Pulmonary tb in children
Reading File
Finding Sources
Searching PubMed
"tuberculosis"[MeSH Terms] AND "child"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
I now have very comprehensive material. Let me compile the complete answer.
Pulmonary Tuberculosis in Children
Pulmonary TB in children differs substantially from adult TB in its pathogenesis, clinical presentation, diagnosis, and treatment. Below is a detailed, evidence-based review drawn primarily from the Red Book 2021 (AAP) and Park's Textbook of Preventive & Social Medicine.
1. Epidemiology
- Childhood TB is largely a marker of failure of TB control in adults - children are exposed via infectious adult contacts, especially smear-positive parents or household members.
- Children under 5 years are most vulnerable; up to 20% of exposed infants develop disease within 2 years of infection.
- The commonest age of childhood TB disease is 1-4 years.
- Risk is higher in urban, low-income populations; immigrants, refugees, and international adoptees are disproportionately affected.
- Children rarely have smear-positive TB and are not significant sources of transmission.
- A diagnosis of TB infection (TBI) or TB disease in a young child is a public health sentinel event, often representing recent community transmission. - Red Book 2021, p.1214
2. Pathogenesis
- Transmission is via airborne droplet nuclei produced by an adult/adolescent with contagious pulmonary, endobronchial, or laryngeal TB.
- After inhalation, bacteria reach alveoli and are taken up by macrophages. Cell-mediated immunity (CMI) develops over 2-10 weeks - this is when the TST/IGRA becomes positive.
- Primary (Ghon) complex forms: a sub-pleural focus + regional lymphadenopathy. In most children this heals without progression.
- Young age, immunodeficiency, malnutrition, and HIV increase the risk of progressive primary disease or dissemination (miliary TB, TB meningitis).
3. Risk Factors for Progression from Infection to Disease
| Risk Factor | Notes |
|---|---|
| Age < 5 years or postpubertal adolescent | Immature/altered immunity |
| HIV infection | Most important risk factor |
| TNF-alpha antagonists / immunosuppressants | Biologic therapy, prolonged corticosteroids |
| Malnutrition | Undernutrition significantly increases susceptibility |
| Diabetes mellitus | |
| Chronic renal failure | |
| Recent infection (< 2 years) | Highest risk window |
| Hodgkin disease, lymphoma |
4. Clinical Features
Children with pulmonary TB commonly present with:
- Persistent fever >= 2 weeks without a known cause
- Unremitting cough >= 2 weeks
- Weight loss of >= 5% in 3 months or failure to gain weight over 3 months
- Night sweats, fatigue, loss of appetite
- Lymphadenopathy (hilar, mediastinal, cervical)
Important: Infants and young children may have non-specific symptoms (poor feeding, failure to thrive) without prominent respiratory symptoms. Classic adult features (cavitation, haemoptysis) are rare in children.
