Aphasia and dysarthria internal medicine
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching PubMed
aphasia dysarthria stroke management rehabilitation
I have all the content I need to deliver a comprehensive, authoritative answer. Let me now compile the full response.
Aphasia and Dysarthria - Internal Medicine Overview
Definitions and Key Distinction
Aphasia is a disorder of language - the complex system of communicative symbols - acquired secondary to brain damage. It is distinct from motor speech disorders. Dysarthria is a disorder of muscular control of speech - the mechanics of articulation and phonation - without primary impairment of the language system itself.
This distinction is clinically critical:
- In aphasia: the patient cannot properly form or comprehend language, but the speech muscles may be intact.
- In dysarthria: the patient knows what they want to say but cannot physically articulate it clearly; reading, writing, and comprehension are preserved in pure cases.
"Aphasia is distinguished from motor speech disorders, which include dysarthria, dysphonia, stuttering, and apraxia of speech. Dysarthrias are disorders of muscular control of speech." - Bradley and Daroff's Neurology in Clinical Practice
Language Network Anatomy
The left perisylvian region of the dominant hemisphere houses the core language network. Two key hubs:
- Broca's area (posterior inferior frontal gyrus, Brodmann area 44/45): governs verbal fluency and grammatical structure
- Wernicke's area (temporoparietal junction / posterior superior temporal gyrus): governs language comprehension and word meaning
These are connected by the arcuate fasciculus. Damage to this network produces aphasias. ~90% of right-handers are left-hemisphere dominant for language.
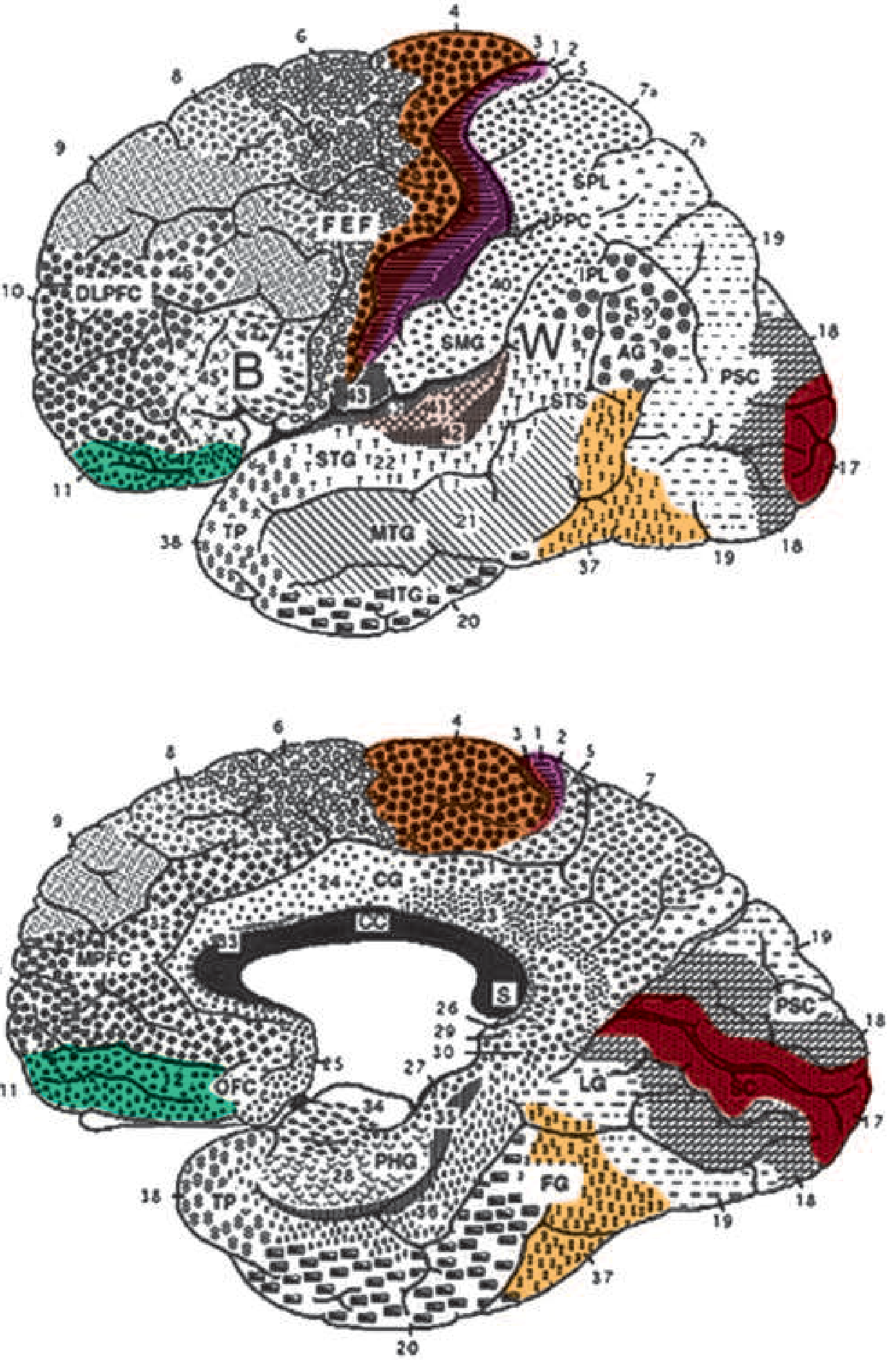
Lateral (top) and medial (bottom) views of the cerebral hemisphere with language network areas. B = Broca's area; W = Wernicke's area; AG = angular gyrus; SMG = supramarginal gyrus; STG = superior temporal gyrus - Harrison's Principles of Internal Medicine 22E
Classification of Aphasia
The most useful bedside approach examines four parameters:
- Fluency of spontaneous speech
- Comprehension
- Repetition
- Naming
1. Broca Aphasia (Expressive / Nonfluent)
| Feature | Finding |
|---|---|
| Spontaneous speech | Nonfluent, telegraphic ("wife come hospital"), often mute acutely |
| Naming | Impaired (tip-of-tongue phenomenon) |
| Comprehension | Relatively intact (mild difficulty with complex syntax) |
| Repetition | Impaired |
| Reading | Often impaired |
| Writing | Impaired (dysmorphic, dysgrammatical) |
| Associated signs | Right hemiparesis, hemisensory loss, ± left limb apraxia |
Lesion: Posterior inferior frontal gyrus (classic Broca area) + adjacent cortex.
