Treatment of gerd in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"gastroesophageal reflux disease" AND treatment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from multiple authoritative textbooks. I have enough to write a thorough, well-organized answer. Let me compose the complete response.
Treatment of Gastroesophageal Reflux Disease (GERD)
GERD is a chronic condition arising from retrograde flow of gastric contents into the esophagus due to failure of the lower esophageal sphincter (LES) complex. Treatment is stepwise, targeting lifestyle, pharmacology, and surgery based on symptom severity and response.
1. Lifestyle Modifications
Lifestyle changes are first-line and should accompany all pharmacological therapy. Evidence for individual interventions is generally modest, but they should be tailored to each patient's triggers.
Three categories of recommendations (Yamada's Textbook of Gastroenterology, 7e):
| Category | Specific Measures |
|---|---|
| Avoid LES-relaxing foods | Coffee, alcohol, chocolate, fatty foods, peppermint |
| Avoid direct esophageal irritants | Citrus, carbonated drinks, spicy foods, onions, garlic |
| Behavioral/positional | Weight loss, smoking cessation, elevate head of bed 6-10 inches, no food 2-3 hours before lying down, limit bending/heavy lifting |
Weight loss deserves special emphasis. There is a dose-dependent relationship between increasing BMI and reflux symptoms. Even patients with a BMI in the normal range (19-25) can develop GERD symptoms with moderate weight gain, which resolves on weight loss. If heartburn developed in parallel with weight gain, weight reduction may eliminate the need for ongoing acid-suppressive therapy. - Fischer's Mastery of Surgery, 8e
2. Pharmacological Treatment
Step-Up vs. Step-Down Approach
Either approach can be used with titration to symptoms. A 6-8 week trial of a daily or twice-daily PPI taken 30 minutes before a meal is the standard empiric treatment. Over half of patients use PPIs incorrectly (too early before a meal, or only as needed), so adherence counseling is important. - Fischer's Mastery of Surgery, 8e
A. Antacids and Alginates
- Antacids neutralize intragastric acid without suppressing subsequent secretion - they provide rapid but short-lived relief.
- The concept of the acid pocket (a layer of newly secreted acid on top of the ingested meal, appearing within 20 minutes of eating) has revived interest in alginate-antacid combinations.
- Alginates (e.g., Gaviscon): natural polysaccharide polymers that precipitate into a viscous gel on contact with gastric acid. The sodium bicarbonate within the formulation releases CO2 which floats the gel on top of gastric contents, displacing the acid pocket and reducing postprandial reflux. - Yamada's Gastroenterology, 7e
- Hyaluronic acid-chondroitin sulfate (Esoxx): forms a protective barrier on the esophageal mucosa. When combined with acid suppression, 53% of NERD patients had symptom relief vs. 32% with acid suppression alone (p < 0.01).
Role: On-demand or adjunctive therapy for mild/intermittent symptoms; not suitable for maintenance in erosive disease.
B. Histamine-2 Receptor Antagonists (H2RAs)
- Competitively block histamine-stimulated H2 receptors on parietal cells
- Less potent than PPIs; duration of action parallels serum half-life
- Tachyphylaxis develops rapidly with continuous use
- PPIs are superior to H2RAs for healing erosive esophagitis
- H2RAs remain useful for nocturnal acid breakthrough on PPI therapy (added at bedtime)
- Agents: ranitidine (withdrawn in many countries due to NDMA), famotidine, cimetidine, nizatidine
C. Proton Pump Inhibitors (PPIs) - First-Line Therapy
PPIs covalently bind to the gastric H+/K+-ATPase (proton pump), blocking the final common pathway of acid secretion. They are the most potent acid-suppressive agents available.
