Mujhe basic se advance tak chest xray samjhao jisse dekhte bata du kya hai
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Ab mere paas Harrison's aur Fishman's Pulmonary se bahut acchi information hai. Ab main ek comprehensive Hinglish guide likhta hoon.
Chest X-Ray - Basic se Advance tak Complete Guide
(Sources: Harrison's Principles of Internal Medicine 22E, Fishman's Pulmonary Diseases, Grainger & Allison's Diagnostic Radiology, Miller's Anesthesia)
Pehle ye samjho - X-Ray kaam kaise karta hai?
X-Ray mein tissues ki density ke hisaab se image banti hai:
- Kaala (Black/Lucent) = Air - jaise normal lungs, pneumothorax
- Safed (White/Opaque) = Dense tissue - jaise haddiyaan, fluid, pus, tumor
- Grey = In dono ke beech - muscles, heart
Yaad rakho: Jitna dense tissue, utna white. Jitna air, utna black.
STEP 1: Views - Kitne type ke CXR hote hain?
| View | Kab liya jaata hai | Khaasiyat |
|---|---|---|
| PA (Posteroanterior) | Outpatient, standing | Standard, best quality |
| AP (Anteroposterior) | Bedside/ICU patient | Heart thoda bada dikhta hai, quality thodi kam |
| Lateral | PA ke saath | Retrocardiac aur posterior areas better dikhte hain |
Tip: ICU mein AP portable film hoti hai - is mein cardiothoracic ratio reliable nahi hota kyunki heart magnify hota hai.
STEP 2: Systematic Approach - "ABCDE" Method
Chest X-Ray ko hamesha ek system se dekho, randomly nahi:
A - Airway
- Trachea midline mein hai ya nahi? (deviate hai toh kuch push/pull kar raha hai)
- Carina angle normal (<70 degrees) hai ya nahi?
- ETT/trach tube ka position check karo (ICU mein)
B - Bones & Soft Tissue
- Ribs fracture toh nahi? (dono sides count karo - 10 pairs dikhni chahiye)
- Clavicles, scapulae, humerus dekho
- Cervical spine dekho
- Soft tissue swelling ya subcutaneous emphysema toh nahi?
C - Cardiac
- Cardiothoracic (CT) ratio = Heart width / Chest width - Normal <0.5 (50%)
- Shape: Normal heart hourglass jaisi hoti hai
- Border clear hai ya blur?
- Right border = Right atrium
- Left border (upar) = Aortic knuckle + Pulmonary trunk
- Left border (neeche) = Left ventricle
D - Diaphragm
- Right dome thoda upar hoti hai left se (liver ki wajah se)
- Both costophrenic (CP) angles sharp hone chahiye
- Blunted CP angle = Pleural effusion
- Air under diaphragm = Bowel perforation!
E - Everything Else (Fields + Edges)
- Lung fields equally black hone chahiye
- Hilar shadows - normal density aur position
- Mediastinum width
- Pleural spaces
Yahan Normal CXR kaisi dikhti hai:
STEP 3: Common Pathologies - Pehchano kaise?
1. CONSOLIDATION (Pneumonia)
Kya hota hai: Lung ke alveoli mein air ki jagah fluid/pus aa jaata hai
CXR mein dikhega:
- White opacification - lobar ya segmental
- Air bronchogram sign - White opacity mein kaale airways dikhte hain (ye consolidation ka diagnostic sign hai)
- Margins lobe ki fissure se limited
Common cause: Pneumonia, pulmonary edema
2. PLEURAL EFFUSION
Kya hota hai: Pleural space mein fluid jam jaata hai
CXR mein dikhega:
- Blunted CP angle - pehla sign (>200-300 mL fluid chahiye)
- Meniscus sign - concave upper border
- Massive effusion mein: whole hemithorax white + trachea opposite side shift
- Supine film mein: diffuse haziness puri side mein
Tip: 200 mL se kam fluid PA film mein nahi dikhta - lateral decubitus view better hai
3. PNEUMOTHORAX
Kya hota hai: Pleural space mein air aa jaata hai
CXR mein dikhega:
- Lung edge (visceral pleural line) dikhti hai
- Uske bahar koi lung markings nahi
- Tension pneumothorax: Trachea opposite side shift + mediastinal shift (EMERGENCY!)
- Expiratory film mein better dikh sakta hai
4. CARDIOMEGALY (Enlarged Heart)
CT ratio >0.5 = Cardiomegaly
Specific enlargements:
- Left ventricular enlargement: Left lower border rounded + apex down aur out
- Left atrial enlargement: Double density sign, splaying of carina, displaced esophagus on lateral
- Right ventricular enlargement: Retrosternal space fill ho jaata hai on lateral view
- Pericardial effusion: Flask/globular shaped heart - "water bottle heart"
5. PULMONARY EDEMA (Congestive Heart Failure)
CXR mein dikhega (stages mein samjho):
| Stage | Finding |
|---|---|
| Early | Cephalization - upper lobe veins prominent (normally lower>upper) |
| Moderate | Kerley B lines - horizontal short white lines at lung bases/periphery (dilated lymphatics) |
| Severe | Bat-wing / butterfly opacity - bilateral perihilar haze |
| Very severe | Pleural effusion (usually bilateral, right > left) |
Bronchial cuffing bhi dikhta hai - bronchial walls thicken ho jaati hain edema se.
6. COLLAPSE / ATELECTASIS
Kya hota hai: Lung ka koi hissa deflate ho jaata hai
Direct signs:
- Increased opacity of that lobe
- Displaced fissures
Indirect signs:
- Trachea/mediastinum ipsilateral (same) side shift
- Elevated hemidiaphragm
- Compensatory hyperinflation of remaining lung
Lobar collapse patterns:
- Right upper lobe: Opacity right upper zone, trachea pulls to right
- Right middle lobe: Right heart border blur (silhouette sign)
- Right lower lobe: Triangular opacity behind heart on lateral
- Left lower lobe: Left heart border maintain (important!) - opacity behind heart
7. PNEUMONIA vs PULMONARY EDEMA - Kaise alag karein?
| Feature | Pneumonia | Pulmonary Edema |
|---|---|---|
| Distribution | Usually unilateral/lobar | Bilateral, symmetric |
| Kerley B lines | Nahi | Haan |
| Air bronchograms | Haan | Haan (dono mein) |
| Cardiomegaly | Usually nahi | Haan |
| CP angle | Normal (ya unilateral effusion) | Bilateral pleural effusion |
| Fever | Haan | Usually nahi |
8. INTERSTITIAL PATTERNS (Diffuse lung diseases)
Reticular pattern: Net/mesh jaisi lines - ILD, pulmonary fibrosis
Nodular pattern: Multiple small round opacities
- Fine nodules (miliary) = Miliary TB, miliary metastasis
- Coarse nodules = Metastasis, sarcoidosis
Reticulonodular: Combination - dono pattern saath
9. HILAR ABNORMALITIES
- Bilateral hilar enlargement: Sarcoidosis (classic), lymphoma, bilateral hilar adenopathy
- Unilateral hilar enlargement: Primary TB, malignancy, hilar node metastasis
- Pulmonary hypertension: Bilateral enlarged hila + peripheral "pruning" (vessels taper off)
10. MEDIASTINAL WIDENING
Normal mediastinum = <8 cm on PA view
Causes:
- Aortic dissection (EMERGENCY)
- Lymphoma / anterior mediastinal mass
- Thyroid goiter (superior mediastinum)
3T rule for anterior mediastinum masses:
- Thymoma (thymus)
- Teratoma (germ cell tumor)
- Terrible lymphoma
STEP 4: Silhouette Sign - Advance Concept
Rule: Jab do adjacent same-density structures ka border blur ho jaata hai toh unhe differentiate karna mushkil ho jaata hai.
