Explain in retinol to me as I'm 3rd year pg resident of general medicine appearing for muhs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
Reading File
Excellent. I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Retinol (Vitamin A) - A Complete PG Medicine Review
Sources: Robbins & Kumar Basic Pathology, Harrison's 22e, Lippincott Biochemistry 8e, Park's PSM, Wills Eye Manual
1. Chemistry and Forms
Vitamin A is a fat-soluble vitamin encompassing a group of related compounds:
| Form | Role |
|---|---|
| Retinol | Transport form; storage form (as retinyl ester) |
| Retinal (retinaldehyde) | Visual cycle (11-cis retinal in rhodopsin) |
| Retinoic acid | Gene transcription regulator |
| β-Carotene | Plant-derived provitamin A (converted in intestinal wall) |
"Retinoids" = all natural + synthetic chemicals structurally related to vitamin A.
Units: 1 RAE (Retinol Activity Equivalent) = 1 µg retinol = 12 µg β-carotene = 24 µg other provitamin A carotenoids. Old literature uses IU: 1 µg retinol = 3.33 IU.
2. Dietary Sources
Animal (preformed retinyl esters - best absorbed):
- Halibut/Cod liver oil (highest: 900,000 / 18,000 RE per 100 g)
- Ox liver (16,500 RE/100 g)
- Butter, margarine, eggs, milk, fish
Plant (provitamin A carotenoids):
- Carrot (1,167 RE), Spinach (607 RE), Mango (313 RE), Papaya (118 RE)
Carotenoids contribute ~30% of dietary vitamin A. Conversion is impaired in malnourished children and those with diarrhoea.
3. Absorption, Transport & Storage
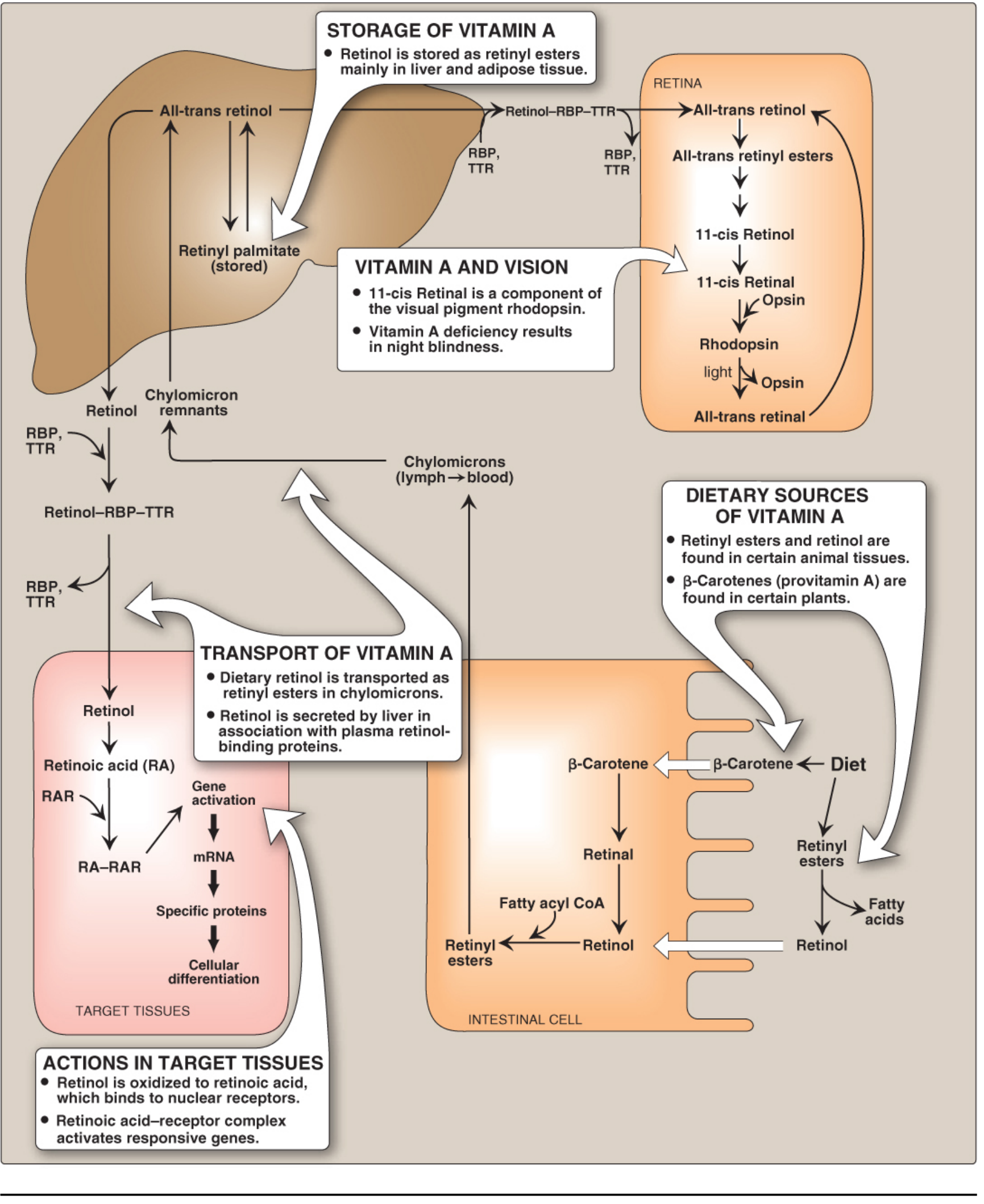
Lippincott Biochemistry, Fig. 28.19 - Absorption, transport and storage of Vitamin A
Step-by-step:
-
Intestine: Dietary retinyl esters + β-carotene absorbed (requires bile, pancreatic enzymes, antioxidant). β-carotene converted to retinol by intestinal enzymes. Retinol esterified (mainly by LRAT - lecithin retinol acyltransferase) → retinyl esters packaged into chylomicrons → lymph → blood.
-
Liver (main store): Retinol taken up via apolipoprotein E receptor. Stored predominantly as retinyl palmitate in perisinusoidal stellate (Ito) cells. >90% of body's reserves in liver. Normal reserves last 6-9 months.
-
Transport to periphery: Retinol released from liver bound to Retinol-Binding Protein (RBP) (synthesized in liver). RBP complexes with transthyretin - this trimolecular complex:
- Prevents filtration by renal glomerulus (protects against free retinol toxicity)
- Allows uptake via specific RBP cell-surface receptors
-
Peripheral uptake: Retinol released intracellularly → binds cellular retinol-binding proteins (CRBPs) → can be stored as retinyl ester OR oxidized to retinoic acid.