Agents: omeprazole, lansoprazole, pantoprazole, rabeprazole, esomeprazole, dexlansoprazole
Efficacy by GERD manifestation (Yamada's Gastroenterology, 7e):
| Manifestation | PPI Efficacy |
|---|---|
| Erosive esophagitis | Close to 100% healing; clear dose-response curve; higher doses more effective |
| Heartburn (erosive) | Good response, therapeutic gain higher with erosive disease |
| Heartburn (NERD) | 10-20% lower therapeutic gain than erosive; still first-line |
| Regurgitation | Lower therapeutic gain than heartburn; <50% complete response |
| Dysphagia without stricture | 83% resolution with PPI therapy |
| Extraesophageal (cough, laryngitis, asthma) | Variable; empiric PPI trial warranted |
Key prescribing principles:
- Take 30-60 minutes before a meal (to allow absorption and activation during the active secretory phase)
- Standard course: 4-8 weeks for initial healing; maintenance therapy for moderate-severe/erosive disease
- For Barrett's esophagus: once-daily PPI maintenance recommended by ACG guidelines for chemoprevention (reduces risk of high-grade dysplasia/adenocarcinoma; adjusted OR 0.29) - Sleisenger & Fordtran's GI and Liver Disease
On-demand therapy: Appropriate for mild-moderate symptoms once healing achieved. Reduces long-term PPI burden.
PPI side effects (long-term considerations):
- Hypomagnesemia
- Increased risk of Clostridioides difficile infection
- Possible reduction in clopidogrel efficacy (CYP2C19 interaction, mainly omeprazole/esomeprazole)
- Vitamin B12 and iron malabsorption (with prolonged use)
- Bone density reduction (long-term high-dose)
- Community-acquired pneumonia (modest increased risk)
D. Prokinetics
- Augment esophageal peristalsis and improve gastric emptying, reducing reflux volume
- Metoclopramide: dopamine antagonist - limited long-term use due to tardive dyskinesia risk
- Domperidone: less CNS penetration than metoclopramide; used in some countries
- Baclofen: GABA-B agonist that reduces transient LES relaxations (TLESRs) - used in refractory GERD and as add-on to PPIs for persistent regurgitation
- Prokinetics are generally adjuncts, not monotherapy