- Right heart border blur = Right middle lobe consolidation/collapse
- Left heart border blur = Lingula (left upper lobe) pathology
- Diaphragm blur = Lower lobe pathology (adjacent to diaphragm)
- Aortic knuckle blur = Left upper lobe or adjacent pleural pathology
STEP 5: Ribs - Special Signs
- Rib notching = Coarctation of aorta (inferior rib margins mein erosion) - enlarged intercostal arteries pressure se
- Rib fractures = Multiple ke saath flail chest, pneumothorax
- "3" sign on CXR = Coarctation ka classic sign - aortic knuckle area mein figure-3 shape
STEP 6: Tubes aur Lines (ICU mein important)
| Device | Correct Position |
|---|---|
| ETT | 5 cm above carina, 2-3 cm below vocal cords |
| CVP catheter | SVC ya right atrium ka junction |
| Chest drain | Pleural space mein, tip apex ya base par (depend on indication) |
| NGT | Below diaphragm, tip stomach mein |
| IABP | Descending aorta, just distal to left subclavian |
Quick Reference Card - Kya Dikhega, Kya Sochna
| CXR Finding | Sabse Pehle Socho |
|---|---|
| Blunted CP angle | Pleural effusion |
| Hyperlucent lung + no markings | Pneumothorax |
| Bilateral perihilar haze + Kerley B | Pulmonary edema / CHF |
| Lobar consolidation + air bronchogram | Pneumonia |
| Air under diaphragm | Bowel perforation |
| Mediastinal widening | Aortic dissection / Lymphoma |
| Bilateral hilar adenopathy | Sarcoidosis |
| Rib notching | Coarctation of aorta |
| Miliary nodules | Miliary TB / Metastasis |
| Flask/water-bottle heart | Pericardial effusion |
Exam ke liye Golden Points
- Hamesha systematically dekho - ABCDE ya "Airway-Bones-Cardiac-Diaphragm-Lungs" order se
- PA vs AP pehle identify karo - AP mein CTR unreliable
- Silhouette sign use karo localization ke liye
- Trachea ko hamesha check karo - push ya pull indicate karta hai
- Both sides compare karo - asymmetry hi pathology hai aksar
- Clinical context hamesha saath rakho - same X-ray ka matlab alag patient mein alag ho sakta hai
Sources: Harrison's Principles of Internal Medicine 22E (2025), Fishman's Pulmonary Diseases & Disorders, Grainger & Allison's Diagnostic Radiology, Miller's Anesthesia 10e
Image ke explain
Asking for Preferences
Image ke sath explain karo table form me kardo jisse easily differenciate karde
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Ab poori visual comparison guide present karta hoon - image ke saath table form mein:
🫁 Chest X-Ray - Image ke Saath Complete Visual Guide
STEP 1 - Pehle Normal CXR Dekho (Reference)
Yahi tumhara baseline hai. Is normal X-ray mein kya dikhna chahiye:
| Structure | Normal Appearance |
|---|---|
| Lung fields | Dono sides equally kaala (air se bhari) |
| Heart (CTR) | Chest width ka <50% - right border = RA, left = LV |
| Trachea | Bilkul midline mein |
| Diaphragm | Right > Left (liver ki wajah se), sharp CP angles |
| Costophrenic (CP) angles | Pointed/sharp - blunt nahi |
| Hila | Symmetrical, moderate density |
PATHOLOGY COMPARISON - Image + Table
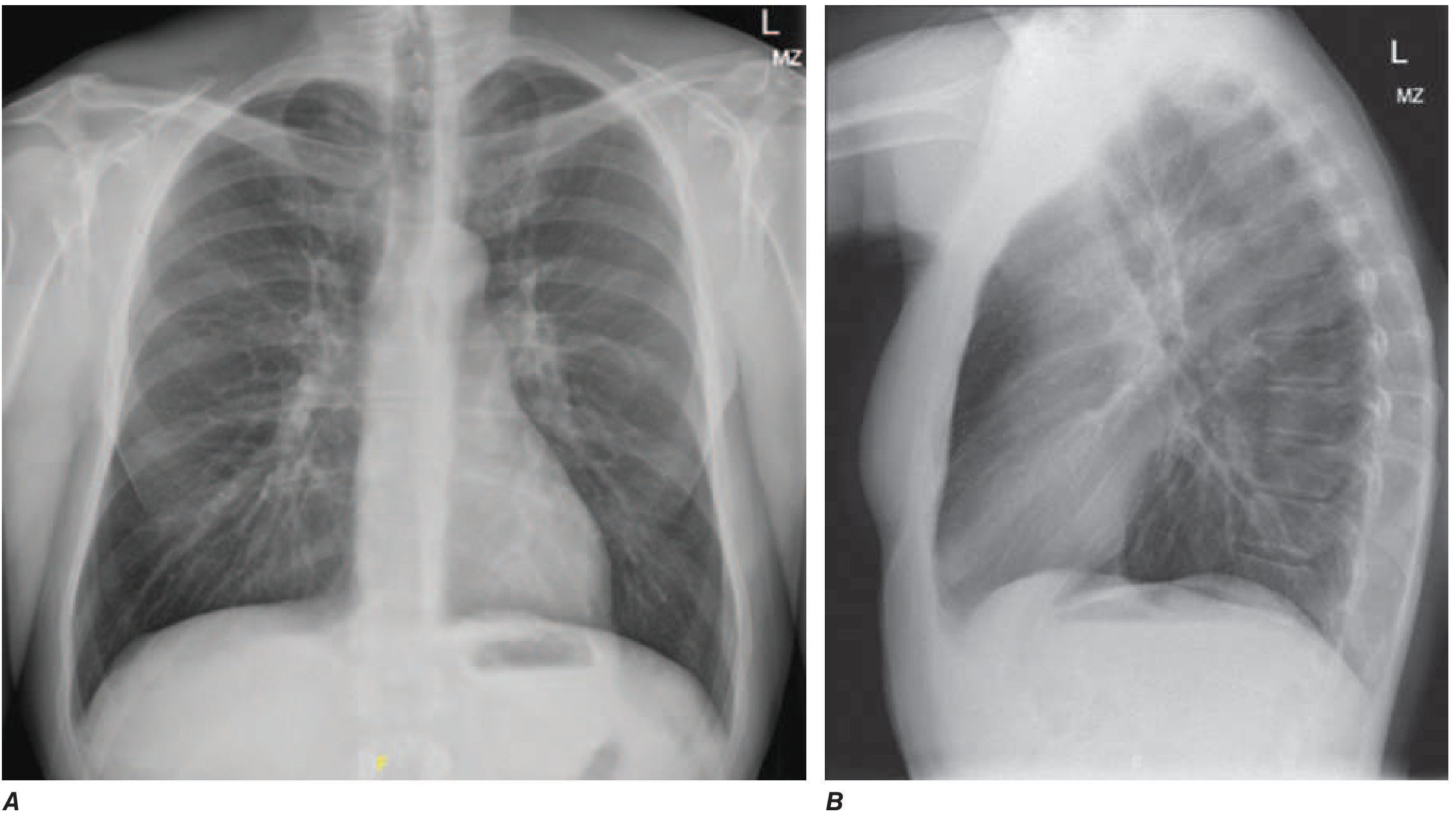
1. PNEUMOTHORAX

Dekho: Is X-ray mein nodular silicosis background ke saath right side pneumothorax hai - visceral pleural line clearly dikhti hai, uske bahar koi lung markings nahi hain
| Feature | Pneumothorax mein kya dikhega |
|---|---|
| Main sign | Visceral pleural line - ek thin white line, uske bahar koi lung markings nahi |
| Color | Affected side thodi zyada kaali (hyperlucent) |
| CP angle | Sharp rehta hai (pleural space mein air hai, fluid nahi) |
| Trachea | Small PTX mein midline; tension PTX mein opposite side shift |
| Diaphragm | Tension mein depress ho jaata hai |
| Erect vs Supine | Erect mein apex pe dikhta hai; supine mein "deep sulcus sign" |
| Cause | Trauma, tall young males (spontaneous), COPD bullae |
| Emergency sign | Trachea shift + depress diaphragm = TENSION - EMERGENCY! |
2. PLEURAL EFFUSION
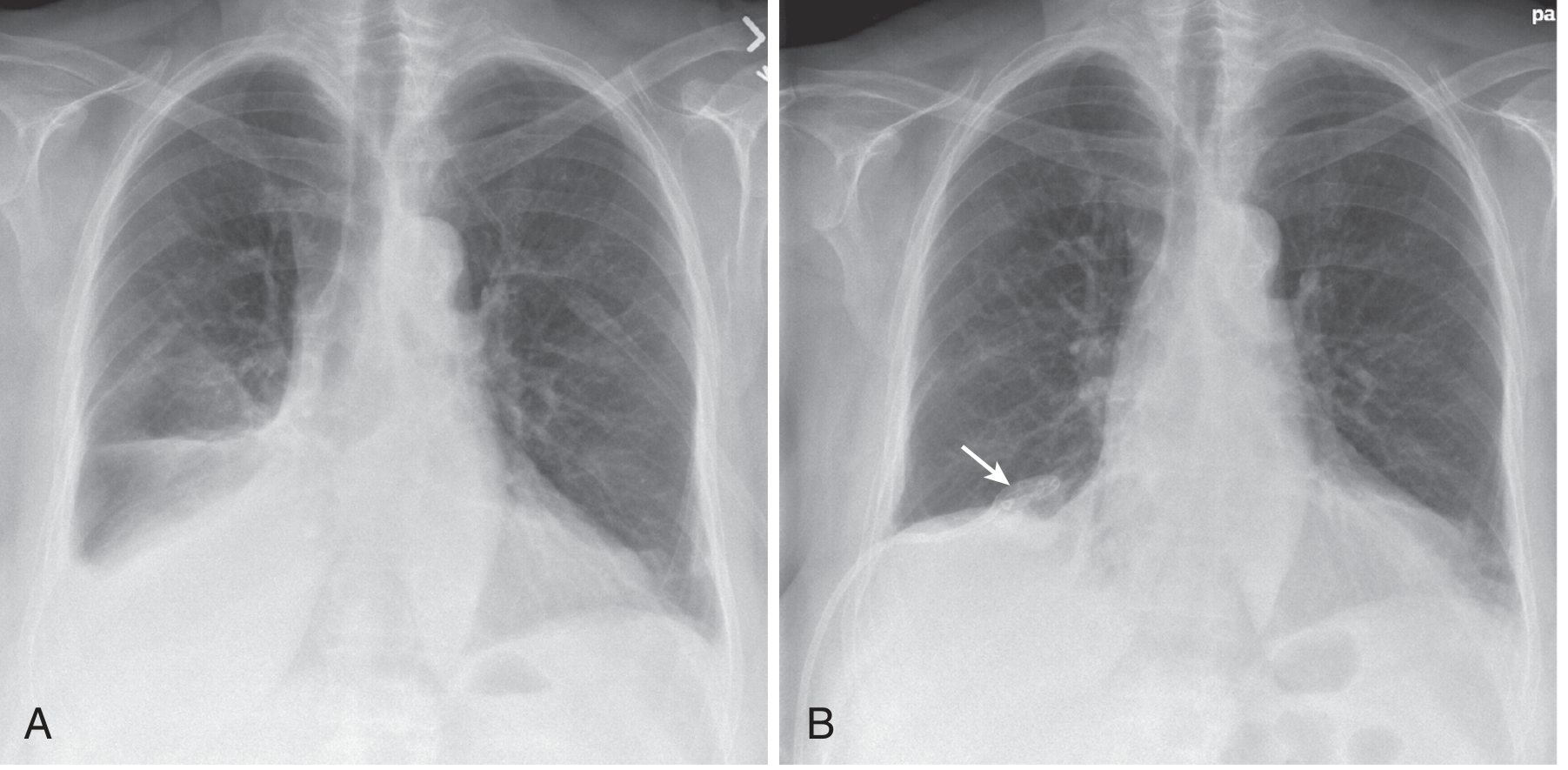
Dekho: Image A mein right side white opacity hai - CP angle blunt ho gaya, lower lobe ka outline blur. Image B mein pigtail catheter dala gaya drainage ke liye, lung reexpand ho gayi.