Psychiatric note: Patients are typically aware of their deficit and commonly develop depression. This may limit rehabilitation.
2. Wernicke Aphasia (Receptive / Fluent)
| Feature | Finding |
|---|---|
| Spontaneous speech | Fluent, sometimes logorrheic; paraphasias, neologisms, jargon |
| Naming | Impaired (bizarre paraphasic substitutions) |
| Comprehension | Impaired (even for simple questions) |
| Repetition | Impaired |
| Reading | Impaired comprehension |
| Writing | Fluent but paragraphic; spelling errors |
| Associated signs | ± Right hemianopia; motor/sensory signs usually absent |
Lesion: Posterior superior temporal gyrus (classic Wernicke area).
Psychiatric note: Unlike Broca aphasia, patients are often unaware of their deficit (anosognosia) and may become paranoid.
3. Conduction Aphasia
Fluent speech with paraphasic errors, intact comprehension, but severely impaired repetition. The disconnection of Wernicke's area from Broca's area via the arcuate fasciculus is the classical explanation.
4. Global Aphasia
Combined dysfunction of both Broca's and Wernicke's areas. Speech is nonfluent, comprehension severely impaired, repetition impaired. Usually follows large MCA territory strokes. Associated with right hemiplegia, hemisensory loss, and homonymous hemianopia.
5. Transcortical Aphasias
- Transcortical Motor (Anterior): Similar to Broca's aphasia but repetition is intact. Lesion isolates language network from prefrontal areas (anterior watershed zone or supplementary motor cortex).
- Transcortical Sensory (Posterior): Similar to Wernicke's aphasia but repetition is intact. Lesion isolates language network from temporoparietal association areas. May show echolalia.
- Isolation Aphasia: Combination - comprehension impaired, no purposeful speech, but repetition/echolalia preserved. Associated with anoxia, CO poisoning, or watershed infarctions.
6. Anomic Aphasia
The "minimal dysfunction" syndrome. Articulation, comprehension, and repetition are intact, but confrontation naming and word-finding are impaired. Circumlocutious speech. Most common language disturbance in head trauma, metabolic encephalopathy, and Alzheimer's disease.
7. Subcortical Aphasia
Damage to the striatum or thalamus of the left hemisphere produces mixed, atypical syndromes. Clinical clue: In a CVA patient, anomic aphasia + dysarthria, or fluent aphasia + hemiparesis, should raise suspicion of a subcortical lesion. - Harrison's 22E
Summary Table
| Type | Fluency | Comprehension | Repetition | Lesion |
|---|---|---|---|---|
| Broca | Nonfluent | Intact | Impaired | Posterior inferior frontal (B area) |
| Wernicke | Fluent | Impaired | Impaired | Posterior superior temporal (W area) |
| Conduction | Fluent | Intact | Severely impaired | Arcuate fasciculus |
| Global | Nonfluent | Impaired | Impaired | Large MCA territory |
| Transcortical motor | Nonfluent | Intact | Intact | Anterior watershed / SMA |
| Transcortical sensory | Fluent | Impaired | Intact | Posterior watershed |
| Anomic | Fluent | Intact | Intact | Anywhere in L hemisphere network |
Dysarthria
In pure dysarthria (or anarthria at its extreme), cortical language mechanisms are normal - the patient understands speech, can read and write, but cannot produce intelligible spoken words. There are five main types:
1. Lower Motor Neuron (Neuromuscular) Dysarthria
- Cause: Disease of motor nuclei of medulla/lower pons, cranial nerves, neuromuscular junction, or articulatory muscles.
- Features: Shriveled, fasciculating tongue; lax/tremulous lips; drooling; dysphonia (rasping monotone from vocal cord paralysis); progressive loss of consonant enunciation - especially vibratives (r), labials (p, b), and linguals.