Exam point: In severe protein deficiency, decreased RBP production prevents mobilization of liver retinol stores - hence VAD can occur despite adequate liver stores!
4. Mechanism of Action (Molecular)
Retinoic acid acts like a steroid hormone:
- Retinol → oxidized → Retinoic acid
- Two receptor families: RARs (bind all-trans retinoic acid + 9-cis RA) and RXRs (bind only 9-cis RA)
- RAR/RXR form heterodimers → bind Retinoic Acid Response Elements (RAREs) on DNA
- Regulate transcription: stimulate or repress gene expression
- RXRs also heterodimerize with PPARs, Vitamin D receptors, thyroid hormone receptors - hence broad metabolic effects
5. Functions - HIGH-YIELD
A. Vision (Retinal form)
- Rhodopsin (rod cells) = 11-cis retinal + opsin - responsible for dim/dark light vision
- On light exposure: 11-cis retinal → all-trans retinal + opsin (bleaching) → triggers G-protein (transducin) → nerve impulse
- Regeneration: all-trans retinal → all-trans retinol → 11-cis retinol → 11-cis retinal → re-combines with opsin
- Three iodopsins (cone cells) similarly use retinal for color vision
B. Epithelial Cell Differentiation
- Vitamin A maintains mucus-secreting columnar epithelium
- Deficiency → squamous metaplasia (keratinizing epithelium replaces columnar/cuboidal)
- Affects: conjunctiva, cornea, respiratory tract, GI mucosa, urinary tract, skin
C. Immune Function
- Supports barrier defenses (epithelial integrity)
- Required for normal innate and acquired immunity
- Deficiency → increased susceptibility to respiratory, GI, measles infections
D. Growth & Reproduction
- Essential for normal spermatogenesis
- Supports fetal development
E. Metabolic Effects (Retinoic acid)
- Inhibits adipogenesis, stimulates lipid breakdown
- RXR as cofactor of PPARs → linked to insulin sensitivity and thiazolidinedione drug action
6. Deficiency - Vitamin A Deficiency (VAD)
WHO Classification of Xerophthalmia
| Grade | Stage |
|---|---|
| XN | Night blindness (nyctalopia) - earliest symptom |
| X1A | Conjunctival xerosis |
| X1B | Bitot's spots |
| X2 | Corneal xerosis |
| X3A | Corneal ulceration / keratomalacia < 1/3 cornea |
| X3B | Corneal ulceration / keratomalacia ≥ 1/3 cornea |
| XS | Corneal scar |
| XF | Xerophthalmia fundus |
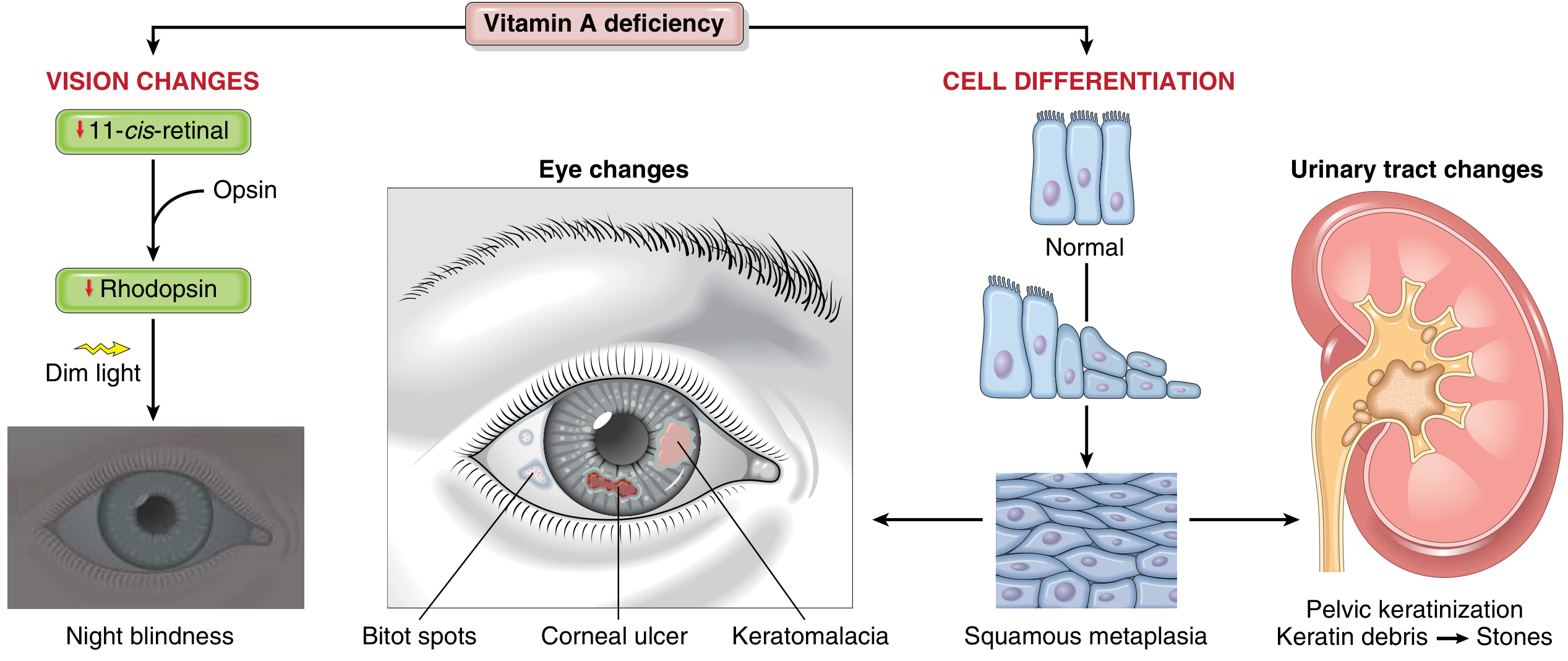
Robbins Basic Pathology - Vitamin A deficiency: Vision changes, squamous metaplasia, and urinary tract changes
Clinical Features in Detail
Ocular (Xerophthalmia):
- Night blindness (XN): Earliest, most common. Mother notices child can't see in dim light
- Conjunctival xerosis (X1A): Conjunctiva dry, non-wettable, muddy, wrinkled - "emerging like sand banks at receding tide" when child ceases to cry
- Bitot's spots (X1B): Triangular, pearly-white/yellowish, foamy, keratinized conjunctival plaques on bulbar conjunctiva - bilateral, temporal > nasal. (In older adults, may be inactive sequelae)
- Corneal xerosis (X2): Cornea dull, dry, non-wettable, eventually opaque
- Keratomalacia (X3B): MEDICAL EMERGENCY - softening/liquefaction of cornea. Cornea may perforate and collapse → irreversible blindness. Fatality rate 4-25%
Extra-ocular:
- Skin: Follicular hyperkeratosis (phrynoderma - "toad skin") - follicular plugging with keratin on extensor surfaces
- Growth retardation, anorexia
- Increased infections (measles, diarrhea, respiratory - leading causes of death in VAD)
- Squamous metaplasia of urinary tract mucosa → pelvic keratinization → keratin debris → renal calculi
Assessment
- Serum retinol: Normal = 1.05-3.50 µmol/L (30-100 µg/dL). Deficient = <0.70 µmol/L (<20 µg/dL or <10 µg/dL in children per Park's)
- Note: Serum retinol is an acute-phase reactant (false low in inflammation) - always measure CRP simultaneously
WHO Community Prevalence Criteria (evidence of public health problem)
| Criterion | Threshold |
|---|---|
| Nightblindness | >1% |
| Bitot's spots | >0.5% |
| Corneal xerosis/ulceration/keratomalacia | >0.01% |
| Corneal scar | >0.05% |
| Serum retinol <10 µg/dL | >5% |
7. Treatment
Urgent treatment (WHO/Indian protocol):
- Day 1: 200,000 IU (110 mg retinol palmitate) orally
- Day 2: 200,000 IU orally
- At discharge (after 2 weeks): 200,000 IU orally
Keratomalacia = treated as emergency (risk of death, especially in infants)
Prevention (National programme):
- Children 1-6 years: 200,000 IU orally every 6 months
- Children 6-12 months: 100,000 IU
- Neonates: WHO does NOT recommend routine high-dose supplementation
8. Toxicity (Hypervitaminosis A)