| Feature | Pleural Effusion mein kya dikhega |
|---|---|
| Main sign | Blunted CP angle - pehla aur sabse important sign |
| Color | Affected side white opacity - base mein zyada |
| Upper border | Meniscus sign - concave curve upar (hallmark!) |
| Trachea | Massive effusion mein opposite side shift |
| Amount | >200-300 mL hone par PA film mein dikhta hai |
| Supine film | Puri side mein diffuse haze - recognize karna mushkil |
| Alag kaise karein | Lateral decubitus mein fluid freely move karta hai |
| Common causes | CHF, TB, malignancy, parapneumonic, hypoalbuminemia |
3. PULMONARY EDEMA / CHF - Bat-Wing Pattern
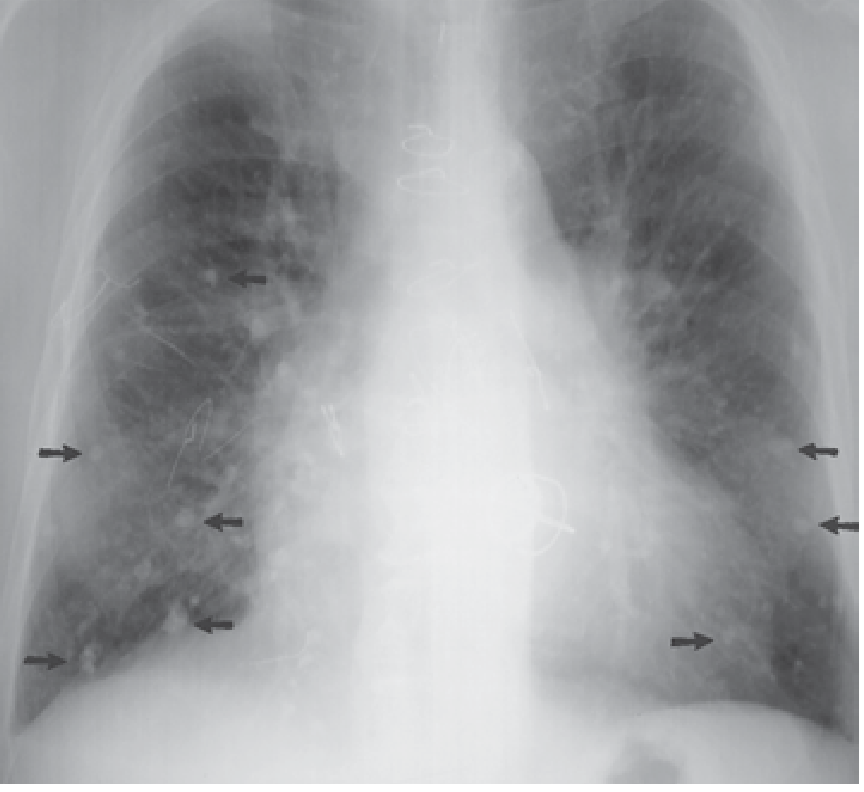
Dekho: Gross cardiomegaly hai. Arrows Kerley B lines point kar rahe hain (lung bases par). Right cardiac border par double density = dilated left atrium. Bilateral lower zone haze = interstitial edema.
| Feature | Pulmonary Edema mein kya dikhega |
|---|---|
| Cephalization | Upper lobe veins lower se zyada prominent (gravity reverse) |
| Kerley B lines | Lung base/periphery mein short horizontal white lines (dilated lymphatics) |
| Bat-wing/Butterfly | Bilateral perihilar white haze - severe case |
| Bronchial cuffing | Bronchi walls thicken dikhti hain |
| Heart size | Cardiomegaly (CTR >0.5) - usually present |
| Pleural effusion | Bilateral, right > left |
| Distribution | Bilateral, symmetric, perihilar |
| Air bronchograms | Ho sakte hain severe mein |
| Key differentiator | CHF = bilateral + cardiomegaly; Pneumonia = unilateral + fever |
4. CARDIOMEGALY + LEFT HEART FAILURE
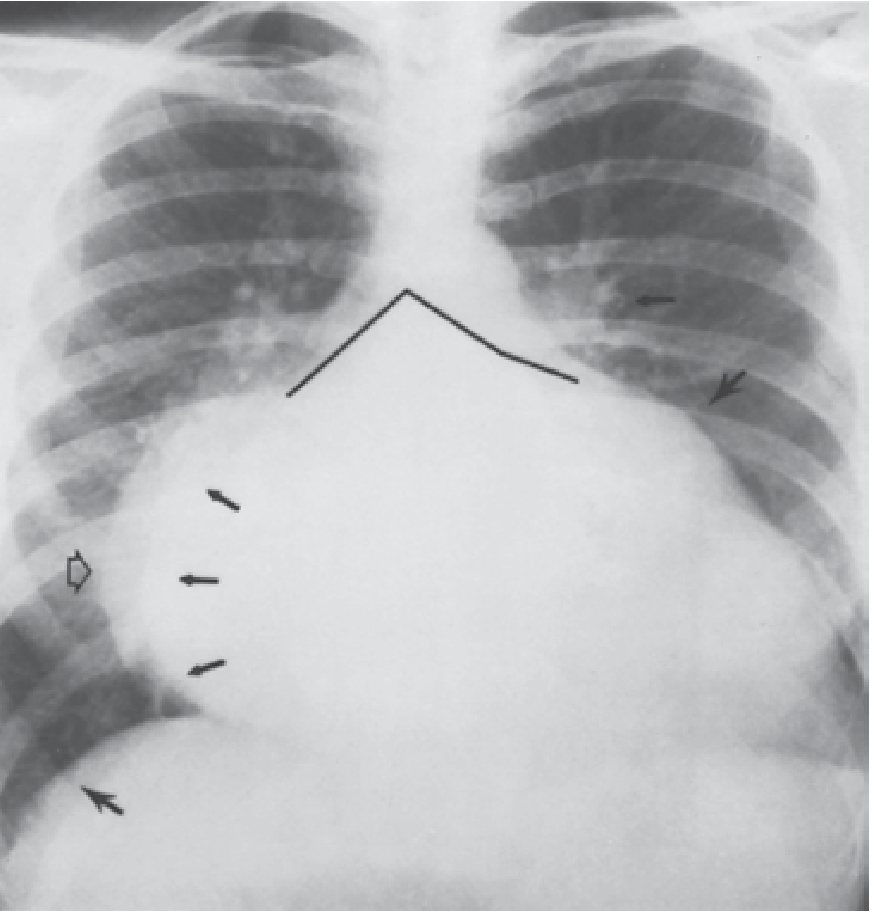
Dekho: Heart ka size massive hai - CTR clearly >0.5. Carina splayed (angles marked). Bilateral lower zone haze. Kerley B lines visible (small arrows). Left atrial appendage visible on left border (arrow).
