Stages of haemostasis, intrinsic & extrinsic pathway coagulation, Anticoagulants 10 marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive content. Let me compile the full answer.
Haemostasis, Coagulation Pathways & Anticoagulants
(Sources: Sabiston Textbook of Surgery 21e, Lippincott Illustrated Reviews: Pharmacology, Medical Physiology - Boron & Boulpaep, Bailey & Love's Short Practice of Surgery 28e)
STAGES OF HAEMOSTASIS
Haemostasis is the physiological process that arrests bleeding after vascular injury. It operates in four overlapping stages:
Stage 1 - Vascular Spasm (Vasoconstriction)
- The immediate response to vessel injury is reflex vasoconstriction of the damaged blood vessel.
- Mediated by local myogenic reflexes, nervous reflexes, and vasoactive amines (serotonin, thromboxane A2) released from activated platelets.
- Reduces blood flow to the injured site and buys time for platelet plug formation.
Stage 2 - Primary Haemostasis (Platelet Plug Formation)
This is the formation of a temporary, loose platelet plug. It occurs in three steps:
-
Platelet Adhesion: Disruption of the vascular endothelium exposes subendothelial collagen and von Willebrand factor (vWF). Platelets adhere via glycoprotein GPIb (binds vWF) and GPIa/IIa / GPVI (binds collagen directly).
-
Platelet Activation: Adherent platelets become activated - they change shape (from disc to spiky spheres) and release granule contents:
- Alpha (α) granules: fibrinogen, vWF, platelet factor 4, P-selectin, growth factors (PDGF, TGF-β, VEGF, EGF, FGF).
- Dense (δ) granules: ADP, ATP, serotonin, Ca²⁺.
- ADP and thromboxane A₂ recruit and activate further platelets (positive feedback).
-
Platelet Aggregation: Activated platelets expose GPIIb/IIIa receptors on their surface, which bind fibrinogen, cross-linking platelets into a platelet plug. This is the primary (temporary) haemostatic plug.
Stage 3 - Secondary Haemostasis (Coagulation Cascade)