More common with preformed retinol (supplements, liver, fish liver oil), not carotenoids
Acute toxicity (single massive dose):
- Nausea, vomiting, abdominal pain, severe headache, dizziness, drowsiness
- Raised ICP → pseudotumor cerebri (papilloedema, diplopia) - does NOT fully resolve after stopping
Chronic toxicity:
- Skin: desquamation, dryness, hair loss
- Hepatomegaly → liver fibrosis/cirrhosis (irreversible, unlike other symptoms)
- Bone: periosteal hyperostosis, bone/joint pain, hypercalcemia
- Alopecia, cheilitis
- Elderly more susceptible (delayed lipoprotein clearance → longer retinyl ester exposure)
Teratogenicity: High-dose vitamin A is a well-established teratogen → neural crest defects, craniofacial abnormalities, cardiac malformations. Isotretinoin (13-cis retinoic acid) is contraindicated in pregnancy. Carotenoid excess (carotenodermia) causes yellow/orange skin discolouration but is NOT toxic.
Exam point: Pseudotumor cerebri and liver cirrhosis are the two complications that persist after stopping excess vitamin A. All others resolve.
9. Quick Recall Summary Table
| Parameter | Value |
|---|---|
| Type | Fat-soluble vitamin |
| Active form (vision) | 11-cis retinal |
| Transport protein | RBP + Transthyretin |
| Storage site | Liver stellate (Ito) cells |
| Storage form | Retinyl palmitate |
| Duration of liver stores | 6-9 months |
| Deficiency: earliest sign | Night blindness (XN) |
| Deficiency: emergency | Keratomalacia (X3B) |
| Serum normal level | 30-100 µg/dL (1.05-3.50 µmol/L) |
| Treatment dose (acute VAD) | 200,000 IU × 2 days |
| Toxicity: irreversible features | Pseudotumor cerebri, liver cirrhosis |
| Teratogen? | YES (preformed vitamin A / retinoids) |
Sources: Robbins & Kumar Basic Pathology 10e, p.292-294 | Harrison's Principles 22e, p.2654 | Lippincott Biochemistry 8e, p.1077-1078 | Park's PSM, p.711-713 | Wills Eye Manual p.1044-1045
Explain incretin to me as a pg resident of 3rd year appearing muhs exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile a thorough, exam-focused answer.
Incretins - Complete PG Medicine Review for MUHS
Sources: Katzung's Pharmacology 16e, Lippincott Pharmacology, Goldman-Cecil Medicine, Harrison's 22e, Guyton & Hall Physiology, Textbook of Family Medicine
1. What is the Incretin Effect?
When an equal amount of glucose is given orally vs. intravenously, the oral route produces a significantly higher insulin response (up to 60-70% greater). This amplification is called the "incretin effect."
This happens because glucose in the gut triggers release of intestinal hormones - the incretins - that amplify glucose-stimulated insulin secretion from pancreatic β-cells.
Exam point: The incretin effect is markedly blunted/reduced in Type 2 Diabetes Mellitus (T2DM). This is one of the core pathophysiological defects in T2DM.
2. The Two Major Incretin Hormones
| Feature | GLP-1 (Glucagon-Like Peptide-1) | GIP (Glucose-Dependent Insulinotropic Polypeptide) |
|---|---|---|
| Secreted by | L cells of distal ileum + colon | K cells of proximal duodenum/jejunum |
| Stimulus | Oral glucose, fats, proteins | Glucose + fat (fat is a stronger stimulus for GIP) |
| Fasting level | 5-10 pmol/L | Low |
| Post-meal level | 15-50 pmol/L (rises within minutes) | Rises rapidly |
| Degraded by | DPP-4 enzyme + renal clearance (t½ ~2 min) | DPP-4 enzyme |
| In T2DM | Secretion impaired + response intact | Secretion near-normal but β-cell response impaired |
Both hormones rise within minutes of eating, even before digested food reaches the L cells - via a combination of endocrine and neural signals (vagal reflexes, etc.)
3. Actions of Incretins
GLP-1 Actions (HIGH-YIELD - multiple effects)
| System | Effect |
|---|---|
| Pancreas (β-cell) | ↑ Glucose-dependent insulin secretion (only when glucose elevated - key safety feature) |
| Pancreas (α-cell) | ↓ Glucagon secretion |
| Stomach | ↓ Gastric emptying (slows glucose absorption) |
| Brain/CNS | ↓ Appetite / food intake (satiety effect) |
| β-cell trophic | ↓ β-cell apoptosis; promotes β-cell proliferation |
| Heart/vessels | Cardioprotective (studied in CVD trials) |
GIP Actions
- ↑ Glucose-dependent insulin secretion
- ↑ Triglyceride storage in adipose tissue
- Less potent compared to GLP-1 in T2DM (β-cell response is blunted)
Exam point: GLP-1's insulin stimulation is glucose-dependent - insulin release is pronounced when glucose is high but attenuated when glucose is normal. This is why GLP-1-based drugs have a LOW risk of hypoglycemia compared to sulfonylureas.
