Lateral half of cord | Ipsilateral spastic paralysis below (corticospinal) | Ipsilateral: fine touch, vibration, proprioception (dorsal column) | Contralateral crude touch (partial) | Stab wound, MS, tumor, disc | Best prognosis of incomplete SCI |
| Contralateral: pain & temperature (spinothalamic; 2-3 segments below) | |||||||
| Central Cord Syndrome | Cervical | Central gray + medial white matter | UE > LE weakness (sacral sparing) | Variable, sacral often preserved | Sacral sensation often spared | Cervical hyperextension + spondylosis | Most common incomplete SCI; moderate recovery |
| Anterior Cord Syndrome | Any | Anterior 2/3 of cord (anterior spinal artery territory) | Bilateral motor paralysis (corticospinal) | Bilateral pain & temperature loss (spinothalamic) | Preserved: vibration, proprioception, fine touch (posterior columns intact) | Anterior spinal artery occlusion, flexion injury | Worst prognosis of incomplete SCI |
| Posterior Cord Syndrome | Any | Posterior columns only | Motor intact | Vibration, proprioception, fine touch lost bilaterally | Pain & temperature intact | B12 deficiency (subacute combined degeneration), syphilis (tabes dorsalis), MS | Rare; motor preserved |
| Conus Medullaris Syndrome | L1-L2 (conus) | Conus medullaris | LMN weakness of legs + sphincters | Saddle anesthesia (S3-S5) | Variable | Central disc herniation, tumor | Variable; bowel/bladder often permanent |
| Cauda Equina Syndrome | Below L2 (not spinal cord) | Cauda equina nerve roots | LMN flaccid weakness, areflexia | Saddle anesthesia, radicular pain | Variable | Massive disc herniation, tumor | Surgical emergency; good if treated early |
| Syringomyelia | Cervical typically | Central canal expansion - damages anterior white commissure first | LMN at level (anterior horn) + UMN below | Cape distribution: pain & temperature loss (bilateral; spinothalamic fibers cross here) | Preserved: fine touch, proprioception (posterior columns) | Chiari malformation, trauma, tumor | Progressive; surgery stabilizes |
Key: Brown-Séquard Deficits at a Glance
| Finding | Side | Why |
|---|---|---|
| Spastic paralysis | Ipsilateral | Lateral corticospinal tract (already crossed in medulla) |
| Loss of fine touch, vibration, proprioception | Ipsilateral | Posterior columns (cross in medulla - not yet crossed at cord level) |
| Loss of pain & temperature | Contralateral (2-3 segments below) | Spinothalamic tract (crosses in spinal cord near entry) |
| LMN signs | Ipsilateral at level | Anterior horn cells at lesion level |
Source: Guyton & Hall Medical Physiology; Bradley and Daroff's Neurology in Clinical Practice
PART 2: Brainstem Syndromes (Crossed Paralysis Syndromes)
Hallmark: Ipsilateral CN palsy + contralateral hemiparesis = lesion is in the brainstem
MIDBRAIN Syndromes
| Syndrome | Level | Lesion Site | Ipsilateral Signs | Contralateral Signs | Cause |
|---|---|---|---|---|---|
| Weber | Midbrain (ventral) | Cerebral peduncle + CN III fascicle | CN III palsy: ptosis, mydriasis, eye "down and out" | Hemiplegia (incl. lower face) - corticospinal/corticobulbar involvement | PCA infarct (penetrating branches) |
| Benedikt | Midbrain (tegmentum) | CN III fascicle + red nucleus + brachium conjunctivum | CN III palsy (dilated pupil) | Hemiataxia, intention tremor (red nucleus); hemiparesis with hyperreflexia | PCA infarct, hemorrhage, tumor |
| Claude | Midbrain (dorsal tegmentum) | CN III fascicle + dorsal red nucleus + superior cerebellar peduncle | CN III palsy | Prominent cerebellar signs: ataxia, asynergia, dysmetria, dysdiadochokinesis (no hemiballismus) | PCA infarct |
| Nothnagel | Midbrain (dorsal) | CN III fascicle + superior cerebellar peduncle | CN III palsy + ipsilateral ataxia | - | Tumor, infarct |
| Parinaud (Dorsal Midbrain / Sylvian Aqueduct) | Dorsal midbrain | Pretectal area + superior colliculus | - | - | Mainly neuro-ophthalmologic: upgaze palsy, convergence-retraction nystagmus, light-near dissociation, lid retraction (Collier's sign) |
PONTINE Syndromes
| Syndrome | Level | Lesion Site | Ipsilateral Signs | Contralateral Signs | Cause |
|---|---|---|---|---|---|
| Millard-Gubler | Pons (ventral) | CN VI + CN VII fascicles + pyramidal tract | CN VI palsy (lateral gaze), CN VII palsy (LMN - all face) | Hemiparesis (corticospinal) | Basilar artery branch infarct, tumor |