| Cardiac Finding | CXR mein kya dikhega |
|---|---|
| Left ventricular enlargement | Left lower border rounded + apex down-and-out |
| Left atrial enlargement | Double density right border, carina splaying >70°, left atrial appendage prominent |
| Right ventricular enlargement | Lateral view mein retrosternal space fill |
| Pericardial effusion | Flask/water-bottle heart shape - all borders rounded globally |
| Aortic stenosis | Post-stenotic dilatation of ascending aorta - right upper border |
5. CAVITARY TUBERCULOSIS (TB)
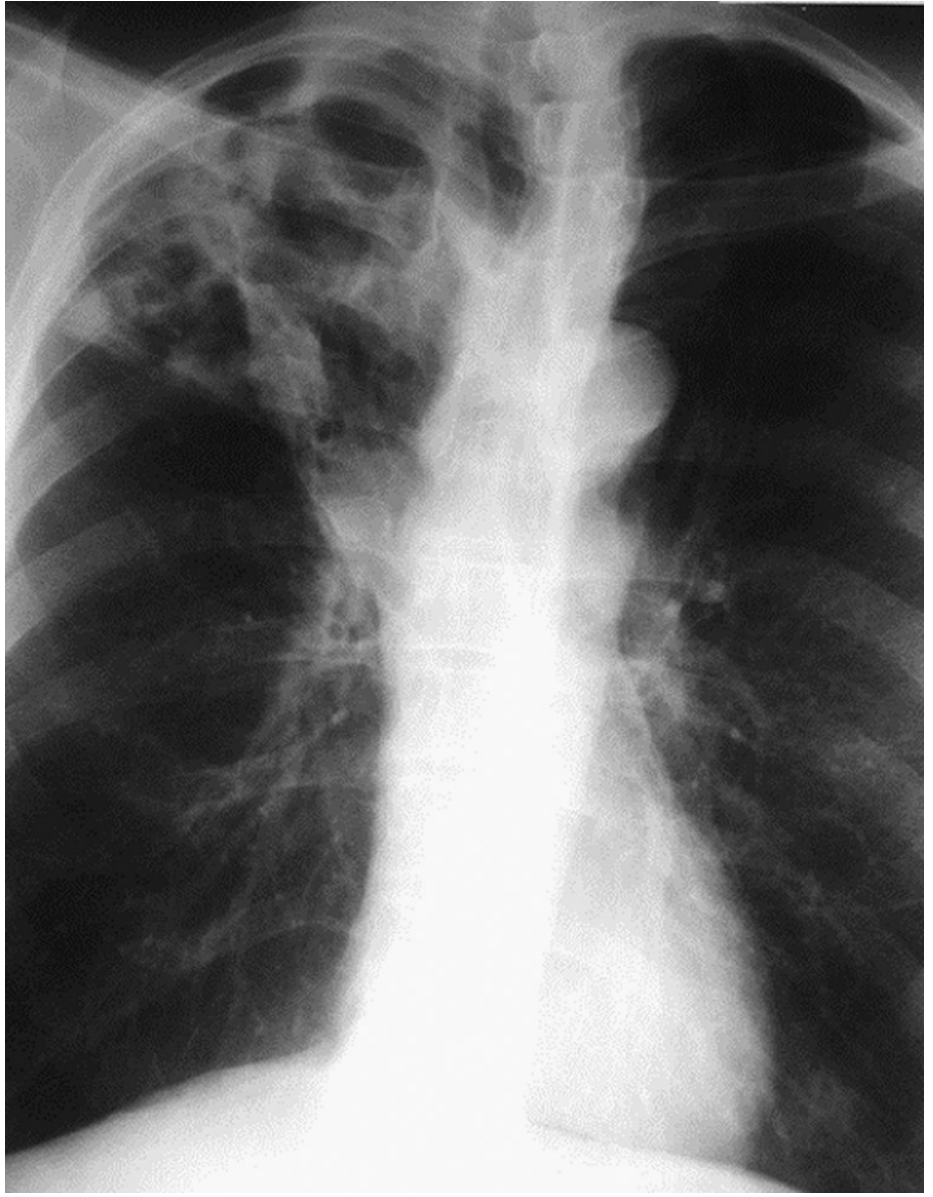
Dekho: Right upper lobe mein extensive cavitation hai - white opacity ke beech kaali cavity (air space). Upper lobe consolidation + cavity = TB until proven otherwise.
| Feature | TB mein kya dikhega |
|---|---|
| Location | Upper lobe predominant (right > left) + superior segment lower lobe |
| Primary TB | Lower/mid zone infiltrate + hilar adenopathy |
| Reactivation TB | Apical consolidation + cavity (hallmark) |
| Cavity | Thick-walled, irregular - kaali hole white opacity ke andar |
| Spread | Centrilobular nodules (bronchogenic spread) |
| Fibrosis/calcification | Old healed TB mein - white calcified foci + volume loss |
| Pleural effusion | TB pleuritis mein |
6. MILIARY TUBERCULOSIS

Dekho: Dono lungs mein bahut saare chote chote white dots - uniform size (1-3 mm), randomly distributed. Yahi miliary pattern hai. Millet seeds jaisi dikhti hai.
| Feature | Miliary Pattern mein kya dikhega |
|---|---|
| Size | 1-3 mm ke uniform small nodules |
| Distribution | Random, bilateral, uniform throughout both lungs |
| Borders | Well-defined, sharp edges |
| Density | Uniformly white dots |
| Look like | Millet seeds scattered - hence "miliary" |
| Common causes | Miliary TB (most common), miliary metastasis, histoplasmosis, sarcoidosis |
| Differentiating | TB = fever + weight loss + contact; Metastasis = known primary cancer |
7. TB WITH HIV - Bilateral Hilar Adenopathy
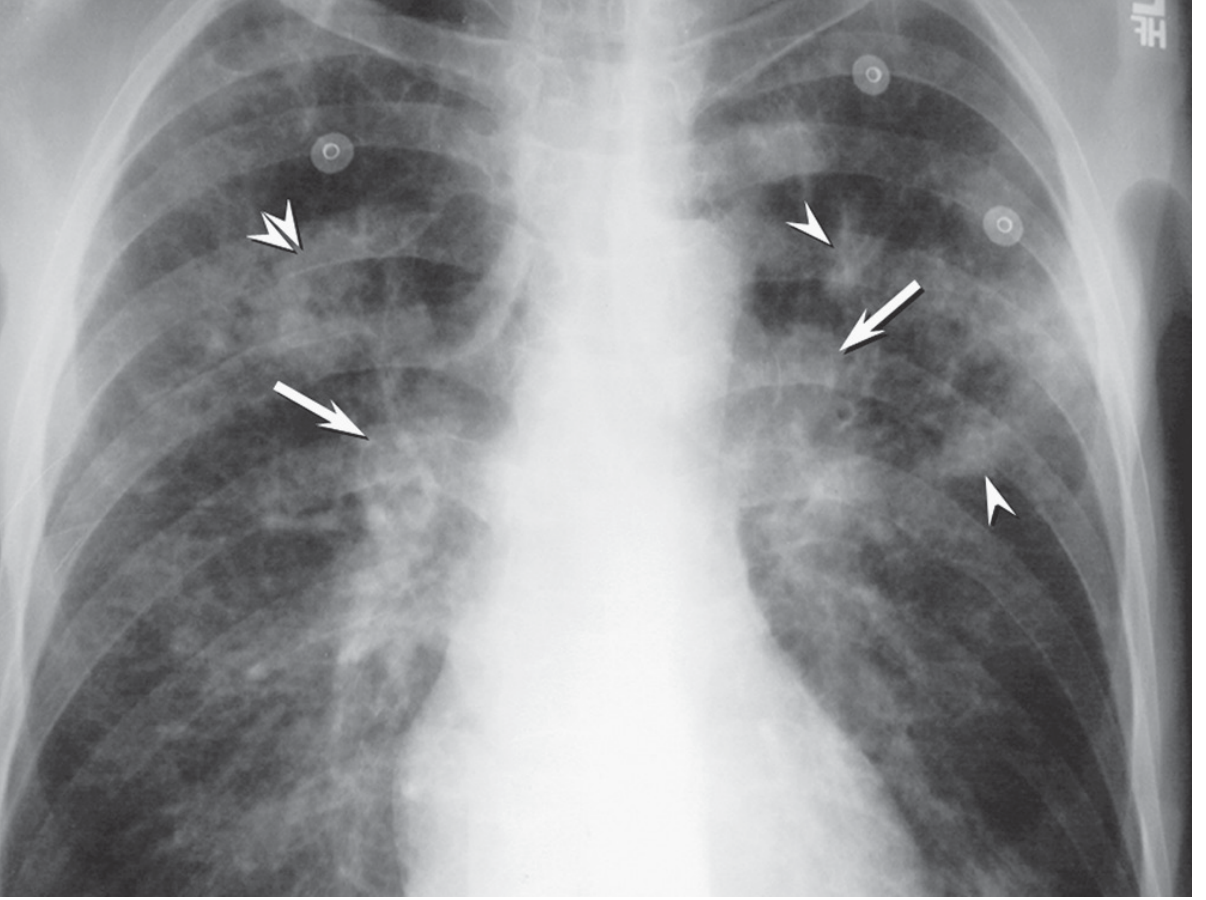
Dekho: Arrows bilateral hilar fullness dikhate hain (enlarged lymph nodes). Double arrowheads parenchymal consolidation. Arrowheads nodular opacities. HIV+ patient mein TB primary pattern show karta hai (lower zones bhi involved).