4. Degradation - The DPP-4 Problem
GLP-1 and GIP are rapidly inactivated by the enzyme Dipeptidyl Peptidase-4 (DPP-4) and cleared by the kidney. Their half-life is only ~2 minutes in circulation. This makes native GLP-1 therapeutically useless - it cannot be administered as a drug directly.
This led to two drug strategies:
Meal → GLP-1/GIP released from gut
↓
DPP-4 degrades them rapidly (t½ ~2 min)
↓
TWO drug approaches to exploit this:
1. GLP-1 Receptor Agonists → DPP-4 resistant analogues (mimic the incretin effect)
2. DPP-4 Inhibitors ("Gliptins") → block degradation, ↑ endogenous GLP-1/GIP
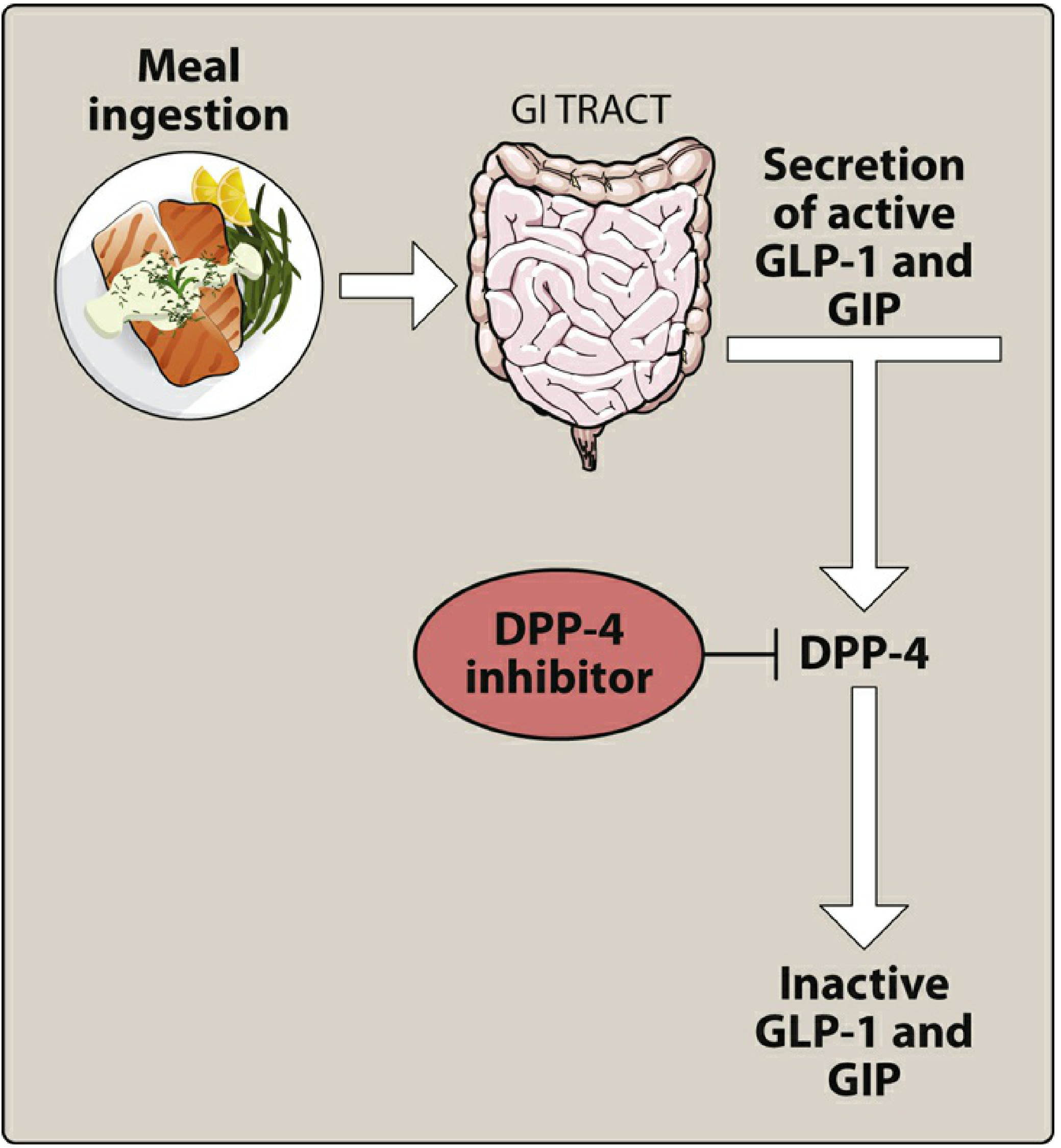
Lippincott Pharmacology Fig. 24.13 - Mechanism of action of DPP-4 inhibitors
5. Drug Classes Based on Incretin Mechanism
CLASS 1: GLP-1 Receptor Agonists ("Incretin Mimetics")
Mechanism: Exogenous GLP-1 analogues that are resistant to DPP-4 degradation. Bind and activate GLP-1 receptors. All actions of GLP-1 above.