Complications to watch for:
- Bronchial compression by enlarged lymph nodes
- Pleural effusion
- Miliary spread (especially in infants < 12 months - always do lumbar puncture to rule out TB meningitis in this age group)
5. Diagnosis
5a. Approach
Diagnosis rests on four pillars: microbiological confirmation + chest X-ray + TST/IGRA + clinical/contact history.
"Diagnosis of tuberculosis should not be made only on clinical features, and further investigations are always necessary." - Park's Textbook
5b. Diagnostic Algorithm (RNTCP/IAP)
The flowchart below (from Park's) summarises the national approach:
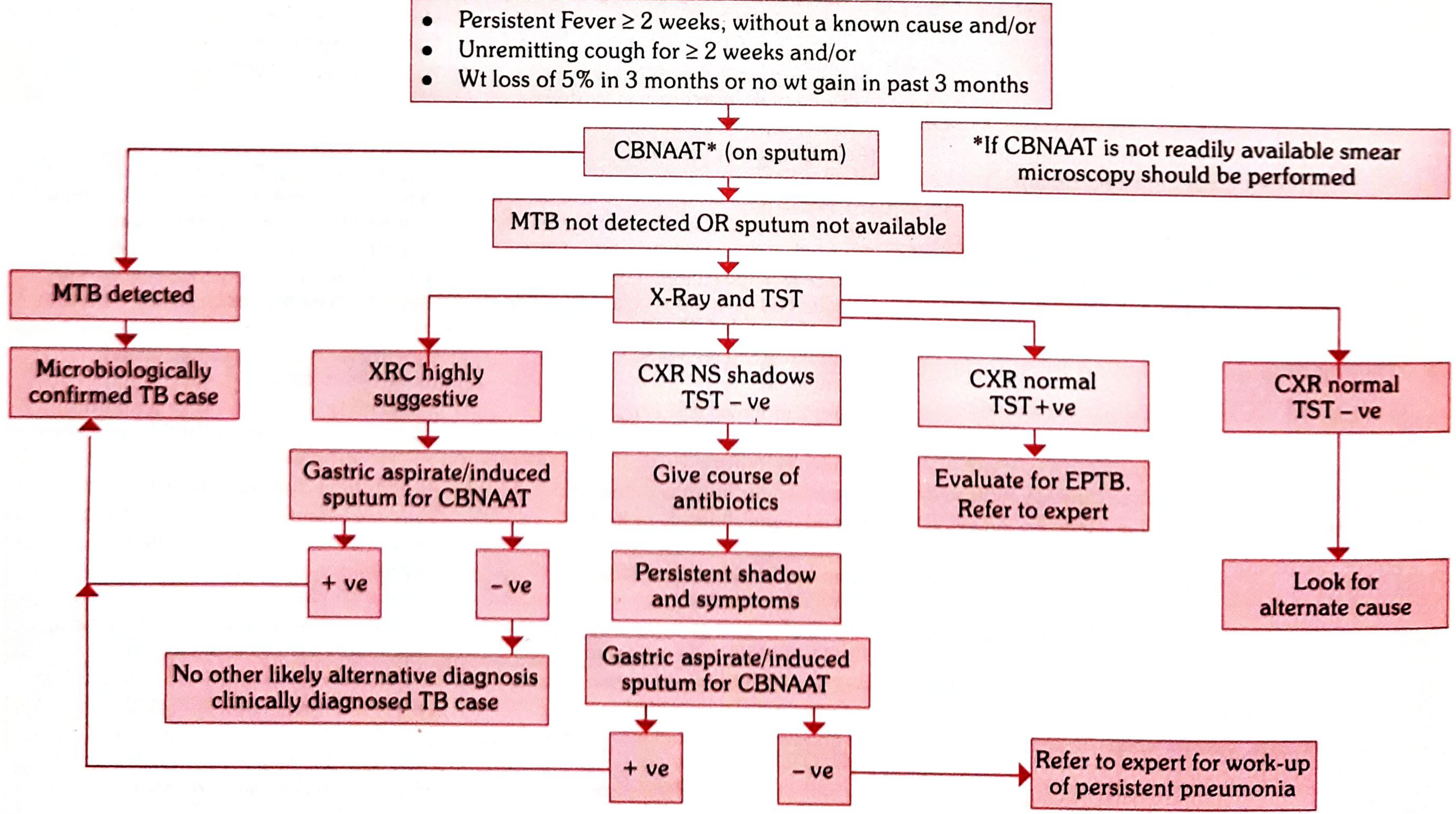
Fig. 4 - Diagnostic algorithm for paediatric pulmonary TB (Park's Textbook of Preventive & Social Medicine)
Key decision points:
- Start with CBNAAT (Xpert MTB/RIF) on sputum - preferred test
- If MTB detected → Microbiologically confirmed TB
- If MTB not detected or sputum unavailable → proceed to Chest X-ray + TST (Mantoux)
- X-ray highly suggestive (miliary, lymphadenopathy, fibrocavitatory) → collect gastric aspirate or induced sputum for CBNAAT
- X-ray non-specific shadows + TST negative → trial of antibiotics (NOT quinolones, linezolid, or Amox-clav as these have anti-TB activity); if shadows persist, collect GA/IS for CBNAAT
- X-ray normal + TST positive → Evaluate for extrapulmonary TB; refer to expert
- X-ray normal + TST negative → Look for alternative diagnosis
5c. Specimen Collection
- Children > 2 years and adolescents: induced sputum (nebulised hypertonic saline)
- Children unable to produce sputum: early-morning gastric aspirate (GA) via nasogastric tube, before ambulation or feeding - collected on 3 separate mornings for AFB stain and culture
- Bronchial washing or bronchoalveolar lavage if available
- Fluorescent staining (auramine) is preferred over traditional Kinyoun acid-fast smear
"The best specimen for diagnosis of pulmonary TB in any child or adolescent in whom cough is absent or nonproductive and sputum cannot be induced is an early-morning gastric aspirate." - Red Book 2021, p.1221
5d. TST (Mantoux) Interpretation in Children
- Intradermal injection of 2 TU of PPD RT-23 (India) or 5 TU PPD-S (USA); read at 48-72 hours
- Positive cutoffs:
| Induration | Considered Positive In |
|---|---|
| >= 5 mm | HIV-infected; immunosuppressed; close contacts of confirmed TB; CXR findings consistent with TB |
| >= 10 mm | Children < 5 yrs; children with risk factors; recent immigrants from high-prevalence areas; medically underserved populations |
| >= 15 mm | Children >= 5 yrs with no risk factors |
- BCG vaccination does not contraindicate TST, but IGRA is preferred in BCG-vaccinated children to avoid false positives.
- TST/IGRA positivity indicates infection (TBI), not necessarily active disease. Chest X-ray and clinical evaluation are required to distinguish TBI from active disease.
