IMNCI paediatrics from op ghai in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching the Web
OP Ghai paediatrics IMNCI integrated management neonatal childhood illness detailed notes
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent! I have comprehensive content. Now I'll compile the full detailed IMNCI response based on Park's (which aligns with Ghai 8th edition on IMNCI) and the supplementary web sources.
IMNCI - Integrated Management of Neonatal and Childhood Illness
(As per OP Ghai Paediatrics & Park's Preventive Medicine)
1. Background and Origin
IMCI (Integrated Management of Childhood Illness) was developed jointly by WHO and UNICEF in the mid-1990s as a strategy to reduce childhood morbidity and mortality. The Indian version was renamed IMNCI - Integrated Management of Neonatal and Childhood Illness - because it was extended to include the first 7 days of life (neonatal period), which is not covered in the original WHO IMCI.
IMNCI is the central pillar of child health interventions under the RCH II / NRHM strategy in India.
2. Rationale / Why IMNCI?
- Most sick children present with signs and symptoms of more than one condition simultaneously (diarrhoea + malnutrition + fever, etc.)
- A single diagnosis is often not possible or appropriate
- Treatment is complicated by the need to combine therapies
- An integrated approach is therefore necessary - looking beyond single-disease treatment
- Evidence from NFHS-III showed: ARI (17%), diarrhoea (13%), fever (27%), undernutrition (43%) were the commonest morbidities in children under 3 years in India
- Coverage of measles vaccination in 12-23 month children was also low
The 5 major childhood killers addressed: ARI, Diarrhoea, Malaria, Measles, Malnutrition (together responsible for >90% of under-5 mortality).
3. Indian Adaptations (IMNCI vs. WHO IMCI)
The Indian adaptation of IMCI differs in the following key ways:
| Feature | Original IMCI | Indian IMNCI |
|---|---|---|
| Age range | 1 week - 5 years | 0-7 days included |
| Neonatal focus | Limited | Equal training time for sick young infant |
| National guidelines | Generic | Incorporates India's malaria, anaemia, Vit-A, immunization schedule |
| Training orientation | Child-heavy | Begins with sick young infants up to 2 months |
Five key highlights of Indian adaptation:
- Inclusion of 0-7 days age group
- Incorporation of national guidelines on malaria, anaemia, Vitamin A supplementation, and immunization schedule
- Training begins with sick young infants up to 2 months
- Training time devoted to sick young infant and sick child is almost equal
- Skill-based training approach
4. Objectives of IMNCI
- Reduce death, illness, and disability in children under 5 years
- Promote improved growth and development
- Improve case management skills of healthcare workers
- Improve the health system (supply chain, referral)
- Improve family and community health practices
5. Three Main Components (Pillars)
Component 1: Improving Case Management Skills of Healthcare Staff
- Health workers are trained to use IMNCI guidelines
- Covers assessment, classification, treatment, counselling, follow-up
Component 2: Improving the Health System
- Referral pathways, drug supply, laboratory support
- Training and supervision systems
Component 3: Improving Family and Community Practices
- Teaching families when to seek care