Route: Subcutaneous injection (polypeptides - cannot be given orally, except semaglutide oral formulation)
Comparison Table - GLP-1 RAs
| Drug | Frequency | Half-life | Special Notes |
|---|---|---|---|
| Exenatide | BD SC | ~2-3 h | Derived from Gila monster venom (exendin-4), 53% homology with GLP-1. Avoid in severe renal impairment |
| Exenatide XR | Once weekly SC | - | Extended release microspheres |
| Liraglutide | Once daily SC | ~13 h | Cardioprotective (LEADER trial) |
| Dulaglutide | Once weekly SC | ~5 days | Cardioprotective |
| Lixisenatide | Once daily SC | Short-acting | |
| Semaglutide | Once weekly SC OR once daily oral | ~7 days | Most potent; approved for obesity (2.4 mg/week); SELECT trial: 20% ↓ in MACE in non-diabetics with obesity |
| Tirzepatide | Once weekly SC | ~117 h | Dual GLP-1/GIP agonist (first of class). FDA approved T2DM 2022, obesity 2023. Greater weight loss than semaglutide alone |
Effects on HbA1c: Reduce by ~0.5-1.5%
Cardiovascular benefits (key for MUHS exams):
- Liraglutide, dulaglutide, semaglutide: approved to reduce cardiovascular mortality in T2DM with CVD
- SELECT trial (semaglutide 2.4mg): 20% ↓ MACE in overweight/obese patients WITHOUT diabetes with CVD
- STEP-HFpEF: semaglutide improved HFpEF symptoms and reduced inflammation
Adverse Effects:
- GI (most common): Nausea, vomiting, diarrhea, constipation (especially on initiation)
- Pancreatitis (avoid in chronic pancreatitis history)
- Thyroid C-cell tumors in rodents → contraindicated in medullary thyroid carcinoma and MEN type 2
- Weight loss (beneficial side effect)
Do NOT combine GLP-1 RAs with DPP-4 inhibitors (overlapping mechanism + increased toxicity)
CLASS 2: DPP-4 Inhibitors ("Gliptins") - "Incretin Enhancers"
Mechanism: Inhibit DPP-4 enzyme → prevent breakdown of endogenous GLP-1 and GIP → prolonged incretin effect → ↑ insulin secretion (meal-dependent) + ↓ glucagon
Route: Oral (tablets)
Comparison Table - DPP-4 Inhibitors
| Drug | Key Feature |
|---|---|
| Sitagliptin | First approved; renal excretion; dose adjust in renal impairment |
| Saxagliptin | CYP3A4/5 metabolism; ↑ risk of heart failure hospitalizations (avoid in heart failure) |
| Alogliptin | Renal excretion; dose adjust |
| Linagliptin | Hepatobiliary elimination - no dose adjustment in renal impairment (only gliptin safe in severe CKD without dose adjustment) |
| Vildagliptin | Available in India/Europe |
HbA1c reduction: 0.5-0.8%
Advantages over GLP-1 RAs:
- Oral drug
- Weight neutral (do not cause weight loss, unlike GLP-1 RAs)
- Well tolerated, minimal GI side effects
Adverse Effects:
- Nasopharyngitis, headache (most common)
- Pancreatitis (rare but serious)
- Severe joint pain (arthralgia - arthritis, can be disabling)
- Hypersensitivity reactions
- Saxagliptin: ↑ heart failure hospitalizations
Exam memory trick - "Gliptins": All DPP-4 inhibitors end in "-gliptin". The one safe in renal failure without dose adjustment = Linagliptin (hepatic route).
6. Incretin Defect in T2DM - Pathophysiology
In T2DM, there are TWO defects:
- GLP-1 secretion is impaired after oral carbohydrate (blunted release from L cells)
- GIP response is relatively preserved BUT β-cells become resistant to GIP stimulation
This means the normal 60-70% incretin contribution to postprandial insulin is lost - contributing to postprandial hyperglycemia.
7. Incretin-based drugs after Bariatric Surgery
An important and commonly asked concept: After gastric bypass (Roux-en-Y), patients with T2DM often experience near-complete remission of diabetes even before significant weight loss occurs. One key mechanism is the rapid delivery of nutrients to the distal ileum → massive surge of GLP-1 from L cells → greatly enhanced incretin effect.
8. Quick Recall Summary
| Parameter | Key Fact |
|---|---|
| Incretin effect | 60-70% of postprandial insulin from oral (vs. IV) glucose |
| Major incretins | GLP-1 (L cells, ileum/colon) + GIP (K cells, duodenum) |
| GLP-1 half-life | ~2 minutes (degraded by DPP-4 + renal clearance) |
| GLP-1 key actions | ↑ Insulin (glucose-dependent), ↓ Glucagon, ↓ gastric emptying, ↓ appetite, ↓ β-cell apoptosis |
| Incretin effect in T2DM | Markedly reduced |
| GLP-1 RA route | SC injection (except oral semaglutide) |
| Most potent weight loss GLP-1 RA | Semaglutide / Tirzepatide |
| First dual GLP-1+GIP agonist | Tirzepatide |
| Gliptin safe in renal failure | Linagliptin (hepatobiliary elimination) |
| Gliptin causing heart failure risk | Saxagliptin |
| GLP-1 RA contraindications | Medullary thyroid Ca, MEN2, pancreatitis |
| GLP-1 RA with proven CV benefit | Liraglutide, dulaglutide, semaglutide |
| Low hypoglycemia risk - why? | Insulin stimulation is GLUCOSE-DEPENDENT |
Sources: Katzung's Basic & Clinical Pharmacology 16e, p.1189 | Lippincott Pharmacology, p.808-818 | Goldman-Cecil Medicine | Harrison's Principles 22e | Guyton & Hall Medical Physiology | Textbook of Family Medicine 9e
Incretin
The previous response already covered incretins in full detail for a MUHS PG Medicine resident. Here's a clean, structured recap you can use directly for revision:
Incretins - MUHS PG Rapid Revision
The Core Concept
Incretin effect = Oral glucose produces 60-70% MORE insulin than the same amount given IV, because the gut releases hormones (incretins) that amplify pancreatic β-cell insulin secretion.
This effect is markedly reduced in T2DM - a core pathophysiological defect.
Two Incretin Hormones
| GLP-1 | GIP | |
|---|---|---|
| Full name | Glucagon-Like Peptide-1 | Glucose-Dependent Insulinotropic Polypeptide |
| Secreted by | L cells - distal ileum & colon | K cells - proximal duodenum/jejunum |
| Stimulus | Glucose, fat, protein | Glucose + fat |
| Half-life | ~2 minutes | ~2 minutes |
| Degraded by | DPP-4 enzyme + renal clearance | DPP-4 enzyme |
| In T2DM | Secretion impaired | Secretion near-normal but β-cell response impaired |
GLP-1 Actions - HIGH YIELD
| Target | Effect |
|---|---|
| Pancreas β-cell | ↑ Insulin secretion (glucose-dependent only) |
| Pancreas α-cell | ↓ Glucagon secretion |
| Stomach | ↓ Gastric emptying |
| Brain | ↓ Appetite / ↑ Satiety |
| β-cell | ↓ Apoptosis + ↑ Proliferation (β-cell preservation) |
| Heart | Cardioprotective |
Why low hypoglycemia risk? Insulin stimulation only occurs when glucose is elevated - switches off at normal glucose. Unlike sulfonylureas.
Why Can't We Use Native GLP-1 as a Drug?
