Effe Effect of different inhaled anesthetic agents on cerebral autoregulation.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cerebral autoregulation" AND "inhaled anesthetics"
Finding Sources
Finding Sources
Searching PubMed
"cerebral autoregulation" AND "volatile anesthetics"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Loading Image
I now have comprehensive information from three major anesthesia textbooks plus two key diagrams. Let me compile the full answer.
Effect of Inhaled Anesthetic Agents on Cerebral Autoregulation
Physiology of Cerebral Autoregulation (Baseline)
Under normal conditions, cerebral blood flow (CBF) is maintained relatively constant across a mean arterial pressure (MAP) range of approximately 50–150 mmHg. This "autoregulatory plateau" is mediated by myogenic, metabolic, and neurogenic mechanisms in the cerebral resistance vessels. All inhaled anesthetics disrupt this relationship to varying degrees.
General Principle: Dose-Dependent Impairment
All potent volatile anesthetics impair cerebral autoregulation in a concentration-dependent manner. The mechanism is direct vasodilation of cerebral vascular smooth muscle, which counteracts myogenic autoregulatory tone. As the dose increases:
- The autoregulatory plateau narrows and shifts to the left (lower MAP threshold)
- Both the upper and lower autoregulatory breakpoints are affected
- At high enough doses, autoregulation is completely abolished, and CBF becomes pressure-passive (directly proportional to MAP)
The figures below illustrate this progression:
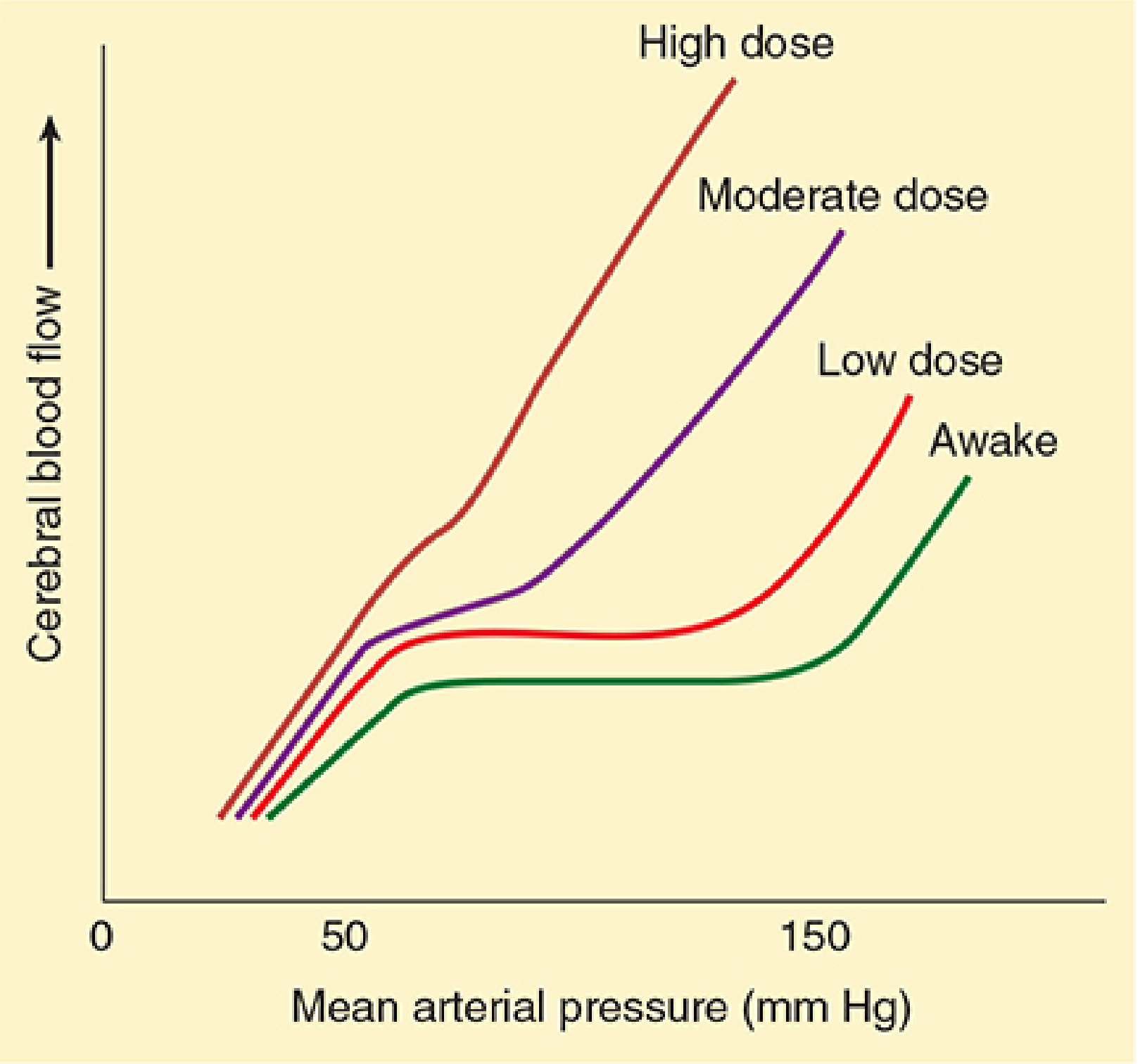