- Promoting key family practices (breastfeeding, nutrition, hygiene, immunization, home management)
6. Two Age Groups in IMNCI
IMNCI case management charts are designed for two distinct age groups:
| Group | Age | Focus |
|---|---|---|
| Sick Young Infant | 0 up to 2 months (includes 0-7 days neonate) | Neonatal sepsis, jaundice, feeding problems, LBW |
| Sick Child | 2 months up to 5 years | ARI, diarrhoea, fever, malaria, measles, malnutrition, ear problems |
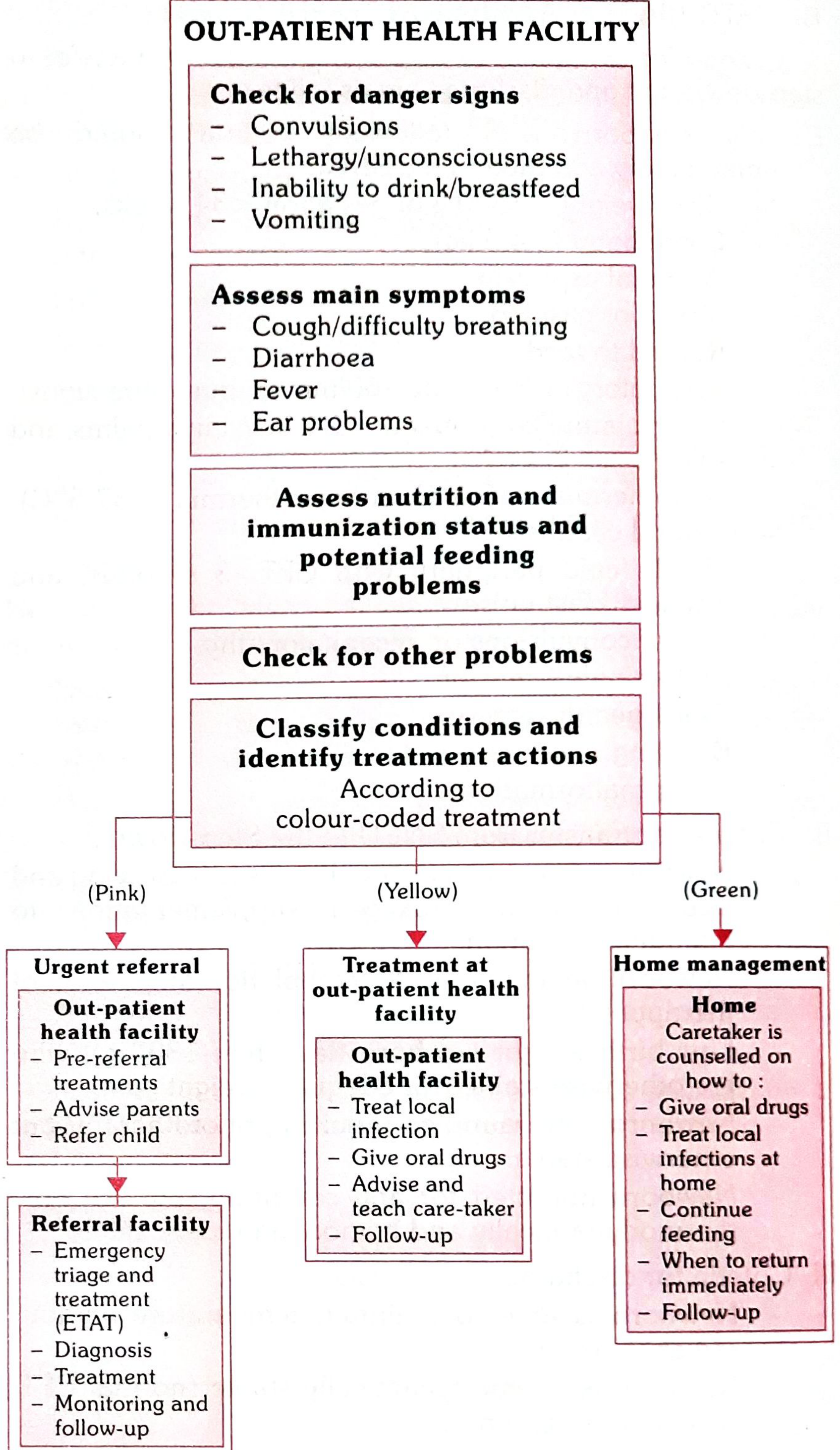
7. The IMNCI Case Management Process - 6 Steps
The stepwise approach used by a trained health worker at an outpatient health facility:
Step 1: ASSESS the condition
- History taking and physical examination using a structured checklist
- For children 2 months - 5 years, assess:
- General danger signs (convulsions, lethargy/unconsciousness, inability to drink/breastfeed, vomiting everything)
- Main symptoms: Cough/difficulty breathing, Diarrhoea, Fever, Ear problems
- Nutrition and immunization status, potential feeding problems
- Other problems
- For young infants (0-2 months), assess for:
- Possible serious bacterial infection
- Jaundice
- Diarrhoea
- Feeding problem/low weight
- Immunization status
Step 2: CLASSIFY the illness
- Uses a colour-coded triage system (traffic-light system):
- 🔴 Pink - Severe classification - Urgent pre-referral treatment and referral
- 🟡 Yellow - Moderate classification - Specific medical treatment and advice at outpatient facility
- 🟢 Green - Mild classification - Simple advice on home management
Step 3: IDENTIFY treatment
- After classifying all conditions, identify specific treatments
- If pink: give essential pre-referral treatment (e.g., first dose antibiotic, oral anti-malarial, IM vitamin K), then refer
- If yellow: develop integrated treatment plan, give first dose of drugs in clinic
- If green: advise on home management
- If immunization needed: give it
Step 4: TREAT
- Give oral drugs
- Treat local infections at the facility
- Teach caretaker how to give oral drugs at home
- Instruct on feeding and fluid management during illness
Step 5: COUNSEL the mother/caretaker
- Ask and listen to problems already being done
- Praise what is being done correctly
- Advise and teach new skills
- Check understanding
- Counsel about her own health
- Assess breastfeeding practices
- Teach danger signs to return immediately
Step 6: FOLLOW UP
- Give dates for scheduled return visit
- On return: give follow-up care and reassess for new problems
Visual summary of the IMNCI case management process:
8. General Danger Signs (Children 2 Months - 5 Years)
A child with ANY of these signs should be classified Pink and referred urgently:
- Convulsions (current or in this illness)
- Lethargy or unconsciousness
- Inability to drink or breastfeed
- Vomiting everything
9. Classification Tables (Key Examples)
Cough / Difficulty Breathing
| Signs | Classification | Action |
|---|---|---|
| Stridor + chest in-drawing OR central cyanosis | SEVERE PNEUMONIA (Pink) | Refer urgently, first dose amoxicillin |
| Fast breathing only (RR ≥ 50/min in 2-12 mo; ≥ 40/min in 1-5 yr) | PNEUMONIA (Yellow) | Oral amoxicillin 5 days |
| No signs of pneumonia | NO PNEUMONIA: cough/cold (Green) | Soothe throat, home care |
Fast breathing cut-offs:
- 2 months - 12 months: ≥50 breaths/min
- 12 months - 5 years: ≥40 breaths/min
Diarrhoea
| Signs | Classification | Action |
|---|---|---|