| Foville | Pons | CN VI + CN VII + pyramidal tract + PPRF | CN VI, CN VII palsy + ipsilateral horizontal gaze palsy, Horner syndrome, deafness, taste/sensation loss | Contralateral hemiparesis + ataxia | Infarct |
| Raymond | Pons (caudal ventral) | CN VI + pyramidal tract | CN VI palsy only | Contralateral hemiparesis | Basilar artery occlusion |
| Locked-in Syndrome | Pons (bilateral ventral) | Bilateral pyramidal + corticobulbar tracts | Quadriplegia, anarthria, dysphagia | (Bilateral) | Basilar artery thrombosis, pontine hemorrhage |
MEDULLARY Syndromes
| Syndrome | Level | Lesion Site | Ipsilateral Signs | Contralateral Signs | Cause |
|---|---|---|---|---|---|
| Wallenberg (Lateral Medullary) | Lateral medulla | PICA territory: spinal trigeminal nucleus/tract, nucleus ambiguus, vestibular nuclei, inferior cerebellar peduncle, sympathetic fibers, spinothalamic tract | Facial numbness (pain & temp); hoarseness, dysphagia (CN IX/X via nucleus ambiguus); vertigo, nystagmus; limb ataxia; Horner syndrome (ptosis, miosis, anhidrosis) | Loss of pain & temperature (body - spinothalamic) | PICA or vertebral artery thrombosis |
| Medial Medullary (Déjerine) | Medial medulla | Pyramid + medial lemniscus + CN XII fascicle | CN XII palsy (tongue deviates ipsilaterally) | Hemiparesis (pyramidal); loss of vibration, fine touch, proprioception (medial lemniscus) | Anterior spinal artery or vertebral artery occlusion |
| Opalski | Lateral medulla (caudal to pyramidal decussation) | Wallenberg territory + corticospinal fibers below decussation | All of Wallenberg + ipsilateral hemiparesis (unique!) | Pain & temperature loss (body) | Vertebral artery occlusion |
| Jackson | Medullary tegmentum | CN X + CN XII + corticospinal | CN X (palate, pharynx), CN XII (tongue) palsy | Contralateral hemiparesis | Infarct, tumor |
PART 3: Other Named CN and Cranial Base Syndromes
| Syndrome | Location | Key Signs | Cause |
|---|---|---|---|
| Gradenigo | Petrous apex (temporal bone) | Facial/mastoid pain (CN V1), ipsilateral CN VI palsy, +/- CN VII involvement | Petrous apicitis (otitis media complication) |
| Tolosa-Hunt | Cavernous sinus / superior orbital fissure | CN III, IV, VI palsies + CN V1/V2 sensory loss + Horner (sympathetics in sinus) + painful ophthalmoplegia | Inflammatory granuloma; responds to steroids |
| Horner Syndrome | Sympathetic chain (hypothalamus → ciliospinal center C8-T2 → superior cervical ganglion) | Ptosis (partial), miosis, anhidrosis (3 Ps) | Pancoast tumor, carotid dissection, Wallenberg, syringomyelia |
PART 4: Cerebrovascular / Hemispheric Syndromes
| Syndrome | Artery | Area Infarcted | Key Deficits |
|---|---|---|---|
| MCA (dominant) | Middle cerebral artery | Lateral frontal, parietal, temporal cortex | Contralateral hemiplegia (face & arm > leg), hemianesthesia, Broca/Wernicke aphasia, hemianopia |
| MCA (non-dominant) | MCA | Same area right hemisphere | Contralateral neglect, anosognosia, constructional apraxia |
| ACA | Anterior cerebral artery | Medial frontal and parietal lobes | Contralateral leg > arm weakness, urinary incontinence, abulia |
| PCA | Posterior cerebral artery | Occipital lobe, thalamus, midbrain | Contralateral homonymous hemianopia, thalamic pain syndrome, midbrain syndromes (Weber, etc.) |
| PICA | Posterior inferior cerebellar | Lateral medulla + inferior cerebellum | Wallenberg syndrome |
| AICA | Anterior inferior cerebellar | Lateral pons + anterior cerebellum | Ipsilateral facial numbness, deafness (CN VIII), Horner; contralateral body pain/temp loss |
| Basilar artery | Basilar | Entire brainstem + pons | "Top of basilar": visual loss, behavioral changes, CN palsies; complete occlusion → locked-in |
PART 5: Memory Mnemonics
Brown-Séquard: "Same-Same-Opposite"
- Same side: motor loss + posterior column loss
- Opposite side: pain/temperature loss
Brainstem syndromes: "WEB-MG" (Weber, Everything Brainstem, Millard-Gubler)
- All have: ipsilateral CN + contralateral body
Wallenberg: "DYVADS Horner"
- Dysphagia, Yaw nystagmus (vertigo), Ataxia, Dissociated sensory loss (face ipsi / body contra), Sympathetic (Horner)
Anterior vs Posterior cord: "Anterior = No motor/pain; Posterior = No position"
Sources: Bradley and Daroff's Neurology in Clinical Practice; Localization in Clinical Neurology 8e; Guyton & Hall Medical Physiology; Adams and Victor's Principles of Neurology 12e
This is a shared conversation. Sign in to Orris to start your own chat.