| Feature | Hilar Adenopathy mein kya dikhega |
|---|---|
| Bilateral hilar enlargement | Hila "lobular" ya potato-like dikhta hai |
| Unilateral | TB (primary), malignancy, lymphoma |
| Bilateral | Sarcoidosis (classic), lymphoma, TB+HIV |
| Eggshell calcification | Sarcoidosis ya silicosis mein hilar nodes |
| "1-2-3 sign" | Sarcoidosis - right paratracheal + bilateral hila = 3 humps |
8. PNEUMOTHORAX DRAINAGE (Before & After)
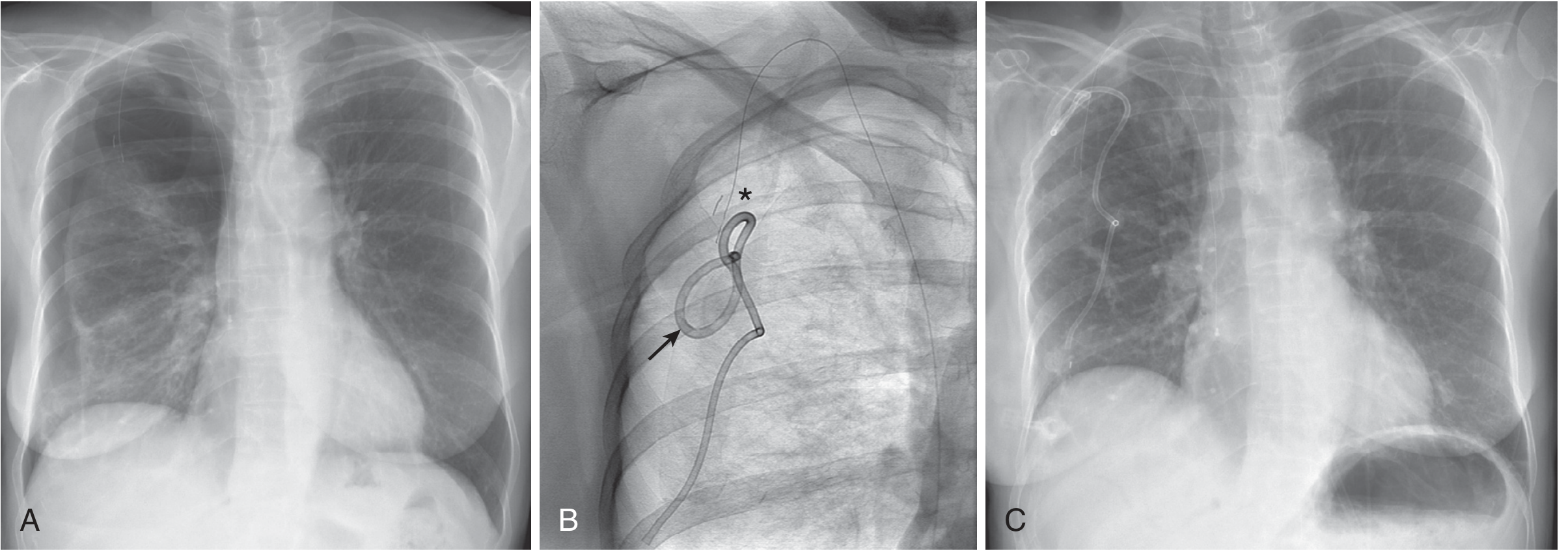
Dekho: Image A - large right pneumothorax (right side kaali, lung collapsed). Image B - 2nd anterior intercostal space se catheter dala. Image C - complete re-expansion, lung wapas normal.
MASTER COMPARISON TABLE - Sabse Important
| Condition | Color/Opacity | Location | Trachea | CP Angle | Heart | Key Sign |
|---|---|---|---|---|---|---|
| Normal | Black lungs | Bilateral equal | Midline | Sharp | <50% CTR | - |
| Pneumothorax | Hyperlucent (extra black) | Apex/unilateral | Midline (tension = shift away) | Sharp | Normal | Visceral pleural line, no lung markings beyond |
| Pleural Effusion | White base | Unilateral or bilateral base | Massive = shift away | Blunted | Normal or enlarged | Meniscus sign |
| Pneumonia | White patch | Lobar/segmental | Normal | Normal | Normal | Air bronchogram |
| Pulmonary Edema | Bilateral haze | Perihilar (bat-wing) | Normal | Blunted (bilateral effusion) | Enlarged | Kerley B lines + cephalization |
| Collapse/Atelectasis | White | Affected lobe | Ipsilateral shift (pulled) | Elevated diaphragm | Normal | Volume loss signs |
| Miliary TB | Tiny white dots | Bilateral, random | Normal | Normal | Normal | 1-3mm uniform nodules |
| Cavitary TB | White + black hole | Upper lobe | Normal | Normal | Normal | Thick-walled cavity |
| Cardiomegaly | Normal lungs | - | Normal | Normal | >50% CTR | Rounded heart borders |
| Pericardial effusion | Normal lungs | - | Normal | Normal | Flask shape | Globally enlarged all borders |
Trachea Rule - Quick Memory
Trachea shift AWAY from opacity = SPACE-OCCUPYING (Effusion, Tumor, Tension PTX)
Trachea shift TOWARD opacity = VOLUME-LOSING (Collapse, Fibrosis, Lobectomy)
Color Cheatsheet
| Color on CXR | Matlab |
|---|---|
| Jet black | Air (Pneumothorax) |
| Dark grey/black | Normal aerated lung |
| White (dense) | Fluid, pus, blood, tumor, bone |
| Grey (intermediate) | Soft tissue, heart, muscles |
| Very white | Bone (ribs, sternum) |
| Black ring in white | Cavity (TB, abscess, cancer) |
Sources: Fishman's Pulmonary Diseases, Fuster & Hurst's The Heart 15th Ed, Murray & Nadel's Respiratory Medicine, Grainger & Allison's Diagnostic Radiology, Harrison's Internal Medicine 22E (2025)
Create a PDF quick reference card with these images for offline study
Reading File
Running Command
mkdir -p /home/daytona/workspace/cxr-reference-card/images && ls /home/daytona/w…
Running Command
cd /home/daytona/workspace/cxr-reference-card/images && \ curl -s -o normal_cxr.…
Writing File
~/cxr-reference-card/generate_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import cm, mm
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Image, Table, TableStyle,
PageBreak, HRFlowable, KeepTogether
)
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.pdfgen import canvas
from reportlab.platypus.flowables import Flowable
import os
IMG_DIR = "/home/daytona/workspace/cxr-reference-card/images"
OUT_PATH = "/home/daytona/workspace/cxr-reference-card/CXR_Quick_Reference.pdf"
# ── Colors ──────────────────────────────────────────────────────────────────
DARK_BLUE = colors.HexColor("#1A3A5C")
MED_BLUE = colors.HexColor("#2E6DA4")
LIGHT_BLUE = colors.HexColor("#D6E8F7")
ACCENT_RED = colors.HexColor("#C0392B")
ACCENT_GRN = colors.HexColor("#1A7A4A")
YELLOW_HL = colors.HexColor("#FFF3CD")
WHITE = colors.white
LIGHT_GREY = colors.HexColor("#F5F5F5")
MID_GREY = colors.HexColor("#CCCCCC")
DARK_GREY = colors.HexColor("#444444")
BLACK = colors.black
PAGE_W, PAGE_H = A4
MARGIN = 1.5 * cm
# ── Styles ───────────────────────────────────────────────────────────────────
styles = getSampleStyleSheet()
title_style = ParagraphStyle(
"MainTitle",
fontSize=22, fontName="Helvetica-Bold",
textColor=WHITE, alignment=TA_CENTER,
spaceAfter=4, leading=28
)
subtitle_style = ParagraphStyle(
"SubTitle",
fontSize=11, fontName="Helvetica",
textColor=LIGHT_BLUE, alignment=TA_CENTER,
spaceAfter=2
)
section_head = ParagraphStyle(
"SectionHead",
fontSize=13, fontName="Helvetica-Bold",
textColor=WHITE, alignment=TA_LEFT,
leftIndent=6, spaceAfter=0, leading=18
)
card_title = ParagraphStyle(
"CardTitle",
fontSize=11, fontName="Helvetica-Bold",
textColor=DARK_BLUE, spaceAfter=3, leading=14
)
body_style = ParagraphStyle(
"Body",
fontSize=8.5, fontName="Helvetica",
textColor=DARK_GREY, leading=12, spaceAfter=2
)
caption_style = ParagraphStyle(
"Caption",
fontSize=7.5, fontName="Helvetica-Oblique",
textColor=colors.HexColor("#666666"),
alignment=TA_CENTER, spaceAfter=4, leading=10
)
table_header_style = ParagraphStyle(
"TblHdr",
fontSize=8, fontName="Helvetica-Bold",
textColor=WHITE, alignment=TA_CENTER, leading=10
)
table_cell_style = ParagraphStyle(
"TblCell",
fontSize=7.5, fontName="Helvetica",
textColor=DARK_GREY, leading=10, alignment=TA_LEFT
)
emergency_style = ParagraphStyle(
"Emergency",
fontSize=8.5, fontName="Helvetica-Bold",
textColor=ACCENT_RED, leading=11
)
tip_style = ParagraphStyle(
"Tip",
fontSize=8, fontName="Helvetica",
textColor=colors.HexColor("#7B4F00"), leading=11
)
# ── Header / Footer canvas ───────────────────────────────────────────────────
def add_page_deco(canvas_obj, doc):
canvas_obj.saveState()
# Footer
canvas_obj.setFillColor(DARK_BLUE)
canvas_obj.rect(0, 0, PAGE_W, 1.0*cm, fill=1, stroke=0)
canvas_obj.setFillColor(WHITE)
canvas_obj.setFont("Helvetica", 7)
canvas_obj.drawCentredString(
PAGE_W/2, 0.35*cm,
"Sources: Harrison's IM 22E | Fishman's Pulmonary | Murray & Nadel | Grainger & Allison | Fuster & Hurst's Heart 15E"
)
canvas_obj.drawRightString(PAGE_W - MARGIN, 0.35*cm, f"Page {doc.page}")
canvas_obj.restoreState()
# ── Helper: coloured section banner ─────────────────────────────────────────
def section_banner(text, color=DARK_BLUE):
data = [[Paragraph(text, section_head)]]
t = Table(data, colWidths=[PAGE_W - 2*MARGIN])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), color),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 8),
("ROUNDEDCORNERS", [4]),
]))
return t