| 2+ of: sunken eyes, very slow skin pinch, lethargic, not drinking | SEVERE DEHYDRATION (Pink) | IV fluids, refer |
| 2+ of: restless/irritable, sunken eyes, drinks eagerly, skin pinch slowly | SOME DEHYDRATION (Yellow) | ORS Plan B |
| No signs | NO DEHYDRATION (Green) | ORS Plan A at home |
| Diarrhoea >14 days + dehydration | SEVERE PERSISTENT DIARRHOEA (Pink) | Refer |
| Diarrhoea >14 days without dehydration | PERSISTENT DIARRHOEA (Yellow) | Treat |
| Blood in stool | DYSENTERY (Yellow) | Cotrimoxazole |
Fever
| Signs | Classification | Action |
|---|---|---|
| Stiff neck OR petechiae/purpura | VERY SEVERE FEBRILE DISEASE (Pink) | Refer urgently |
| Malaria risk area + fever | MALARIA (Yellow) | Antimalarials |
| Measles with complication | SEVERE COMPLICATED MEASLES (Pink) | Refer |
| Measles (no complication) | MEASLES (Yellow) | Vitamin A |
Malnutrition Assessment
| Signs | Classification |
|---|---|
| Visible severe wasting OR bilateral oedema OR MUAC <115 mm | SEVERE ACUTE MALNUTRITION (Pink) |
| MUAC 115-125 mm OR weight-for-height -2 to -3 SD | MODERATE ACUTE MALNUTRITION (Yellow) |
| Normal | NO MALNUTRITION (Green) |
10. Sick Young Infant (0 up to 2 months) - Key Assessments
Possible Serious Bacterial Infection (PSBI) / Sepsis
Signs to look for:
- Convulsions
- Respiratory rate ≥60/min
- Severe chest in-drawing
- Nasal flaring
- Grunting
- Bulging fontanelle
- Purulent umbilical discharge with redness
- Temperature >37.5°C or <35.5°C (or feels hot/cold)
- Many/severe skin pustules
- Lethargic or unconscious
- Reduced movement
Pink classification - refer with benzylpenicillin + gentamicin
Jaundice
- Jaundice appearing <24 hrs - Severe (Pink), refer
- Jaundice appearing >24 hrs, not reaching palms/soles - Jaundice (Yellow), counsel, follow up
- Yellow palms and soles = Severe jaundice (Pink)
Feeding Problem / Low Weight
- Weight <2000 g or extremely small
- Not feeding well (poor attachment, less than 8 feeds/day, receives other food/drink)
- Exclusive breastfeeding counselling is key
11. Variants: F-IMNCI and C-IMNCI
Facility-Based IMNCI (F-IMNCI)
- Integration of facility-based care with IMNCI package
- Empowers health personnel to manage newborn and childhood illness at health facility level
- Focuses on inpatient management of: asphyxia, sepsis, LBW, pneumonia, diarrhoea, malaria, meningitis, severe malnutrition
- Master trainers at state and district level = paediatricians from tertiary hospitals and medical colleges
Community IMNCI (C-IMNCI)
- Targets community-level care
- Implemented at:
- Household level
- Sub-centre level through ANMs
- PHC level through medical officers, nurses, LHVs
- Focusses on preventive, promotive, and curative aspects
Pre-service IMNCI
- Being included in curriculum of medical colleges across India
- Accepted as strategy to scale up IMNCI by Government of India
- Helps provide trained IMNCI manpower in both public and private sectors
12. Levels of Care and Facility-Based Newborn Care
| Health Facility Level | All Newborns | Sick Newborns |
|---|---|---|
| PHC/Sub-centre (MCH Level I) | Newborn Care Corner (NBCC) in labor room | Prompt referral |
| CHC/FRU (MCH Level II) | NBCC in labor room + OT | Newborn Stabilization Unit (NBSU) |
| District Hospital (MCH Level III) | NBCC in labor room + OT | Special Newborn Care Unit (SNCU) |
13. Key Drugs Used in IMNCI
| Drug | Condition | Dose |
|---|---|---|