Half-life is only ~2 minutes - DPP-4 degrades it almost immediately. Two solutions:
STRATEGY 1 → Give DPP-4-resistant GLP-1 analogues = GLP-1 Receptor Agonists
STRATEGY 2 → Block DPP-4 itself = DPP-4 Inhibitors (Gliptins)
Drug Class 1: GLP-1 Receptor Agonists (Incretin Mimetics)
Route: SC injection (peptides - destroyed orally) - except oral semaglutide
| Drug | Dose Frequency | Special Points |
|---|---|---|
| Exenatide | BD SC | From Gila monster venom; avoid severe renal failure |
| Exenatide XR | Once weekly SC | |
| Liraglutide | Once daily SC | LEADER trial - CV mortality ↓ in T2DM |
| Dulaglutide | Once weekly SC | CV benefit proven |
| Lixisenatide | Once daily SC | Short-acting |
| Semaglutide | Once weekly SC / once daily oral | Most potent; SELECT trial: 20% ↓ MACE even without diabetes (obesity + CVD); STEP-HFpEF: improved HFpEF |
| Tirzepatide | Once weekly SC | Dual GLP-1 + GIP agonist (first of class); greatest weight loss; FDA 2022 (T2DM), 2023 (obesity) |
HbA1c reduction: ~0.5-1.5%
Adverse effects:
- GI: Nausea, vomiting, diarrhea (most common, especially on initiation)
- Pancreatitis (avoid in h/o chronic pancreatitis)
- Thyroid C-cell tumors in rodents → contraindicated in medullary thyroid carcinoma + MEN2
- Weight loss (beneficial)
Do NOT combine with DPP-4 inhibitors (overlapping mechanism)
Drug Class 2: DPP-4 Inhibitors / "Gliptins" (Incretin Enhancers)
Route: Oral tablets
Mechanism: Block DPP-4 → endogenous GLP-1 + GIP survive longer → meal-dependent ↑ insulin + ↓ glucagon
Weight effect: Neutral (no weight loss unlike GLP-1 RAs)
| Drug | Key Exam Point |
|---|---|
| Sitagliptin | First approved; renal excretion; dose adjust in CKD |
| Saxagliptin | CYP3A4 metabolism; ↑ heart failure hospitalization risk |
| Alogliptin | Renal excretion |
| Linagliptin | Hepatobiliary elimination - NO dose adjustment in renal failure (only one safe in severe CKD) |
| Vildagliptin | Available in India/Europe |
Adverse effects:
- Nasopharyngitis, headache (most common)
- Pancreatitis (rare)
- Severe disabling arthralgia (class effect)
- Saxagliptin: ↑ heart failure hospitalizations
Incretin Defect in T2DM
Two abnormalities:
- GLP-1 secretion is impaired after oral carbohydrate
- β-cells are resistant to GIP (even though GIP levels are near-normal)
Result: Loss of the normal 60-70% incretin contribution → postprandial hyperglycemia
Bonus - Bariatric Surgery and Incretins
After Roux-en-Y gastric bypass, T2DM often remits before significant weight loss. Key mechanism: Rapid nutrient delivery to distal ileum → massive GLP-1 surge → restored incretin effect.
One-Line Exam Answers
| Question | Answer |
|---|---|
| What % of postprandial insulin is from incretins? | 60-70% |
| Which cells secrete GLP-1? | L cells (ileum/colon) |
| Which cells secrete GIP? | K cells (duodenum) |
| Why low hypoglycemia with GLP-1 RAs? | Glucose-dependent insulin release |
| Native GLP-1 half-life? | ~2 minutes (DPP-4 + renal clearance) |
| First dual GLP-1/GIP agonist? | Tirzepatide |
| Gliptin safe in severe CKD (no dose adjust)? | Linagliptin |
| Gliptin increasing heart failure risk? | Saxagliptin |
| GLP-1 RA contraindicated in? | Medullary thyroid Ca + MEN2 |
| GLP-1 RAs with proven CV benefit? | Liraglutide, Dulaglutide, Semaglutide |
| Incretin effect in T2DM? | Markedly reduced/blunted |
Explain this as saq for 15 marks
Here is a model 15-mark SAQ answer on Incretins, written exactly as you should present it in a MUHS PG exam - structured, point-wise, with subheadings, and covering all scorable points.
INCRETINS
(Short Answer Question - 15 Marks)
Definition / Introduction (1 mark)
Incretins are gut-derived peptide hormones released in response to food ingestion that amplify glucose-stimulated insulin secretion from pancreatic β-cells in a glucose-dependent manner.
The "Incretin Effect" refers to the observation that an oral glucose load produces 60-70% more insulin than an equivalent intravenous glucose load - due to simultaneous release of incretin hormones from the gut.
This effect is markedly blunted in Type 2 Diabetes Mellitus (T2DM).
Incretin Hormones (2 marks)
Two major incretin hormones:
1. GLP-1 (Glucagon-Like Peptide-1)
- Secreted by L cells of distal ileum and colon
- Released within minutes of eating
- Fasting level: 5-10 pmol/L → rises to 15-50 pmol/L postprandially
- Half-life: ~2 minutes (degraded by DPP-4 enzyme + renal clearance)
2. GIP (Glucose-Dependent Insulinotropic Polypeptide)
- Secreted by K cells of proximal duodenum and jejunum
- Released in response to glucose + fat (fat is a stronger stimulus)
- Also degraded by DPP-4
Actions of Incretins (3 marks)
GLP-1 Actions (multi-organ):
| Organ | Action |
|---|---|
| Pancreas β-cell | ↑ Insulin secretion (glucose-dependent only) |
| Pancreas α-cell | ↓ Glucagon secretion |
| Stomach | ↓ Gastric emptying → slows glucose absorption |
| Brain/CNS | ↓ Appetite, ↑ Satiety, ↓ food intake |
| β-cell trophic | ↓ β-cell apoptosis, ↑ β-cell proliferation |
| Cardiovascular | Cardioprotective (reduces MACE in CVD) |
GIP Actions:
- ↑ Glucose-dependent insulin secretion
- ↑ Triglyceride storage in adipose tissue
- In T2DM: β-cell response to GIP is impaired even though secretion is near-normal
Key point: Insulin stimulation by incretins is glucose-dependent - it is activated when glucose is elevated and switches off at normal levels. This is why incretin-based drugs carry a low risk of hypoglycemia.