# ── Helper: image with caption ───────────────────────────────────────────────
def img_with_caption(fname, caption, width=7.5*cm):
path = os.path.join(IMG_DIR, fname)
if not os.path.exists(path):
return Paragraph(f"[Image not found: {fname}]", body_style)
try:
img = Image(path, width=width, height=width*0.72, kind="proportional")
cap = Paragraph(caption, caption_style)
data = [[img], [cap]]
t = Table(data, colWidths=[width + 0.4*cm])
t.setStyle(TableStyle([
("ALIGN", (0,0), (-1,-1), "CENTER"),
("BACKGROUND", (0,0), (0,0), colors.HexColor("#1A1A1A")),
("BACKGROUND", (0,1), (0,1), LIGHT_GREY),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 3),
("RIGHTPADDING", (0,0), (-1,-1), 3),
("BOX", (0,0), (-1,-1), 1, MID_GREY),
]))
return t
except Exception as e:
return Paragraph(f"[Error loading {fname}: {e}]", body_style)
# ── Helper: pathology table ───────────────────────────────────────────────────
def make_table(headers, rows, col_widths, header_color=MED_BLUE):
hdr = [Paragraph(h, table_header_style) for h in headers]
data = [hdr]
for row in rows:
data.append([Paragraph(str(c), table_cell_style) for c in row])
t = Table(data, colWidths=col_widths, repeatRows=1)
style = [
("BACKGROUND", (0,0), (-1,0), header_color),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("ALIGN", (0,0), (-1,-1), "LEFT"),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,-1), 7.5),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING", (0,0), (-1,-1), 3),
("LEFTPADDING", (0,0), (-1,-1), 5),
("GRID", (0,0), (-1,-1), 0.4, MID_GREY),
("ROWBACKGROUNDS", (0,1), (-1,-1), [WHITE, LIGHT_GREY]),
("VALIGN", (0,0), (-1,-1), "TOP"),
]
t.setStyle(TableStyle(style))
return t
# ── Build content ─────────────────────────────────────────────────────────────
def build_pdf():
doc = SimpleDocTemplate(
OUT_PATH,
pagesize=A4,
rightMargin=MARGIN, leftMargin=MARGIN,
topMargin=MARGIN, bottomMargin=1.6*cm,
title="Chest X-Ray Quick Reference Card",
author="Orris Medical Library"
)
story = []
CW = PAGE_W - 2*MARGIN # content width
# ═══════════════════════════════════════════════════════
# PAGE 1 – COVER + NORMAL CXR + BASICS
# ═══════════════════════════════════════════════════════
# Cover banner
cover_data = [[
Paragraph("🫁 CHEST X-RAY", title_style),
Paragraph("Quick Reference Card", subtitle_style),
Paragraph("Basic se Advance – Visual Guide", subtitle_style),
]]
cover = Table([[
Paragraph("🫁 CHEST X-RAY", title_style)],
[Paragraph("Quick Reference Card | Basic se Advance – Visual Guide", subtitle_style)
]], colWidths=[CW])
cover.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), DARK_BLUE),
("TOPPADDING", (0,0), (-1,-1), 12),
("BOTTOMPADDING", (0,0), (-1,-1), 12),
("LEFTPADDING", (0,0), (-1,-1), 10),
("ROUNDEDCORNERS", [6]),
]))
story.append(cover)
story.append(Spacer(1, 0.4*cm))
# X-Ray Density cheatsheet
story.append(section_banner("X-Ray Density – Kya Color Kya Matlab?", MED_BLUE))
story.append(Spacer(1, 0.2*cm))
density_rows = [
["Jet Black", "Air / Pneumothorax (most lucent)"],
["Dark Grey/Black", "Normal aerated lung"],
["Grey", "Soft tissue – heart, muscles, liver"],
["White (opaque)", "Fluid, pus, blood, tumor, collapse"],
["Bright White", "Bone – ribs, sternum, clavicles"],
["Black hole in White", "Cavity – TB abscess, lung cancer"],
]
story.append(make_table(
["Color on X-Ray", "Matlab (Meaning)"],
density_rows,
[5.5*cm, CW - 5.5*cm - 0.1*cm],
header_color=MED_BLUE
))
story.append(Spacer(1, 0.35*cm))
# Normal CXR + Normal anatomy table side by side
story.append(section_banner("NORMAL CHEST X-RAY – Baseline", ACCENT_GRN))
story.append(Spacer(1, 0.25*cm))
normal_img = img_with_caption(
"normal_cxr.png",
"Normal PA (left) + Lateral (right) CXR\n(Harrison's IM 22E)",
width=9.5*cm
)
normal_tbl = make_table(
["Structure", "Normal Finding"],
[
["Trachea", "Midline, visible above carina"],
["Carina angle", "<70° (LA enlargement mein splayed)"],
["Lung fields", "Bilateral equal black (aerated)"],
["Heart (CTR)", "<0.5 (50%) on PA erect film"],
["Right border", "Right atrium (RA)"],
["Left border (up)","Aortic knuckle + Pulm trunk"],
["Left border (dn)","Left ventricle (LV)"],
["Diaphragm", "Right > Left (liver neeche)"],
["CP angles", "Sharp, pointed – blunt = effusion"],
["Hila", "Symmetric, left slightly higher"],
],
[3.2*cm, CW - 9.8*cm - 0.2*cm],
header_color=ACCENT_GRN
)
row = Table(
[[normal_img, normal_tbl]],
colWidths=[9.8*cm, CW - 9.8*cm]
)
row.setStyle(TableStyle([
("VALIGN", (0,0), (-1,-1), "TOP"),
("LEFTPADDING", (0,0), (-1,-1), 0),
("RIGHTPADDING", (0,0), (-1,-1), 4),
]))
story.append(row)
story.append(Spacer(1, 0.35*cm))
# ABCDE systematic approach
story.append(section_banner("SYSTEMATIC APPROACH – ABCDE Method", DARK_BLUE))
story.append(Spacer(1, 0.2*cm))
abcde_rows = [
["A – Airway", "Trachea midline? ETT position? Carina angle?"],
["B – Bones", "Rib fractures? Clavicles? Scapulae? Soft tissue?"],
["C – Cardiac", "CTR <0.5? Heart shape? Borders clear?"],
["D – Diaphragm", "Right > Left? CP angles sharp? Air under = perforation!"],
["E – Everything", "Lung fields? Hila? Mediastinum? Pleural space? Tubes/lines?"],
]
story.append(make_table(
["Step", "Check Karo"],
abcde_rows,
[3.2*cm, CW - 3.2*cm - 0.1*cm],
header_color=DARK_BLUE
))
story.append(PageBreak())
# ═══════════════════════════════════════════════════════
# PAGE 2 – PNEUMOTHORAX + PLEURAL EFFUSION
# ═══════════════════════════════════════════════════════
story.append(section_banner("1. PNEUMOTHORAX", DARK_BLUE))
story.append(Spacer(1, 0.25*cm))
ptx_img = img_with_caption(
"pneumothorax.png",
"Spontaneous PTX – visceral pleural\nline clearly visible (Fishman's Pulmonary)",
width=8.5*cm
)
ptx_tbl = make_table(
["Feature", "Finding"],
[
["Main sign", "Visceral pleural line – thin white line, NO lung markings beyond"],
["Color", "Hyperlucent (extra black) on affected side"],
["CP angle", "Sharp (air, not fluid)"],
["Trachea", "Midline in simple; OPPOSITE shift in Tension PTX"],
["Diaphragm", "Depressed in Tension PTX"],
["Erect film", "Air at APEX (best seen)"],
["Supine film", "\"Deep sulcus sign\" – very deep lateral CP angle"],
["Causes", "Trauma, tall young males (spontaneous), COPD bullae"],
],
[2.8*cm, CW - 8.8*cm - 0.2*cm],
header_color=DARK_BLUE
)
ptx_row = Table([[ptx_img, ptx_tbl]], colWidths=[8.8*cm, CW - 8.8*cm])
ptx_row.setStyle(TableStyle([("VALIGN",(0,0),(-1,-1),"TOP"),("LEFTPADDING",(0,0),(-1,-1),0),("RIGHTPADDING",(0,0),(-1,-1),4)]))