5e. IGRA (Interferon-Gamma Release Assay)
- Examples: QuantiFERON-TB Gold Plus, T-SPOT.TB
- Not recommended for children < 2 years (limited data)
- Preferred over TST in BCG-vaccinated children
- Cannot distinguish TBI from active disease
5f. Chest X-Ray Findings
| Pattern | Significance |
|---|---|
| Hilar / mediastinal lymphadenopathy | Most common in children; "highly suggestive" |
| Miliary pattern | Haematogenous spread; urgent |
| Primary focus (Ghon focus) + hilar node (Ghon complex) | Classic primary TB |
| Consolidation / lobar collapse | Due to airway compression by nodes |
| Pleural effusion | Particularly in older children/adolescents |
| Cavitation | Uncommon in young children; more in adolescents |
6. Treatment
6a. Drug-Susceptible Pulmonary TB (First-Line)
The standard regimen is RIPE (Rifampin, Isoniazid, Pyrazinamide, Ethambutol):
| Phase | Drugs | Duration |
|---|---|---|
| Intensive phase | Rifampin (R) + Isoniazid (H) + Pyrazinamide (Z) + Ethambutol (E) | 2 months |
| Continuation phase | Rifampin (R) + Isoniazid (H) | 4 months |
| Total | 6 months |
Modifications:
- If cavitation on CXR or sputum culture positive at 2 months → extend to 9 months
- If only hilar adenopathy with no drug resistance risk → 3-drug regimen (HRZ x 2 months, then HR x 4 months) may be used by some experts
- DOT (Directly Observed Therapy) is strongly recommended for all children and adolescents
"A 6-month, 4-drug regimen... is recommended for treatment of pulmonary disease, pulmonary disease with hilar adenopathy, and hilar adenopathy disease in infants, children, and adolescents." - Red Book 2021, p.1230
6b. Paediatric Doses (WHO/RNTCP)
| Drug | Dose (mg/kg/day) | Max daily dose |
|---|---|---|
| Isoniazid (H) | 10 mg/kg (range 7-15) | 300 mg |
| Rifampin (R) | 15 mg/kg (range 10-20) | 600 mg |
| Pyrazinamide (Z) | 35 mg/kg (range 30-40) | 2000 mg |
| Ethambutol (E) | 20 mg/kg (range 15-25) | 1000 mg |
India uses weight-band-based fixed-dose combination (FDC) tablets in pre-packaged patient-wise boxes, including dedicated paediatric FDC tablets.
6c. Special Situations
| Situation | Recommendation |
|---|---|
| HIV co-infection | Start TB treatment first; commence ART after 2-8 weeks; do not use rifampin with certain PIs |
| MDR-TB | Consult expert; include 4-6 drugs susceptible to the strain; treat for at least 12 months after culture conversion (24 months if HIV+) |
| Extrapulmonary TB (bone, joint, disseminated) | 9-12 months depending on site |
| TB meningitis | 12 months + corticosteroids |
| Congenital TB | RIPE ± aminoglycoside immediately; add corticosteroids if meningitis confirmed |
7. TB Preventive Therapy (Chemoprophylaxis)
Isoniazid (INH) 10 mg/kg/day for 6 months is given to:
- a. All asymptomatic contacts < 6 years of a smear-positive case, regardless of BCG status (after ruling out active disease)
- b. All HIV-infected children with known TB exposure or TST >= 5 mm, without active disease
- c. All TST-positive children on immunosuppressive therapy (nephrotic syndrome, acute leukemia, etc.)
- d. Newborns of mothers diagnosed with TB in pregnancy - 6 months of prophylaxis, then BCG vaccination
Red Book 2021 recommends 9 months of INH for TBI in the United States (30% more efficacious than 6 months). Alternatively, rifampin x 4 months is used when the source case has isoniazid-resistant TB.
8. BCG Vaccination
- BCG (Bacille Calmette-Guerin) is given at birth in high-burden countries (India's Universal Immunization Programme).
- Protects against miliary TB and TB meningitis in young children (up to 80% efficacy for severe forms).
- Does NOT reliably prevent pulmonary TB in adults.
- BCG does not eliminate the need for TB chemoprophylaxis in high-risk contacts.
9. Drug-Resistant TB in Children - Key Principles
- Always treat in consultation with an expert
- Include at least 4-6 bactericidal drugs to which the strain is susceptible
- Never add a single drug to a failing regimen
- Treat for at least 12 months after culture conversion (24 months if HIV+)
- Bedaquiline and delamanid are options for pre-XDR/XDR-TB in older children
10. Monitoring During Treatment
- Monthly clinical assessment and weight measurement
- CXR at 2 months and end of treatment
- Monthly sputum culture if microbiologically confirmed
- Watch for drug toxicity: isoniazid (hepatotoxicity, peripheral neuropathy), rifampin (hepatotoxicity, orange body fluids), ethambutol (optic neuritis - use with caution in young children who cannot report visual changes), pyrazinamide (hepatotoxicity, hyperuricaemia)
Sources
- Red Book 2021: Report of the Committee on Infectious Diseases, AAP - pp. 1214-1238
- Park's Textbook of Preventive & Social Medicine - Paediatric TB section
- Oral swabs with rapid molecular diagnostic for pulmonary TB in adults and children - Lancet Global Health, 2024 (systematic review, PMID: 38097297)
This is a shared conversation. Sign in to Orris to start your own chat.