FIGURE: Dose-dependent depression of cerebral autoregulation. The normal autoregulatory plateau (Awake) progressively disappears with increasing volatile anesthetic dose. At high doses, CBF tracks MAP linearly throughout the entire pressure range. — Morgan & Mikhail's Clinical Anesthesiology, 7e
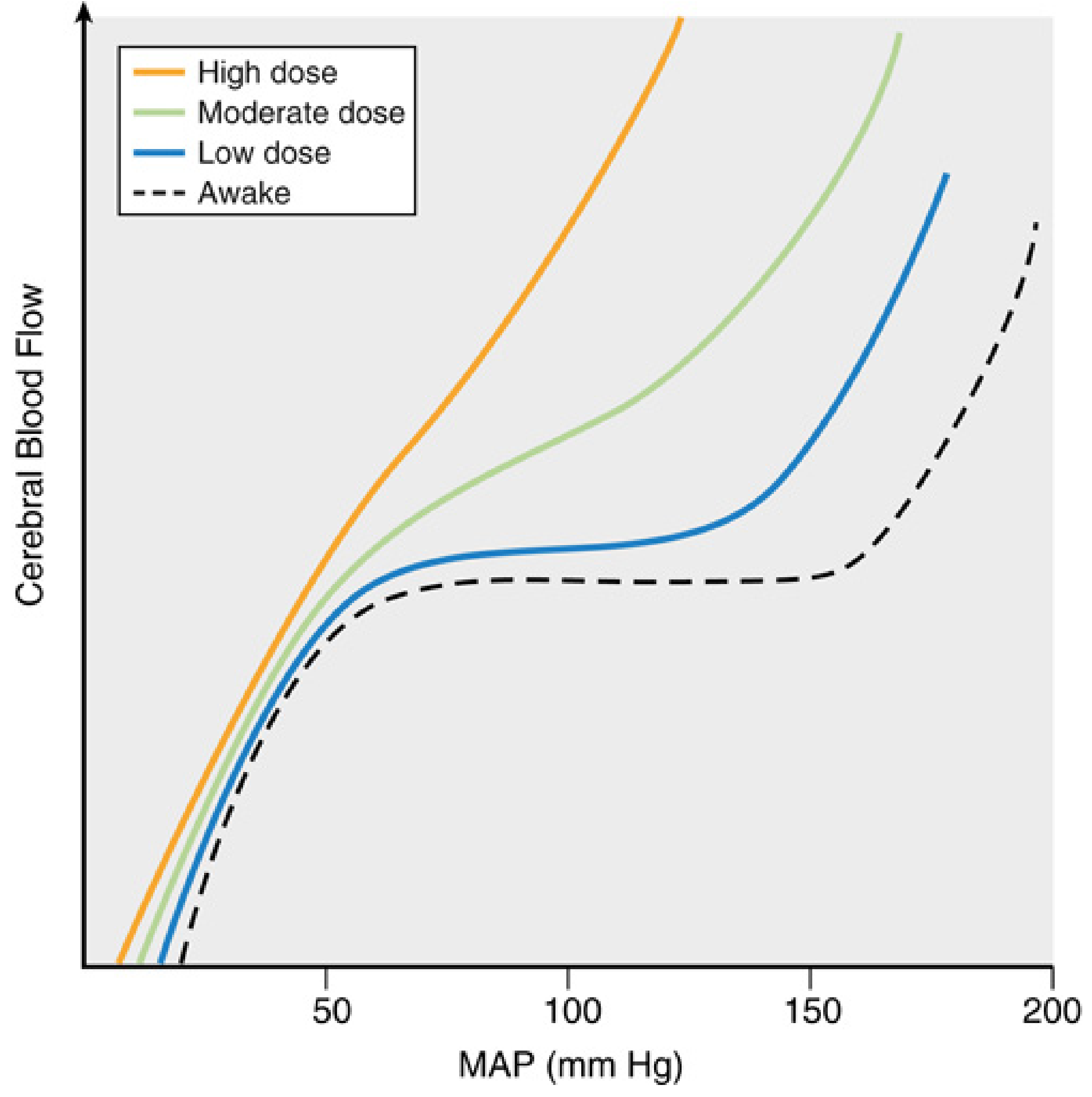
FIGURE: The autoregulatory curve shifts leftward with increasing volatile anesthetic concentration. Both upper and lower thresholds are affected, and the plateau shortens before being abolished entirely. — Miller's Anesthesia, 10e
Agent-by-Agent Comparison
1. Halothane (most potent disruptor)
- Has the greatest cerebrovascular effect of all volatile agents
- At concentrations >1 MAC (>1%), halothane nearly abolishes cerebral autoregulation
- Increases CBF by up to 200% at equivalent MAC compared to isoflurane/desflurane (~20% increase)
- Vasodilation is generalized throughout all brain regions
- CMR depression is relatively limited (≤25% maximal reduction) — less than isoflurane
- Important timing caveat for CO₂ reactivity: hyperventilation (hypocapnia) must be initiated before halothane administration to prevent increases in CBF and ICP. Simultaneous hyperventilation after halothane has already been given is less effective — in contrast to the other agents, where concurrent hyperventilation is effective.
"Halothane has the greatest effect on CBF; at concentrations greater than 1%, it nearly abolishes cerebral autoregulation."
— Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 1088
2. Isoflurane
- Causes far less cerebral vasodilation per MAC-multiple than halothane