Simultaneously, tissue factor (TF) exposed at the site of injury initiates the coagulation cascade, resulting in the formation of thrombin, which:
- Converts fibrinogen to fibrin monomers.
- Activates factor XIII → factor XIIIa cross-links fibrin into a stable, insoluble meshwork.
- Stabilises and reinforces the platelet plug.
- Amplifies the process by further activating factors V, VIII, and XI.
Stage 4 - Fibrinolysis (Clot Resolution)
- Once healing begins, the clot must be dissolved.
- Tissue plasminogen activator (tPA) converts plasminogen → plasmin.
- Plasmin digests fibrin into fibrin degradation products (FDPs) including D-dimers.
- Regulated by α₂-antiplasmin and plasminogen activator inhibitor-1 (PAI-1) to prevent excessive clot lysis.
THE COAGULATION CASCADE
The classical model describes two converging pathways activating a common pathway:
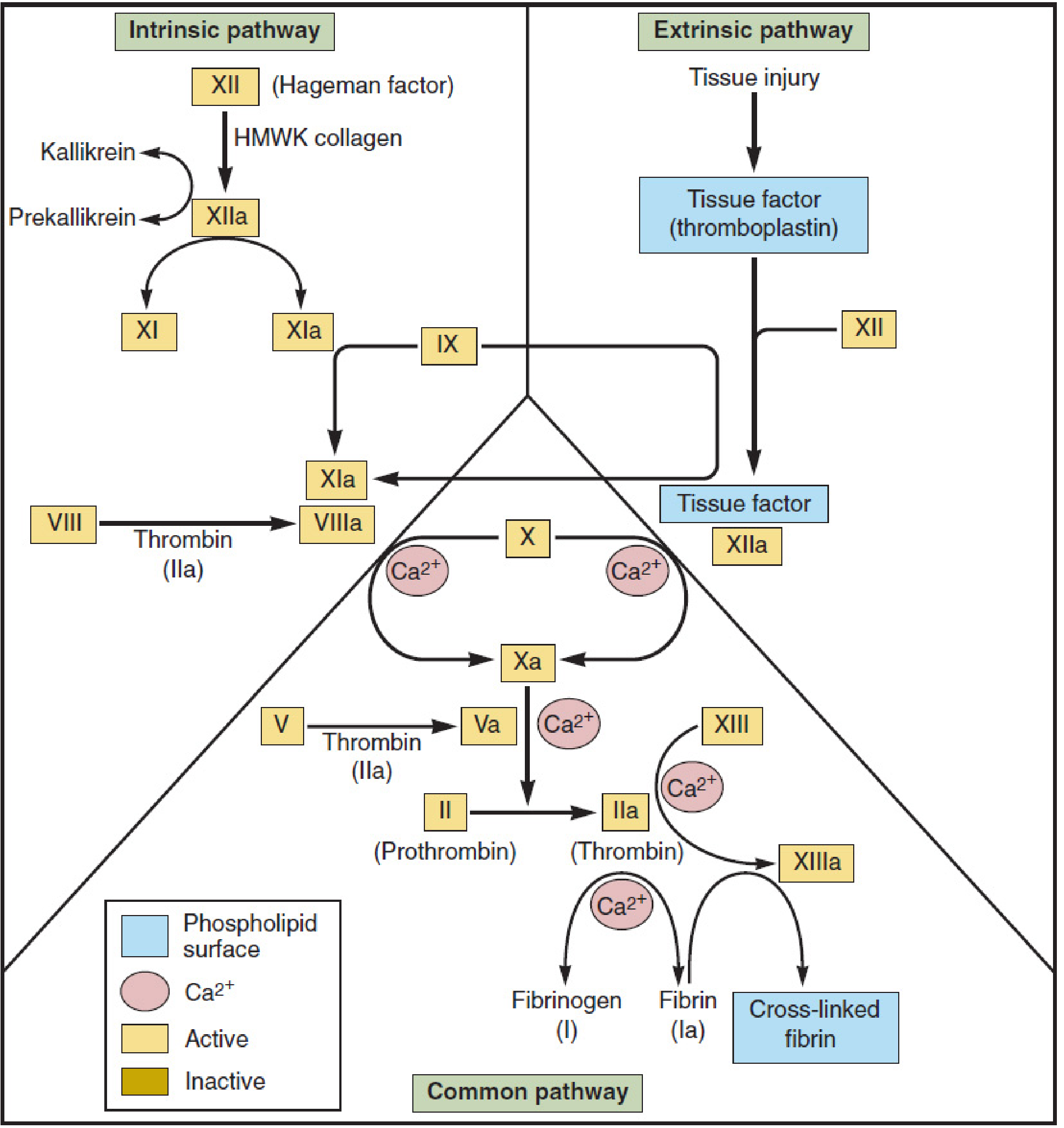
Classic coagulation cascade - Mulholland & Greenfield's Surgery
Extrinsic Pathway (Tissue Factor Pathway)
- Trigger: Vascular injury exposing tissue factor (TF / thromboplastin), a subendothelial transmembrane glycoprotein expressed on fibroblasts and vascular smooth muscle cells.
- TF binds and activates circulating factor VII → TF:FVIIa complex (extrinsic tenase complex).
- TF:FVIIa activates factor X → Xa and factor IX → IXa.
- Measured by: Prothrombin Time (PT / INR).
Intrinsic Pathway (Contact Activation Pathway)
- Trigger: Blood contact with a negatively charged surface (e.g., exposed subendothelial collagen, artificial surfaces, glass in vitro).
- Factor XII (Hageman factor) is activated → XIIa by HMWK + collagen.
- XIIa activates prekallikrein ↔ kallikrein feedback (amplification), and activates factor XI → XIa.
- XIa activates factor IX → IXa.
- IXa + factor VIIIa + Ca²⁺ + phospholipid surface = intrinsic tenase complex → activates factor X → Xa.
- Measured by: Activated Partial Thromboplastin Time (aPTT).