| Amoxicillin (oral) | Pneumonia | 40 mg/kg/day in 2 divided doses x 5 days |
| Cotrimoxazole | Dysentery | Trimethoprim 5 mg/kg/day in 2 doses x 5 days |
| Benzylpenicillin + Gentamicin | Neonatal PSBI (refer with pre-referral dose) | |
| ORS | Dehydration | As per plan |
| Zinc | Diarrhoea | <6 months: 10 mg/day; >6 months: 20 mg/day x 10-14 days |
| Vitamin A | Measles / Deficiency | 100,000 IU (<1 yr), 200,000 IU (>1 yr) |
| Chloroquine/Artesunate | Malaria | As per national guidelines |
| Paracetamol | Fever/pain | 15 mg/kg/dose |
14. Counselling for Feeding
Key IMNCI counselling points on feeding:
- Exclusive breastfeeding for first 6 months
- Initiation of breastfeeding within 1 hour of birth
- Appropriate complementary feeding from 6 months
- Continue breastfeeding up to 2 years and beyond
- Feed the child more frequently during illness and extra food after illness
- How to correctly attach infant to breast
15. When to Return Immediately (Danger Signs Taught to Caretakers)
Caretakers are taught to bring the child back immediately if:
- The child is unable to drink or breastfeed
- The child becomes sicker
- Child develops fever
- Child has fast or difficult breathing
- Blood in stool
- Drinking poorly
16. Limitations of IMNCI Guidelines
- Does not address all major reasons a sick child presents to clinic
- Does not cover trauma or acute emergencies from accidents/injuries
- HIV/AIDS not addressed specifically (though diarrhoea and respiratory infections in HIV children are managed by standard guidelines)
- Children with chronic problems or uncommon illnesses may need special/referral care
- Case management is only effective if families bring children early to trained providers
17. Associated Programmes Linked to IMNCI
| Programme | Focus |
|---|---|
| NSSK (Navjat Shishu Suraksha Karyakram) | Basic newborn care and resuscitation at birth |
| SNCU (Special Newborn Care Unit) | Sick newborn inpatient care at district hospitals |
| NBSU (Newborn Stabilization Unit) | Sick newborn stabilization at CHCs/FRUs |
| NBCC (Newborn Care Corner) | Essential newborn care at all delivery points |
| NRC (Nutrition Rehabilitation Centre) | SAM management |
| RBSK (Rashtriya Bal Swasthya Karyakram) | Screening for 4Ds: defects, diseases, deficiencies, developmental delays in children 0-18 years |
Summary Table: IMNCI at a Glance
| Parameter | Detail |
|---|---|
| Full form | Integrated Management of Neonatal and Childhood Illness |
| Developed by | WHO + UNICEF (Indian version by MoHFW) |
| Target age | 0 days to 5 years (Indian IMNCI includes 0-7 days) |
| Programme umbrella | RCH II / NRHM |
| Major illnesses addressed | ARI, Diarrhoea, Malaria, Measles, Malnutrition |
| Case management steps | Assess → Classify → Identify → Treat → Counsel → Follow up |
| Colour code | Pink (refer) / Yellow (treat OPD) / Green (home care) |
| Two age-group charts | 0-2 months + 2 months-5 years |
| Three components | Case management skills + Health system + Family/community |
| Indian addition vs IMCI | Includes 0-7 days neonates |
Source: Park's Textbook of Preventive and Social Medicine (Chapter 7 & 8), which is the standard cross-reference for IMNCI in OP Ghai's Essential Paediatrics, 8th edition. The IMNCI content in Ghai is based on the same WHO/MoHFW IMNCI framework and national guidelines.
This is a shared conversation. Sign in to Orris to start your own chat.