- Nasality from palatal paralysis: historically diphtheria/polio, now most commonly motor neuron disease (progressive bulbar palsy) and myasthenia gravis.
- Causes: ALS (bulbar form), myasthenia gravis, Guillain-Barré syndrome, Lyme disease, sarcoidosis.
2. Spastic (Pseudobulbar) Dysarthria
- Cause: Bilateral corticobulbar tract disease (vascular, demyelinating, or MND).
- Features: Slow, strained speech; high-pitched monotone; exaggerated jaw jerk and facial reflexes; no atrophy or fasciculations; pseudobulbar affect (emotional lability - pathological crying/laughing).
- Causes: Bilateral cortical strokes, MS, ALS (corticobulbar involvement), pontine strokes.
3. Rigid (Extrapyramidal) Dysarthria
- Cause: Extrapyramidal disease (basal ganglia / Parkinson's).
- Features: Rapid, mumbling, cluttered speech; hypophonia (low-pitched, soft, monotone); words trail off at sentence end; festination of speech. Almost opposite to spastic dysarthria.
- Causes: Parkinson's disease (hypokinetic dysarthria), progressive supranuclear palsy (spastic in PSP), Wilson disease.
4. Hyperkinetic Dysarthria
- Cause: Chorea, myoclonus.
- Features: Loud, harsh, poorly stressed; abrupt interruptions by involuntary inspirations and bulbar muscle movements - "hiccup speech". Unexpected breaks during words.
- Causes: Huntington's disease, Tourette syndrome (coprolalia, vocalizations), myoclonus.
5. Ataxic (Cerebellar) Dysarthria
- Cause: Cerebellar lesions.
- Features: Slow, slurred, monotonous; unnatural syllable separation; erratic coordination of speech and respiration; explosive speech (excess force on some syllables); scanning dysarthria (metronomic, poetry-scanning pattern - most often from mesencephalic lesions).
- Causes: Multiple sclerosis, cerebellar degenerations, anoxic encephalopathy, heat stroke, Creutzfeldt-Jakob disease.
Dysarthria Classification Summary
| Type | Tone | Speech Pattern | Key Causes |
|---|---|---|---|
| LMN/Neuromuscular | Flaccid | Nasal, slurred, weak consonants | ALS-bulbar, MG, GBS |
| Spastic (Pseudobulbar) | Spastic | Slow, strained, strangled | Bilateral stroke, MS, ALS |
| Rigid (Extrapyramidal) | Rigid | Rapid mumble, hypophonic, festinating | Parkinson's, PSP |
| Hyperkinetic | Variable | Explosive, irregular, "hiccup" | Huntington's, Tourette's |
| Ataxic (Cerebellar) | Hypotonic | Scanning, slurred, explosive | MS, cerebellar degeneration |
Aphasia vs. Dysarthria: Bedside Differentiation
| Feature | Aphasia | Dysarthria |
|---|---|---|
| Primary problem | Language formulation/comprehension | Muscle/motor control of articulation |
| Comprehension | Often impaired (type-dependent) | Intact |
| Writing | Impaired | Intact |
| Reading | Often impaired | Intact |
| Speech clarity | May be normal but incoherent | Slurred/distorted but content correct |
| Hemisphere | Left dominant | Bilateral, brainstem, or cerebellar |
Clinical Associations (Internal Medicine Perspective)
- Stroke (most common cause): Broca/Wernicke aphasia from MCA territory infarction; subcortical aphasia + dysarthria from lacunar strokes or basal ganglia/thalamic hemorrhage.
- TIA: Aphasia with dominant hemisphere involvement and dysarthria (not in isolation) are classic carotid TIA symptoms.
- Dementia: Anomic aphasia is the most common language disturbance in Alzheimer's disease.
- ALS: Combined spastic + flaccid (bulbar) dysarthria is pathognomonic.
- Myasthenia Gravis: Fatigable dysarthria + dysphonia + ptosis - characteristically worsening with sustained speech.
- Multiple Sclerosis: Ataxic or mixed dysarthria from cerebellar/corticobulbar plaques.
- Parkinson's Disease: Hypokinetic dysarthria (hypophonia, festination).
- Metabolic encephalopathy: Anomic aphasia is common.
Treatment
- Aphasia: Speech therapy to retrain contralateral/non-dominant hemisphere areas. If the lesion is limited, preserved language modalities (e.g., writing) can provide immediate communication channels.
- Dysarthria: Speech therapy focusing on slowing delivery and emphasizing key words. Augmentative communication devices for severe cases.
- Underlying cause: Treatment of the primary etiology (anticoagulation/thrombolysis for stroke, immunotherapy for MG, dopamine replacement for Parkinson's) is the most important intervention.
Sources:
- Bradley and Daroff's Neurology in Clinical Practice - Chapters 13 & 14
- Harrison's Principles of Internal Medicine 22E (2025) - Chapter 32
- Adams and Victor's Principles of Neurology, 12th Edition - Chapter 6
- Goldman-Cecil Medicine, International Edition
This is a shared conversation. Sign in to Orris to start your own chat.