Common Pathway
Both pathways converge at factor X activation:
- Xa + Va + Ca²⁺ + phospholipid = prothrombinase complex
- Prothrombinase converts prothrombin (II) → thrombin (IIa)
- Thrombin cleaves fibrinogen (I) → fibrin monomers (Ia)
- Thrombin activates factor XIII → XIIIa
- XIIIa cross-links fibrin monomers into a stable, cross-linked fibrin clot
Cell-Based Model of Coagulation (Modern View)
The current accepted model replaces the separate pathways concept with three overlapping phases on cell membranes - as described in Sabiston Surgery:
| Phase | Location | Key Events |
|---|---|---|
| Initiation | TF-expressing cells | TF:FVIIa → activates FX → trace thrombin (thrombin "spark") |
| Amplification | Platelet surface | Trace thrombin activates FV, FVIII, FXI; platelets recruit and activate |
| Propagation | Activated platelet surface | Intrinsic tenase (IXa:VIIIa) → massive FXa → thrombin burst → fibrin |
KEY COAGULATION FACTORS TABLE
| Factor | Name | Pathway | Vitamin K-dependent? |
|---|---|---|---|
| I | Fibrinogen | Common | No |
| II | Prothrombin | Common | Yes |
| III | Tissue Factor | Extrinsic | No |
| V | Labile factor | Common | No |
| VII | Proconvertin | Extrinsic | Yes |
| VIII | Antihemophilic A | Intrinsic | No |
| IX | Christmas factor | Intrinsic | Yes |
| X | Stuart-Prower | Common | Yes |
| XI | PTA | Intrinsic | No |
| XII | Hageman | Intrinsic | No |
| XIII | Fibrin-stabilising | Common | No |
Vitamin K-dependent factors: II, VII, IX, X (also Protein C and Protein S - anticoagulants)
ANTICOAGULANTS
Classification
Anticoagulants
├── Parenteral
│ ├── Unfractionated Heparin (UFH)
│ ├── Low-Molecular-Weight Heparins (LMWH)
│ ├── Fondaparinux
│ └── Direct Thrombin Inhibitors (DTI): Argatroban, Bivalirudin
└── Oral
├── Vitamin K Antagonist: Warfarin
└── DOACs (Direct Oral Anticoagulants)
├── Factor Xa inhibitors: Rivaroxaban, Apixaban, Edoxaban
└── Direct Thrombin Inhibitor: Dabigatran
1. Unfractionated Heparin (UFH)
- Route: IV or SC injection.
- Mechanism: Binds antithrombin III (AT-III), causing a conformational change that accelerates AT-III inhibition of thrombin (IIa) and factor Xa by ~1000-fold. Also inhibits IXa, XIa, XIIa.
- Monitoring: aPTT (target 60-100 sec, or 1.5-2.5× normal).
- Reversal: Protamine sulfate (1 mg neutralises ~100 units heparin).
- Adverse effects:
- Bleeding (most common).
- Heparin-Induced Thrombocytopenia (HIT): immune-mediated, IgG antibodies against heparin-PF4 complex → paradoxical thrombosis. Stop heparin immediately; replace with argatroban.
- Osteoporosis (long-term use).
- Advantages: Rapid onset, reversible, can be used in pregnancy (does not cross placenta).
2. Low-Molecular-Weight Heparins (LMWH) - Enoxaparin, Dalteparin
- Mechanism: Complex with AT-III → primarily inhibit factor Xa (anti-Xa activity); less effect on thrombin vs. UFH.
- Advantages over UFH: More predictable pharmacokinetics, SC administration, no routine monitoring needed, lower risk of HIT.
- Monitoring: Anti-Xa levels (in obesity, renal failure, pregnancy).
- Reversal: Protamine sulfate (incomplete - ~60-75% reversal of anti-Xa activity).
- Use in renal impairment: Use cautiously; accumulate in renal failure → prefer UFH.
3. Fondaparinux
- Mechanism: Synthetic pentasaccharide that selectively binds AT-III → selective factor Xa inhibition (no direct anti-IIa effect).
- 300-1000-fold potentiation of AT-III's Xa inhibition.
- No reversal agent (no protamine effect; andexanet alfa may be considered).
- No HIT risk (does not bind PF4).
4. Warfarin (Vitamin K Antagonist)
- Route: Oral.
- Mechanism: Inhibits vitamin K epoxide reductase (VKOR), preventing regeneration of reduced (active) Vitamin K. Without active Vit K, the hepatic γ-carboxylation of factors II, VII, IX, X, Protein C, Protein S is impaired → non-functional coagulation factors.
- Onset: Delayed - 3-5 days (circulating factors must be cleared; shortest half-life is factor VII, so PT prolongs first, then full effect takes 5+ days).
- Monitoring: INR (International Normalised Ratio). Therapeutic INR: 2.0-3.0 for most indications; 2.5-3.5 for mechanical heart valves.
- Reversal:
- Mild/no bleeding: Withhold warfarin ± oral Vit K.