- At 0.5 MAC: CMR suppression predominates → net decrease in CBF vs. awake state
- At 1 MAC: CMR suppression and vasodilation are balanced → CBF approximately unchanged
- >1 MAC: Direct vasodilation predominates → CBF increases significantly despite continued CMR reduction ("luxury perfusion")
- Autoregulation is attenuated at 1 MAC and progressively impaired beyond; fully abolished at high doses
- Produces the greatest maximal CMR depression of all volatile agents (up to 50%), allowing EEG burst suppression at clinically tolerated hemodynamic doses
- CO₂ reactivity preserved: hypocapnia can blunt ICP rise when initiated simultaneously
- ICP increases are mild and can be blunted by hyperventilation or barbiturate co-administration
3. Sevoflurane
- Produces the least cerebral vasodilation of the modern volatile agents
- Autoregulation preserved up to approximately 1 MAC
- At 1.5 MAC, dynamic autoregulation (rate of CBF response to rapid transient BP changes) is better preserved with sevoflurane than isoflurane
- CMR depression is similar to isoflurane and desflurane
- CO₂ vasoreactivity is preserved at 1 MAC
- ICP increases are mild (similar to isoflurane and desflurane at equivalent MAC)
- May produce EEG abnormalities (spike-wave activity) with high doses (1.5–2 MAC), especially with hypocapnia or in female patients — raises questions about use in epileptics
- PET studies confirm dose-dependent redistribution of CBF, including increased subcortical/cerebellar flow at 1.5–2 MAC
"Sevoflurane preserves autoregulation up to approximately 1 MAC. At 1.5 MAC, the dynamic rate of autoregulation is better preserved with sevoflurane than isoflurane."