Incretin Defect in T2DM (1 mark)
Two abnormalities exist in T2DM:
- GLP-1 secretion is impaired after oral carbohydrate (blunted L-cell response)
- β-cell resistance to GIP - even though GIP levels are near-normal, the β-cell fails to respond
Result: Loss of 60-70% incretin contribution → postprandial hyperglycemia
Incretin-Based Drugs (8 marks)
Two pharmacological strategies exploit the incretin system:
Strategy 1: GLP-1 Receptor Agonists (Incretin Mimetics)
Rationale: Native GLP-1 has t½ ~2 min and cannot be used therapeutically. DPP-4-resistant analogues are synthesized that mimic or exceed GLP-1's effects.
Route: Subcutaneous injection (peptides) - except oral semaglutide
Mechanism: Bind and activate GLP-1 receptors → ↑ glucose-dependent insulin, ↓ glucagon, ↓ gastric emptying, ↓ appetite, β-cell preservation
| Drug | Frequency | Key Points |
|---|---|---|
| Exenatide | BD SC | Derived from Gila monster venom (exendin-4); avoid in severe renal failure |
| Exenatide XR | Once weekly SC | Extended-release microspheres |
| Liraglutide | Once daily SC | LEADER trial - ↓ CV mortality in T2DM with CVD |
| Dulaglutide | Once weekly SC | CV benefit proven (REWIND trial) |
| Lixisenatide | Once daily SC | Short-acting |
| Semaglutide | Once weekly SC / once daily oral | Most potent; SELECT trial: 20% ↓ MACE even in non-diabetic obese patients with CVD; STEP-HFpEF: improved HFpEF symptoms |
| Tirzepatide | Once weekly SC | First dual GLP-1 + GIP agonist; greatest weight loss; FDA approved T2DM (2022) and obesity (2023) |
HbA1c reduction: ~0.5-1.5%
Adverse Effects:
- GI: Nausea, vomiting, diarrhea, constipation (most common, especially on initiation)
- Pancreatitis (avoid in history of chronic pancreatitis)
- Thyroid C-cell tumors (rodents) → Contraindicated in medullary thyroid carcinoma and MEN type 2
- Weight loss (beneficial in obese T2DM)
Strategy 2: DPP-4 Inhibitors / "Gliptins" (Incretin Enhancers)
Rationale: Block DPP-4 enzyme → prevent degradation of endogenous GLP-1 and GIP → prolonged incretin effect
Route: Oral tablets
Weight effect: Weight neutral (unlike GLP-1 RAs)
| Drug | Key Exam Point |
|---|---|
| Sitagliptin | First approved; renal excretion; dose reduce in CKD |
| Saxagliptin | CYP3A4 metabolism; ↑ heart failure hospitalization risk - avoid in heart failure |
| Alogliptin | Renal excretion; dose adjust in CKD |
| Linagliptin | Hepatobiliary elimination → NO dose adjustment in renal failure (only DPP-4 inhibitor safe in severe CKD without dose adjustment) |
| Vildagliptin | Available in India and Europe |
HbA1c reduction: ~0.5-0.8%
Adverse Effects:
- Nasopharyngitis, headache (most common)
- Pancreatitis (rare but serious)
- Severe, disabling arthralgia (joint pain - class effect)
- Hypersensitivity reactions
- Saxagliptin: ↑ heart failure hospitalizations
Important combination note: GLP-1 RAs + DPP-4 inhibitors should NOT be combined - overlapping mechanism of action + increased toxicity risk.
Clinical Applications Beyond Diabetes (1 mark)
- Obesity: Semaglutide 2.4 mg/week approved for chronic weight management; Tirzepatide 5/10/15 mg/week approved for obesity
- Bariatric surgery: Post-Roux-en-Y gastric bypass, rapid nutrient delivery to distal ileum → massive GLP-1 surge → T2DM remission before significant weight loss
- HFpEF: Semaglutide improved heart failure symptoms and reduced inflammation (STEP-HFpEF trial)
- CKD: GLP-1 RAs show emerging renoprotective benefits (FLOW trial with semaglutide)
Summary Box (for quick recall)
| Parameter | Key Fact |
|---|---|
| Incretin contribution to postprandial insulin | 60-70% |
| GLP-1 secreting cells | L cells (ileum/colon) |
| GIP secreting cells | K cells (duodenum) |
| Half-life of native GLP-1 | ~2 minutes |
| Why low hypoglycemia risk? | Glucose-dependent insulin release |
| First dual GLP-1/GIP agonist | Tirzepatide |
| Gliptin safe in severe CKD | Linagliptin |
| Gliptin increasing HF risk | Saxagliptin |
| GLP-1 RA contraindicated in | Medullary thyroid Ca + MEN2 |
| GLP-1 RAs with proven CV benefit | Liraglutide, Dulaglutide, Semaglutide |
Word to the wise for MUHS exams: Draw the DPP-4 mechanism as a small diagram showing Meal → GLP-1/GIP released → DPP-4 degrades them → Gliptin blocks DPP-4 → prolonged incretin effect. Examiners reward diagrams in pharmacology SAQs.
Explain it as saq to me
Asking for Preferences
Got it - same topic, 15 marks. The previous response already gave you a fully structured 15-mark SAQ answer. But I understand you want it written as you would actually write it in the exam hall - flowing prose with subheadings, no tables, the way a MUHS examiner expects it. Here it is:
SAQ: INCRETINS (15 Marks)
Definition
Incretins are gut-derived peptide hormones released in response to food ingestion that amplify glucose-stimulated insulin secretion from pancreatic β-cells in a glucose-dependent manner.
The "Incretin Effect" is defined as the observation that an oral glucose load produces 60-70% more insulin than an equivalent intravenous glucose load. This amplification occurs because oral ingestion of glucose triggers the simultaneous release of incretin hormones from intestinal cells, which potentiate pancreatic insulin secretion.
This effect is markedly blunted in Type 2 Diabetes Mellitus (T2DM), making it a key pathophysiological target.
Incretin Hormones
There are two major incretin hormones:
1. GLP-1 (Glucagon-Like Peptide-1)
- Secreted by L cells of the distal ileum and colon
- Released within minutes of eating, before digested food even reaches L cells (via neurohormonal signals)
- Fasting plasma level: 5-10 pmol/L, rising to 15-50 pmol/L postprandially
- Half-life: approximately 2 minutes - rapidly inactivated by the enzyme DPP-4 and cleared by the kidneys
2. GIP (Glucose-Dependent Insulinotropic Polypeptide)
- Secreted by K cells of the proximal duodenum and jejunum
- Released in response to glucose and fat (fat is a stronger stimulus for GIP than for GLP-1)
- Also rapidly degraded by DPP-4
Physiological Actions
Actions of GLP-1 (clinically most important):
GLP-1 acts on multiple organ systems:
- Pancreatic β-cells: Stimulates insulin secretion in a strictly glucose-dependent manner. This means insulin is released only when blood glucose is elevated - the effect attenuates at normal glucose levels. This is the basis for the low hypoglycemia risk of GLP-1-based drugs.