- Serious bleeding: IV Vitamin K + 4-factor Prothrombin Complex Concentrate (4F-PCC) or Fresh Frozen Plasma (FFP).
- Life-threatening: 4F-PCC + IV Vitamin K.
- Drug interactions: Extensive (inhibits/induces CYP2C9). Narrow therapeutic window.
- Contraindicated in pregnancy (crosses placenta - warfarin embryopathy in 1st trimester).
- Bridging: During initiation, overlap with heparin/LMWH for 5 days until INR therapeutic (because Protein C and S - anticoagulants - have short half-lives and may drop before coagulation factors, creating a transient hypercoagulable state).
5. Direct Thrombin Inhibitors (DTI) - Argatroban, Bivalirudin
- Mechanism: Directly and reversibly inhibit thrombin (IIa) - both free and clot-bound thrombin - without requiring AT-III.
- Argatroban: Derived from L-arginine; hepatically metabolised. Used in HIT.
- Bivalirudin: Hirudin analogue; renally excreted (t½ 25 min). Used in PCI in HIT patients.
- Monitoring: aPTT or ACT.
6. Direct Oral Anticoagulants (DOACs)
| Drug | Target | Reversal Agent |
|---|---|---|
| Dabigatran | Direct thrombin inhibitor (IIa) | Idarucizumab (monoclonal antibody) |
| Rivaroxaban | Direct factor Xa inhibitor | Andexanet alfa |
| Apixaban | Direct factor Xa inhibitor | Andexanet alfa |
| Edoxaban | Direct factor Xa inhibitor | Andexanet alfa |
- Advantages: Fixed dosing, no routine monitoring, fewer food/drug interactions vs. warfarin, predictable pharmacokinetics.
- Disadvantages: No routine monitoring, renally cleared (use cautiously in CKD), contraindicated in pregnancy, expensive.
NATURAL ANTICOAGULANT MECHANISMS
The body restricts clotting to the injury site through:
- Antithrombin III (AT-III): Serine protease inhibitor - slowly inactivates thrombin, Xa, IXa, XIa, XIIa. Accelerated 1000× by heparin.
- Protein C + Protein S: Vitamin K-dependent. Activated Protein C (APC) + Protein S inactivate factors Va and VIIIa, limiting coagulation. Thrombomodulin on endothelium activates Protein C.
- Tissue Factor Pathway Inhibitor (TFPI): Inhibits the TF:VIIa:Xa complex, limiting the extrinsic pathway after initial activation.
- Prostacyclin (PGI₂) and NO: Released by intact endothelium; inhibit platelet activation and cause vasodilation.
CLINICAL CORRELATION - COAGULATION TESTS
| Test | Pathway Tested | Normal | Prolonged by |
|---|---|---|---|
| PT/INR | Extrinsic + Common (VII, X, V, II, I) | 12-15 sec / INR 1.0 | Warfarin, Vitamin K deficiency, liver disease |
| aPTT | Intrinsic + Common (XII, XI, IX, VIII, X, V, II, I) | 25-35 sec | Heparin, Haemophilia A/B, DIC |
| Thrombin Time (TT) | Common (fibrinogen to fibrin) | 14-16 sec | Heparin, low/abnormal fibrinogen |
| Platelet count | Primary haemostasis | 150,000-400,000/µL | ITP, TTP, HIT, DIC |
| Bleeding Time | Platelet function & vascular integrity | 3-9 min | Aspirin, vWD, thrombocytopenia |
SUMMARY DIAGRAM - SITES OF ANTICOAGULANT ACTION
Intrinsic: XII→XIIa→XI→XIa→IX→IXa
↘
X → Xa ← TF:VIIa (Extrinsic)
↓
Heparin/LMWH → [AT-III] blocks Xa ← FONDAPARINUX blocks Xa
↓
Prothrombin (II) → Thrombin (IIa)
↑
WARFARIN blocks synthesis of II, VII, IX, X
ARGATROBAN/BIVALIRUDIN/DABIGATRAN block IIa
↓
Fibrinogen → Fibrin → Cross-linked Fibrin
Sources: Sabiston Textbook of Surgery 21e, Ch. 100 | Lippincott Illustrated Reviews: Pharmacology | Medical Physiology - Boron & Boulpaep, Ch. 18 | Bailey & Love's Short Practice of Surgery 28e, Ch. 3
This is a shared conversation. Sign in to Orris to start your own chat.