story.append(ptx_row)
story.append(Spacer(1, 0.15*cm))
story.append(Table([[Paragraph(
"⚠ TENSION PNEUMOTHORAX EMERGENCY: Trachea shifts AWAY + depressed diaphragm + hemodynamic collapse → immediate needle decompression!",
emergency_style
)]], colWidths=[CW], style=[
("BACKGROUND",(0,0),(-1,-1),colors.HexColor("#FDECEA")),
("BOX",(0,0),(-1,-1),1,ACCENT_RED),
("TOPPADDING",(0,0),(-1,-1),5),("BOTTOMPADDING",(0,0),(-1,-1),5),
("LEFTPADDING",(0,0),(-1,-1),8),
]))
story.append(Spacer(1, 0.4*cm))
# Pleural effusion
story.append(section_banner("2. PLEURAL EFFUSION", MED_BLUE))
story.append(Spacer(1, 0.25*cm))
eff_img = img_with_caption(
"pleural_effusion.png",
"Right pleural effusion (A) → after\ndrainage catheter placement (B)\n(Murray & Nadel's Respiratory Medicine)",
width=9*cm
)
eff_tbl = make_table(
["Feature", "Finding"],
[
["Main sign", "BLUNTED CP angle – pehla aur sabse important sign"],
["Shape", "Meniscus sign – concave upper border (hallmark)"],
["Color", "White opacity at base, affected side"],
["Trachea", "Massive effusion mein OPPOSITE side shift"],
["Threshold", ">200-300 mL PA film mein dikh ta hai"],
["Supine film", "Diffuse haze entire side – diagnose karna mushkil"],
["Lat decubitus","Freely mobile fluid = effusion confirmed"],
["Causes", "CHF, TB, malignancy, parapneumonic, hypoalbuminemia"],
],
[2.8*cm, CW - 9.3*cm - 0.2*cm],
header_color=MED_BLUE
)
eff_row = Table([[eff_img, eff_tbl]], colWidths=[9.3*cm, CW - 9.3*cm])
eff_row.setStyle(TableStyle([("VALIGN",(0,0),(-1,-1),"TOP"),("LEFTPADDING",(0,0),(-1,-1),0),("RIGHTPADDING",(0,0),(-1,-1),4)]))
story.append(eff_row)
story.append(PageBreak())
# ═══════════════════════════════════════════════════════
# PAGE 3 – PULMONARY EDEMA + CARDIOMEGALY
# ═══════════════════════════════════════════════════════
story.append(section_banner("3. PULMONARY EDEMA / CHF", MED_BLUE))
story.append(Spacer(1, 0.25*cm))
ped_img = img_with_caption(
"pulm_edema_kerleyb.png",
"CHF – Kerley B lines (arrows at periphery),\ncardiomegaly, bilateral lower zone haze\n(Fuster & Hurst's Heart 15E)",
width=7.5*cm
)
ped_tbl = make_table(
["Stage/Sign", "CXR Finding"],
[
["Cephalization", "Upper lobe veins MORE prominent than lower (gravity reversed)"],
["Kerley B lines", "Short horizontal white lines at lung BASE/periphery (dilated lymphatics) ★"],
["Bat-wing/Butterfly","Bilateral PERIHILAR white haze – severe edema"],
["Bronchial cuffing","Bronchial walls appear THICKENED (peribronchial edema)"],
["Heart size", "Cardiomegaly – CTR >0.5"],
["Pleural effusion", "Bilateral, RIGHT > LEFT"],
["Distribution", "Bilateral, symmetric, perihilar"],
["vs Pneumonia", "CHF = bilateral + cardiomegaly; Pneumonia = unilateral + fever"],
],
[3.5*cm, CW - 7.8*cm - 0.2*cm],
header_color=MED_BLUE
)
ped_row = Table([[ped_img, ped_tbl]], colWidths=[7.8*cm, CW - 7.8*cm])
ped_row.setStyle(TableStyle([("VALIGN",(0,0),(-1,-1),"TOP"),("LEFTPADDING",(0,0),(-1,-1),0),("RIGHTPADDING",(0,0),(-1,-1),4)]))
story.append(ped_row)
story.append(Spacer(1, 0.4*cm))
story.append(section_banner("4. CARDIOMEGALY & CARDIAC ENLARGEMENT", colors.HexColor("#6B2D8B")))
story.append(Spacer(1, 0.25*cm))
card_img = img_with_caption(
"cardiomegaly_chf.png",
"Gross cardiomegaly – mitral & tricuspid\nregurgitation. Carina splayed (lines).\nKerley B lines (arrows). LA = double density.\n(Fuster & Hurst's Heart 15E)",
width=7.5*cm
)
card_tbl = make_table(
["Chamber/Condition", "CXR Sign"],
[
["CTR >0.5", "CARDIOMEGALY (PA erect film mein measure karo)"],
["Left Ventricle ↑", "Left lower border ROUNDED, apex down-and-out"],
["Left Atrium ↑", "Double density right border, carina splaying >70°, LA appendage"],
["Right Ventricle ↑", "Lateral view: retrosternal space fill ho jaata hai"],
["Pericardial effusion", "FLASK / WATER-BOTTLE heart – all borders globally rounded"],
["Aortic stenosis", "Post-stenotic dilatation – ascending aorta right upper border"],
["Pulmonary hypertension", "Bilateral enlarged hila + peripheral pruning"],
],
[4.5*cm, CW - 7.8*cm - 0.2*cm],
header_color=colors.HexColor("#6B2D8B")
)
card_row = Table([[card_img, card_tbl]], colWidths=[7.8*cm, CW - 7.8*cm])
card_row.setStyle(TableStyle([("VALIGN",(0,0),(-1,-1),"TOP"),("LEFTPADDING",(0,0),(-1,-1),0),("RIGHTPADDING",(0,0),(-1,-1),4)]))
story.append(card_row)
story.append(PageBreak())
# ═══════════════════════════════════════════════════════
# PAGE 4 – TUBERCULOSIS (Cavitary + Miliary + HIV)
# ═══════════════════════════════════════════════════════
story.append(section_banner("5. CAVITARY TUBERCULOSIS", ACCENT_RED))
story.append(Spacer(1, 0.25*cm))
ctb_img = img_with_caption(
"cavitary_tb.png",
"Cavitary TB – extensive right upper\nlobe cavitation (Fishman's Pulmonary)",
width=7.2*cm
)
ctb_tbl = make_table(
["Feature", "Finding"],
[
["Location", "UPPER LOBE dominant (right > left) + superior segment lower lobe"],
["Primary TB", "Lower/mid zone infiltrate + hilar adenopathy + pleural effusion"],
["Reactivation TB", "APICAL CONSOLIDATION + CAVITY (hallmark) ★"],
["Cavity appearance", "Thick-walled, irregular – kaali hole white opacity ke andar"],
["Bronchogenic spread","Centrilobular nodules – tree-in-bud pattern"],
["Healed TB", "Calcified foci + volume loss + fibrosis upper lobes"],
["Pleural effusion", "TB pleuritis mein – lymphocyte exudate"],
],
[3.5*cm, CW - 7.5*cm - 0.2*cm],
header_color=ACCENT_RED
)
ctb_row = Table([[ctb_img, ctb_tbl]], colWidths=[7.5*cm, CW - 7.5*cm])
ctb_row.setStyle(TableStyle([("VALIGN",(0,0),(-1,-1),"TOP"),("LEFTPADDING",(0,0),(-1,-1),0),("RIGHTPADDING",(0,0),(-1,-1),4)]))
story.append(ctb_row)
story.append(Spacer(1, 0.4*cm))
# Miliary TB + TB-HIV side by side
story.append(section_banner("6. MILIARY TB & 7. TB with HIV – Hilar Adenopathy", colors.HexColor("#C0711A")))
story.append(Spacer(1, 0.25*cm))
mil_img = img_with_caption(
"miliary_tb.png",
"Miliary TB – 1-3 mm random\nbilateral nodules (Murray & Nadel)",
width=7*cm
)
hiv_img = img_with_caption(
"tb_hiv_hilar.png",
"TB + HIV – bilateral hilar adenopathy\n(arrows) + parenchymal nodules\n(Murray & Nadel)",
width=7*cm
)
mil_tbl = make_table(
["Feature", "Finding"],
[
["Size", "1-3 mm uniform nodules"],
["Distribution", "Random, bilateral, uniform"],
["Pattern", "Millet seeds – fine stippling"],
["Cause", "TB (most common), metastasis,\nhistoplasmosis, sarcoidosis"],
],
[2.8*cm, 3.8*cm],
header_color=colors.HexColor("#C0711A")
)
hiv_tbl = make_table(
["Feature", "Finding"],