E. Reflux Inhibitors
- Baclofen (GABA-B agonist): reduces TLESR frequency - the dominant mechanism of reflux in most patients. Used in refractory regurgitation when PPI response is incomplete. Dose-limited by CNS side effects (dizziness, somnolence).
3. Treatment Algorithm
Here is the evidence-based management algorithm from Yamada's Gastroenterology:
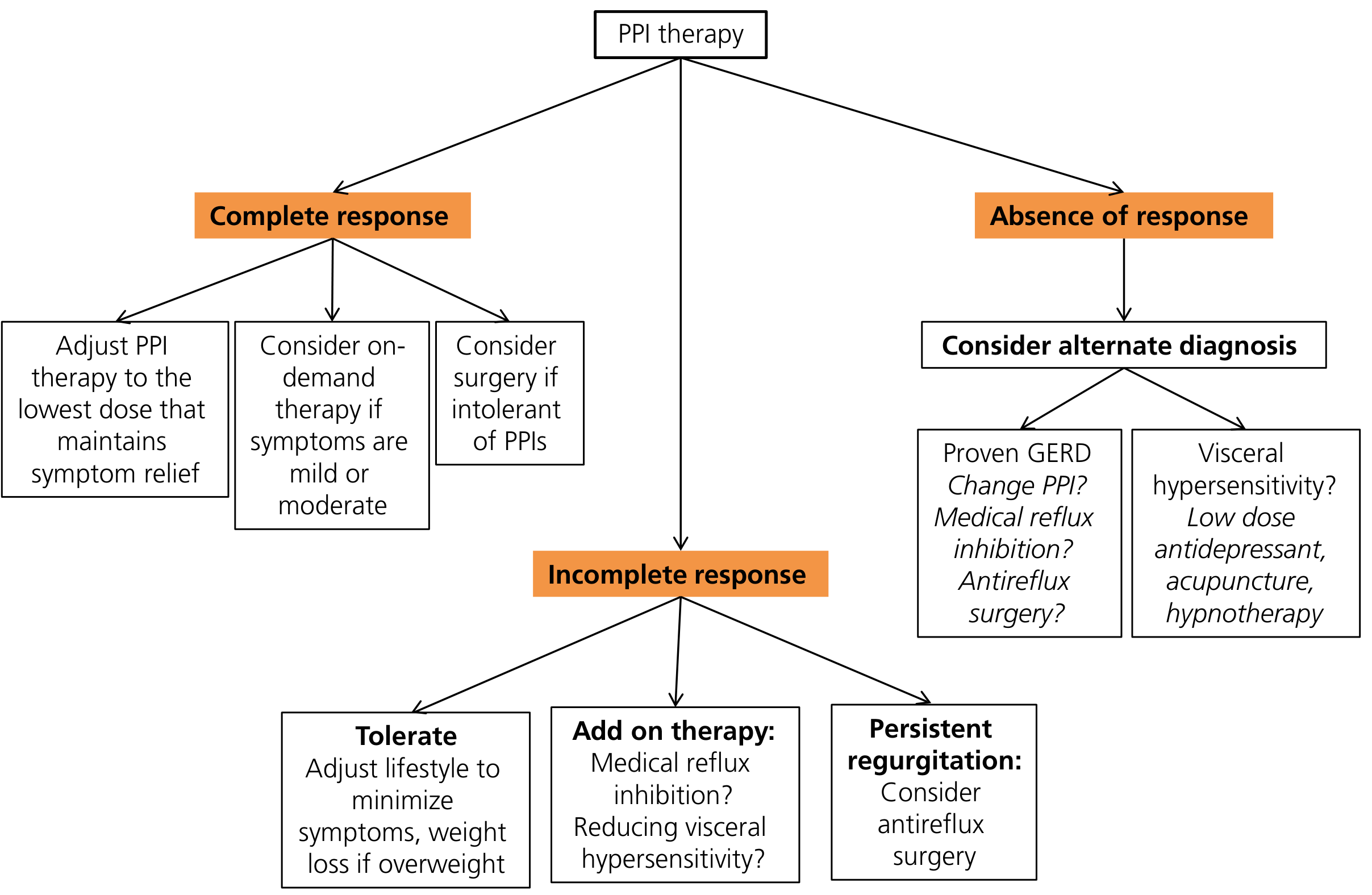
Complete response to PPI:
- Adjust to lowest effective dose
- Consider on-demand therapy if symptoms are mild-moderate
- Consider antireflux surgery if PPI-intolerant
Incomplete response to PPI:
- Tolerate: lifestyle adjustment, weight loss
- Add-on therapy: baclofen (reflux inhibition), address visceral hypersensitivity
- Persistent regurgitation: consider antireflux surgery
No response at all:
- Reconsider diagnosis - proven GERD? Change PPI? Surgery?
- If visceral hypersensitivity predominates: low-dose antidepressant, acupuncture, hypnotherapy
4. Surgical Treatment - Antireflux Surgery (ARS)
Surgical therapy recreates the gastroesophageal flap valve by reinforcing the diaphragmatic crura and wrapping the gastric fundus around the LES.
Indications
-
Medically refractory symptoms
-
Patient preference (desire to stop long-term PPIs)
-
Barrett's esophagus with ongoing symptomatic reflux
-
Extraesophageal complications (laryngopharyngeal reflux, aspiration, pulmonary disease) - antireflux surgery improves respiratory symptoms in ~90% of children and ~70% of adults with asthma and GERD
-
Medication intolerance/noncompliance
-
Young patients averse to lifelong pharmacotherapy
-
Fischer's Mastery of Surgery, 8e; Maingot's Abdominal Operations
Procedures
Laparoscopic Nissen fundoplication (360°): Gold standard. The gastric fundus is wrapped 360° around the distal esophagus. Most effective at controlling heartburn and regurgitation.
Laparoscopic Toupet fundoplication (270° posterior wrap): Preferred in patients with impaired esophageal motility to reduce risk of postoperative dysphagia.
Partial fundoplications (Dor - anterior 180°): Less common; used when peristalsis is compromised.