- Pancreatic α-cells: Suppresses inappropriate glucagon secretion, thereby reducing hepatic glucose output.
- Stomach: Delays gastric emptying, slowing the rate of glucose absorption and blunting postprandial glucose spikes.
- Brain/CNS: Acts centrally to reduce appetite and increase satiety, leading to reduced food intake and weight loss.
- β-cell preservation: Reduces β-cell apoptosis and promotes β-cell proliferation, potentially preserving β-cell mass over time.
- Cardiovascular: Cardioprotective effects demonstrated in multiple clinical trials.
Actions of GIP:
- Stimulates glucose-dependent insulin secretion (similar to GLP-1)
- Promotes triglyceride storage in adipose tissue
- In T2DM, even though GIP secretion is relatively preserved, the β-cell response to GIP is impaired
Incretin Defect in T2DM
In T2DM, two specific abnormalities exist in the incretin system:
- GLP-1 secretion is reduced after oral carbohydrate ingestion (impaired L-cell function)
- β-cell resistance to GIP - β-cells fail to respond adequately to GIP even when GIP levels are near-normal
The net result is loss of the normal 60-70% incretin contribution to postprandial insulin secretion, which significantly worsens postprandial hyperglycemia.
Pharmacological Exploitation - Incretin-Based Drugs
Since native GLP-1 has a half-life of only ~2 minutes, it cannot be used as a drug directly. Two strategies have been developed:
Strategy 1: GLP-1 Receptor Agonists (Incretin Mimetics)
These are synthetic, DPP-4-resistant analogues of GLP-1 that bind and activate the GLP-1 receptor. They reproduce all actions of endogenous GLP-1.
Since they are peptides, they must be given by subcutaneous injection (destroyed by oral route) - with the exception of oral semaglutide.
Drugs and key features:
- Exenatide (twice daily SC): Derived from exendin-4, a peptide found in Gila monster venom, with 53% homology to human GLP-1. Should be avoided in severe renal impairment.
- Liraglutide (once daily SC): LEADER trial demonstrated reduction in cardiovascular mortality in T2DM patients with established CVD.
- Dulaglutide (once weekly SC): Proven cardiovascular benefit (REWIND trial).
- Semaglutide (once weekly SC or once daily oral): Most potent GLP-1 RA. The SELECT trial showed a 20% reduction in MACE even in overweight/obese patients without diabetes who had established CVD. STEP-HFpEF trial showed improvement in HFpEF symptoms and reduction in inflammation. Also approved for chronic weight management at 2.4 mg weekly.
- Tirzepatide (once weekly SC): The first dual GLP-1 and GIP receptor agonist. Engineered from native GIP sequence with affinity for both receptors. Produces greater weight loss than GLP-1 RAs alone. FDA approved for T2DM in 2022 and obesity in 2023.
HbA1c reduction: 0.5-1.5%
Adverse effects:
- Gastrointestinal effects (nausea, vomiting, diarrhea, constipation) are the most common, especially on initiation - usually transient
- Pancreatitis - avoid in patients with history of chronic pancreatitis
- Thyroid C-cell tumors seen in rodent studies → Contraindicated in medullary thyroid carcinoma and MEN type 2
- Weight loss occurs as a beneficial side effect
Strategy 2: DPP-4 Inhibitors / Gliptins (Incretin Enhancers)
These are oral drugs that inhibit the DPP-4 enzyme, thereby preventing the degradation of endogenously released GLP-1 and GIP. This prolongs the incretin effect after meals, increasing glucose-dependent insulin secretion and reducing glucagon.
They are weight neutral (no weight loss unlike GLP-1 RAs) and well tolerated.
Drugs and key features:
- Sitagliptin: First DPP-4 inhibitor approved. Renally excreted - dose reduction required in CKD.
- Saxagliptin: Metabolized via CYP3A4. Important: associated with increased risk of heart failure hospitalization - should be avoided in patients with or at risk for heart failure.
- Alogliptin: Renally excreted - dose adjustment in CKD.
- Linagliptin: Eliminated via hepatobiliary route. Only DPP-4 inhibitor that does not require dose adjustment in renal failure, making it the preferred gliptin in patients with severe CKD.
- Vildagliptin: Available in India and Europe.
HbA1c reduction: 0.5-0.8%
Adverse effects:
- Nasopharyngitis and headache (most common)
- Pancreatitis (rare but serious)
- Severe, disabling arthralgia - a class effect; can be debilitating
- Hypersensitivity reactions
- Saxagliptin specifically: increased heart failure hospitalizations
Important: GLP-1 RAs and DPP-4 inhibitors should not be combined - overlapping mechanism and increased toxicity risk without additive glucose benefit.
Beyond Diabetes - Emerging Uses
- Obesity management: Semaglutide 2.4 mg/week and tirzepatide approved for chronic weight management
- Post-bariatric surgery remission of T2DM: Roux-en-Y gastric bypass causes rapid delivery of nutrients to the distal ileum → massive GLP-1 surge → T2DM remission before major weight loss occurs
- Heart failure (HFpEF): Semaglutide reduces symptoms and inflammation in HFpEF patients
- CKD: GLP-1 RAs show emerging renoprotective benefits
Conclusion
Incretins represent a physiologically elegant mechanism where the gut communicates with the pancreas to optimise postprandial glucose control. Their deficiency in T2DM has led to two major drug classes - GLP-1 RAs and DPP-4 inhibitors - that exploit this pathway with low hypoglycemia risk and additional cardioprotective and weight-reducing benefits, making them cornerstones of modern T2DM management.
Diagram to draw in exam:
MEAL INGESTED
↓
Gut releases GLP-1 (L cells) + GIP (K cells)
↓
DPP-4 enzyme degrades them (t½ ~2 min)
↓
Two drug strategies:
┌─────────────────────┐ ┌──────────────────────┐
│ GLP-1 RA │ │ DPP-4 Inhibitor │
│ (DPP-4 resistant │ │ (blocks DPP-4 → │
│ GLP-1 analogue) │ │ ↑ endogenous GLP-1) │
└─────────────────────┘ └──────────────────────┘
Both → ↑ Glucose-dependent insulin + ↓ Glucagon
This diagram alone can fetch you 1-2 marks in a MUHS SAQ.
This is a shared conversation. Sign in to Orris to start your own chat.