[
["Hilar", "Bilateral enlarged, lobular"],
["Pattern", "Lower zone infiltrates (atypical)"],
["Sarcoidosis", "\"1-2-3 sign\" bilateral hilar adenopathy"],
["Eggshell calc","Sarcoidosis / silicosis nodes"],
],
[2.8*cm, 3.8*cm],
header_color=colors.HexColor("#C0711A")
)
dual = Table([
[mil_img, Spacer(0.2*cm,1), mil_tbl, Spacer(0.4*cm,1), hiv_img, Spacer(0.2*cm,1), hiv_tbl]
], colWidths=[7.2*cm, 0.2*cm, 6.8*cm, 0.4*cm, 7.2*cm, 0.2*cm, 6.8*cm])
# recalculate – total CW=17cm approx, split each pair
# simpler 4-col
dual2 = Table([
[mil_img, mil_tbl, hiv_img, hiv_tbl]
], colWidths=[7.2*cm, 6.8*cm - 0.2*cm, 7.2*cm, 6.5*cm - 0.2*cm])
dual2.setStyle(TableStyle([
("VALIGN",(0,0),(-1,-1),"TOP"),
("LEFTPADDING",(0,0),(-1,-1),2),
("RIGHTPADDING",(0,0),(-1,-1),4),
]))
story.append(dual2)
story.append(PageBreak())
# ═══════════════════════════════════════════════════════
# PAGE 5 – MASTER COMPARISON TABLE + TRACHEA RULE
# ═══════════════════════════════════════════════════════
story.append(section_banner("MASTER COMPARISON TABLE – Ek Nazar Mein Sabkuch", DARK_BLUE))
story.append(Spacer(1, 0.25*cm))
master_rows = [
["Normal", "Bilateral equal black", "Bilateral", "Midline", "Sharp", "<0.5", "–"],
["Pneumothorax", "Hyperlucent (extra black)", "Unilateral apex", "Normal / Away*","Sharp", "Normal", "Visceral pleural line, no lung markings beyond"],
["Pleural Effusion", "White base opacity", "Unilateral/bilateral","Away* (massive)","BLUNTED ★", "Normal", "Meniscus sign"],
["Pneumonia", "White lobar/segmental patch", "Lobar/segmental", "Normal", "Normal", "Normal", "Air bronchogram ★"],
["Pulmonary Edema", "Bilateral perihilar haze", "Perihilar bilateral", "Normal", "Blunted (bil)","ENLARGED","Kerley B + cephalization ★"],
["Collapse/Atelectasis","White – volume loss", "Affected lobe", "TOWARD ★", "Elevated hemi","Normal", "Fissure displacement, ipsilateral shift"],
["Miliary TB", "Tiny white dots 1-3mm", "Random bilateral", "Normal", "Normal", "Normal", "Uniform millet-seed nodules ★"],
["Cavitary TB", "White + black hole", "Upper lobe ★", "Normal", "Normal", "Normal", "Thick-walled cavity"],
["Cardiomegaly", "Normal lungs", "–", "Normal", "Normal", ">0.5 ★", "Rounded cardiac borders"],
["Pericardial Effusion","Normal lungs", "–", "Normal", "Normal", ">0.5", "FLASK / water-bottle heart ★"],
]
master_hdrs = ["Condition", "Color/Opacity", "Location", "Trachea", "CP Angle", "CTR", "Key Sign ★"]
master_cws = [3.2*cm, 3.5*cm, 3.0*cm, 2.2*cm, 2.0*cm, 1.5*cm, CW-15.4*cm]
mt = Table([
[Paragraph(h, table_header_style) for h in master_hdrs]
] + [
[Paragraph(str(c), table_cell_style) for c in row]
for row in master_rows
], colWidths=master_cws, repeatRows=1)
mt.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), DARK_BLUE),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,-1), 7.2),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING", (0,0), (-1,-1), 3),
("LEFTPADDING", (0,0), (-1,-1), 4),
("GRID", (0,0), (-1,-1), 0.4, MID_GREY),
("ROWBACKGROUNDS",(0,1), (-1,-1), [WHITE, LIGHT_GREY]),
("VALIGN", (0,0), (-1,-1), "TOP"),
# Highlight emergency rows
("BACKGROUND", (0,1), (-1,1), colors.HexColor("#EBF5FF")), # Normal
("BACKGROUND", (0,2), (-1,2), colors.HexColor("#FFF8E1")), # PTX
("BACKGROUND", (0,5), (-1,5), colors.HexColor("#FFF3CD")), # PNA
("BACKGROUND", (0,6), (-1,6), colors.HexColor("#F3E5F5")), # Edema
]))
story.append(mt)
story.append(Spacer(1, 0.4*cm))
# Trachea Rule box
story.append(section_banner("TRACHEA RULE – Yaad Karo", colors.HexColor("#1A6B3A")))
story.append(Spacer(1, 0.15*cm))
trachea_data = [
[
Paragraph("TRACHEA shifts AWAY from opacity", ParagraphStyle("tr1",fontSize=9,fontName="Helvetica-Bold",textColor=ACCENT_RED,leading=12)),
Paragraph("TRACHEA shifts TOWARD opacity", ParagraphStyle("tr2",fontSize=9,fontName="Helvetica-Bold",textColor=MED_BLUE,leading=12)),
],
[
Paragraph("= SPACE-OCCUPYING lesion\n(Effusion, Tension PTX, Large Tumor)", body_style),
Paragraph("= VOLUME-LOSING lesion\n(Collapse, Fibrosis, Post-pneumonectomy)", body_style),
]
]
trachea_tbl = Table(trachea_data, colWidths=[CW/2 - 0.2*cm, CW/2 - 0.2*cm])
trachea_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (0,-1), colors.HexColor("#FDECEA")),
("BACKGROUND", (1,0), (1,-1), colors.HexColor("#E3F0FF")),
("BOX", (0,0), (-1,-1), 1, MID_GREY),
("INNERGRID", (0,0), (-1,-1), 0.5, MID_GREY),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 8),
("VALIGN", (0,0), (-1,-1), "TOP"),
]))
story.append(trachea_tbl)
story.append(Spacer(1, 0.35*cm))
# Silhouette sign
story.append(section_banner("SILHOUETTE SIGN – Location Pehchano", colors.HexColor("#5D4037")))
story.append(Spacer(1, 0.15*cm))
sil_rows = [
["Right heart border BLUR", "Right Middle Lobe pathology"],
["Left heart border BLUR", "Lingula (Left Upper Lobe) pathology"],
["Diaphragm border BLUR", "Lower Lobe pathology (adjacent to diaphragm)"],
["Aortic knuckle BLUR", "Left Upper Lobe or adjacent pleural pathology"],
["Descending aorta BLUR", "Left Lower Lobe pathology"],
]
story.append(make_table(
["Border Blur", "Location Indicate Karta Hai"],
sil_rows,
[5.5*cm, CW - 5.5*cm - 0.1*cm],
header_color=colors.HexColor("#5D4037")
))
# ── Build ────────────────────────────────────────────────────────────────
doc.build(story, onFirstPage=add_page_deco, onLaterPages=add_page_deco)
print(f"PDF created: {OUT_PATH}")
if __name__ == "__main__":
build_pdf()
Running Command
python /home/daytona/workspace/cxr-reference-card/generate_pdf.py 2>&1
Running Command
ls -lh /home/daytona/workspace/cxr-reference-card/CXR_Quick_Reference.pdf && pyt…
PDF tayaar hai! ✅
5 pages, 7.3 MB - saari real textbook CXR images ke saath.
CXR Quick Reference
PDF Document · PDF
PDF mein kya hai:
| Page | Content |
|---|---|
| Page 1 | X-Ray density cheatsheet + Normal CXR anatomy table + ABCDE systematic approach |
| Page 2 | Pneumothorax (image + table) + Pleural Effusion (image + table) + Emergency box |
| Page 3 | Pulmonary Edema/CHF (Kerley B image) + Cardiomegaly/Cardiac chambers |
| Page 4 | Cavitary TB + Miliary TB + TB-HIV Hilar Adenopathy (3 real X-ray images) |
| Page 5 | Master Comparison Table (10 conditions ek saath) + Trachea Rule + Silhouette Sign |
Saare images real medical textbooks (Harrison's, Fishman's, Murray & Nadel, Fuster & Hurst's) se liye gaye hain - offline study ke liye perfect reference card hai.
This is a shared conversation. Sign in to Orris to start your own chat.