— Barash, Cullen & Stoelting's Clinical Anesthesia, 9e, p. 1415
4. Desflurane
- Cerebrovascular effects broadly similar to isoflurane and sevoflurane per MAC
- At >1 MAC: mild increases in ICP, slightly greater than isoflurane or sevoflurane in some studies
- CO₂ vasoreactivity normal up to 1.5 MAC
- Unique EEG property: desflurane-induced isoelectric EEG (at ~2 MAC in dogs) may revert to continuous activity over time despite unchanged MAC — unique to desflurane
- Airway irritant properties → administration after propofol induction can trigger increases in HR, MAP, and middle cerebral artery flow velocity — likely due to sympathetic activation rather than a direct neurophysiologic effect
- Increases CBF by ~20% at equivalent MAC vs. halothane's ~200%
5. Nitrous Oxide (N₂O)
- Acts as a direct cerebral vasodilator but causes minimal effect on CMRO2 — in sharp contrast to the potent volatile agents (which couple vasodilation to metabolic suppression)
- Effect on cerebral autoregulation is variable; some sources describe it as having a variable/uncertain effect compared to the consistent dose-dependent pattern of the potent agents
- When combined with potent volatile agents, may augment CBF increases
- Does not abolish CO₂ reactivity
Summary Comparison Table
| Agent | CBF Effect | CMR Depression | Autoregulation Impairment | CO₂ Reactivity | Relative Risk at 1 MAC |
|---|---|---|---|---|---|
| Halothane | ↑↑↑ (up to +200%) | Minimal (≤25%) | Nearly abolished at >1% | Preserved (timing-sensitive) | Highest |
| Isoflurane | ↑ at >1 MAC (~20%) | Maximal (up to 50%) | Progressive; abolished at high dose | Preserved | Moderate |
| Desflurane | ↑ similar to isoflurane | Similar to isoflurane | Similar to isoflurane | Preserved to 1.5 MAC | Moderate |
| Sevoflurane | Least of volatile agents | Similar to isoflurane | Best preserved; intact to ~1 MAC | Preserved at 1 MAC | Lowest |
| Nitrous oxide | ↑ (direct vasodilator) | Minimal | Variable | Preserved | Low–Moderate |
Underlying Mechanisms
The net effect of volatile anesthetics on CBF represents a balance between two opposing actions:
- CMR suppression → coupled reduction in CBF (flow-metabolism coupling is maintained, not abolished)
- Direct cerebral vasodilation → CBF increase independent of metabolism
At low doses (0.5 MAC), mechanism 1 dominates → CBF decreases. At 1 MAC, they balance. Above 1 MAC, mechanism 2 dominates → increasing CBF/CMRO₂ ratio ("luxury perfusion"). Autoregulation impairment is the direct consequence of progressive vasodilation overriding myogenic vascular tone.
The cerebrovascular response to CO₂ is retained with all volatile agents, allowing hyperventilation to be used as an adjunct to limit ICP increases — though with halothane, this intervention must precede drug administration.
Clinical Implications
- In elevated ICP states: prefer agents with least cerebrovascular effect; sevoflurane at ≤1 MAC is favored; halothane is contraindicated
- Hyperventilation (targeting PaCO₂ 30–35 mmHg) can blunt volatile-agent-induced CBF increases and is effective for all modern agents (isoflurane, sevoflurane, desflurane) even when used concurrently
- CBV (not CBF per se) determines ICP impact; changes in CBV are proportionally smaller than CBF changes
- Cerebral steal is possible with volatile agents in focal ischemia: increased flow to normal areas may divert blood from ischemic territories where arterioles are already maximally dilated
- All three modern potent agents (isoflurane, sevoflurane, desflurane) can be safely used with adjunctive therapies in neurosurgery, with sevoflurane generally preferred for its favorable autoregulation profile
Sources:
- Morgan & Mikhail's Clinical Anesthesiology, 7e, pp. 1087–1092
- Miller's Anesthesia, 10e, pp. 1004–1020
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e, pp. 1411–1416
This is a shared conversation. Sign in to Orris to start your own chat.