LOTUS Trial Evidence
The LOTUS trial (large European RCT comparing laparoscopic antireflux surgery vs. esomeprazole for chronic GERD) showed:
- Both treatments similarly effective in achieving complete symptom remission at 3 years
- At 5 years: remission rates 92% (esomeprazole) vs. 85% (fundoplication), p=0.048
- Regurgitation was significantly better controlled surgically (13% surgical vs. 2% medical failure, p<0.001)
- Dysphagia, bloating, flatulence: more common in fundoplication group
Yamada's Gastroenterology, 7e
Contraindications to Surgery
- Absolute: Absent esophageal peristalsis (e.g., scleroderma)
- Relative: Severe esophagitis with stricture, short esophagus, prior upper abdominal surgery, severe peristaltic dysfunction
- Pre-operative esophageal manometry is mandatory to exclude achalasia and assess peristaltic function
Surgical Complications/Risks
- Dysphagia (most common postoperative complaint)
- Gas-bloat syndrome (inability to belch, flatulence)
- Diarrhea, bowel symptoms
- Recurrence: ~30% resume PPI therapy within 5 years in community practice
- Revision surgery needed in up to 50% at referral centers
5. Endoscopic Therapies
Several endoscopic approaches for GERD have been introduced but none has achieved efficacy equivalent to antireflux surgery (Maingot's Abdominal Operations):
- Radiofrequency ablation at the LES (Stretta procedure): Delivers RF energy to the LES to increase muscle bulk/reduce TLESR. Improves heartburn but not acid exposure on pH testing.
- Transoral incisionless fundoplication (TIF/EsophyX): Endoscopic reconstruction of the flap valve. Suitable for small hiatal hernias; inferior to surgical fundoplication for severe GERD.
- LINX device (magnetic sphincter augmentation): A ring of magnetic beads implanted laparoscopically around the GEJ. Opens with swallowing pressure; prevents reflux at rest. Reversible. Contraindicated in MRI-dependent patients (older models) and nickel allergy.
6. Special Populations
Barrett's Esophagus
- Maintain PPI therapy indefinitely (ACG guideline) for chemoprevention
- Fundoplication is not superior to medical therapy for cancer prevention based on meta-analyses (IRR 0.76 for surgery vs. medical, overall effect similar)
- Patients with Barrett's may be rendered asymptomatic by PPIs while still having pathological acid exposure - pH monitoring may be needed to confirm adequate control
- Sleisenger & Fordtran's GI and Liver Disease
Pediatric GERD
- Infants: formula thickening, volume reduction, positional adjustments first
- Pharmacological acid suppression as next step
- Fundoplication reserved for life-threatening complications (apnea, severe aspiration, failure to thrive refractory to medical therapy)
- Age-appropriate dosing; H2RAs and PPIs both used
- Sabiston Textbook of Surgery, 21e
GERD in Athletes
- Particularly worsens with endurance and high-intensity exercise (exercise-induced LES relaxation)
- Avoid aggravating foods, solid food 3 hours before exercise, adequate hydration
- PPIs are effective and do not affect performance
- Textbook of Family Medicine, 9e
Summary Table
| Treatment | Class | Use Case | Notes |
|---|---|---|---|
| Lifestyle changes | Non-pharmacological | All patients | Weight loss most impactful |
| Antacids/alginates | Acid neutralization | Mild/on-demand | Target acid pocket |
| H2RAs | Acid suppression | Mild-moderate; nocturnal breakthrough | Tachyphylaxis limits chronic use |
| PPIs | Acid suppression | First-line, all grades | Take 30 min before meals |
| Baclofen | Reflux inhibitor | PPI-refractory regurgitation | TLESR reduction |
| Nissen/Toupet fundoplication | Surgery | Refractory/PPI-intolerant | Pre-op manometry mandatory |
| LINX device | Endoscopic/laparoscopic | Moderate GERD, no large hernia | Reversible; MRI precautions |
| TIF/Stretta | Endoscopic | Mild-moderate; PPI-averse | Inferior to surgery |
Sources: Yamada's Textbook of Gastroenterology, 7e | Sleisenger & Fordtran's GI and Liver Disease | Fischer's Mastery of Surgery, 8e | Maingot's Abdominal Operations | Sabiston Textbook of Surgery, 21e | Textbook of Family Medicine, 9e
This is a shared conversation. Sign in to Orris to start your own chat.